
Abstract
Objectives:
The National Suicide Prevention Trial was announced by the Australian Government in 2016 and aimed to prevent suicidal behaviour in 12 trial sites (representing a population of ~8 million). This study investigated the early population-level impact of the National Suicide Prevention Trial activity on rates of suicide and hospital admissions for self-harm in comparison to control areas.
Methods:
Relative and absolute differences in monthly rates of suicide and hospital admissions for self-harm were compared in the period after the National Suicide Prevention Trial implementation (July 2017–November 2020) to the period prior to implementation (January 2010–June 2017) in (1) ‘National Suicide Prevention Trial areas’ and (2) ‘Control areas’, using a difference-in-difference method in a series of negative binomial models. Analyses also investigated whether associations for suicide and self-harm rates differed by key socio-demographic factors, namely sex, age group, area socio-economic status and urban–rural residence.
Results:
There were no substantial differences between ‘National Suicide Prevention Trial areas’ and ‘Control areas’ in rates of suicide (2% relative decrease, relative risk = 0.98, 95% confidence interval = [0.91, 1.06]) or self-harm (1% relative decrease, relative risk = 0.99, 95% confidence interval = [0.96, 1.02]), adjusting for sex, age group and socio-economic status. Stronger relative decreases in self-harm only were evident for those aged 50–64 years, high socio-economic status areas, metropolitan and remote geographic areas.
Conclusion:
There was limited evidence that the National Suicide Prevention Trial resulted in reductions in suicide or hospital admissions for self-harm during the first 4 years of implementation. Continued monitoring of trends with timely data is imperative over the next 2–3 years to ascertain whether there are any subsequent impacts of National Suicide Prevention Trial activities.
Introduction
Suicide remains a major public health issue in Australia. It is the leading cause of death among young people aged 15–24 years, and the highest rates are evident among middle-aged males (Australian Bureau of Statistics (ABS), 2020). Suicide rates have not changed substantially over the last 20 years and, if anything, have increased during the past decade (Australian Bureau of Statistics, 2020; Milner and Page, 2017).
Current suicide prevention initiatives have been informed by the 2014 National Mental Health Commission report (National Mental Health Commission (NMHC), 2014), which proposed the devolution of suicide prevention funding from national to local area organisations. In Australia, the relevant local area organisations are Primary Health Networks (PHNs). Thirty-one PHNs were established across Australia in 2015, and these organisations are responsible for the planning and commissioning of primary health services, including mental health services and suicide prevention, for geographically defined catchment areas. The National Mental Health Commission report also called for population-level trials to evaluate suicide prevention activity against objective endpoints (suicide and attempted suicide).
The National Suicide Prevention Trial (NSPT) was funded by the Australian Government and established in June 2016, and aimed to gather evidence and further understanding about which strategies are most effective in preventing suicide at a local level and in at-risk populations. The NSPT was implemented in 12 sites, managed by 11 PHNs (Northern Territory; Brisbane North; North Queensland; Central Queensland, Wide Bay, Sunshine Coast; Western New South Wales; North Coast New South Wales; North Western Melbourne; Tasmania; Country South Australia; Perth South; Country Western Australia), and represented a diverse population base of ~8 million from each state of Australia (Table 1). Under the NSPT, each site selected one or more at-risk populations to focus on and delivered whole-of-population suicide prevention activities. At-risk populations included Aboriginal and Torres Strait Islander peoples; middle-aged men; young people; lesbian, gay, bisexual, transsexual, intersex (LGBTI) people; ex-Australian Defence members and older Australians. Some NSPT sites encompassed the entire PHN geographic catchment, while others centred on particular geographical areas within their catchments. Over the course of the NSPT from 2016 to 2022, participating PHNs undertook an extensive community consultation and planning process, and then commissioned a range of suicide prevention activities based on identified needs and selected focus population groups. Selection of activities was guided by multi-component models, including the Lifespan (Black Dog Institute, 2021) and Alliance Against Depression frameworks (Hegerl et al., 2013). Sites focussing on suicide prevention for Aboriginal and Torres Strait Islander peoples drew on the Aboriginal and Torres Strait Islander Suicide Prevention Evaluation Project (ATSISPEP) findings and principles (Dudgeon et al., 2016). Further information on the process used across the trial for selecting suicide prevention activities is provided in the NSPT final evaluation report (Currier et al., 2022).
National Suicide Prevention Trial Site Primary Health Network (PHN) areas and establishment date.
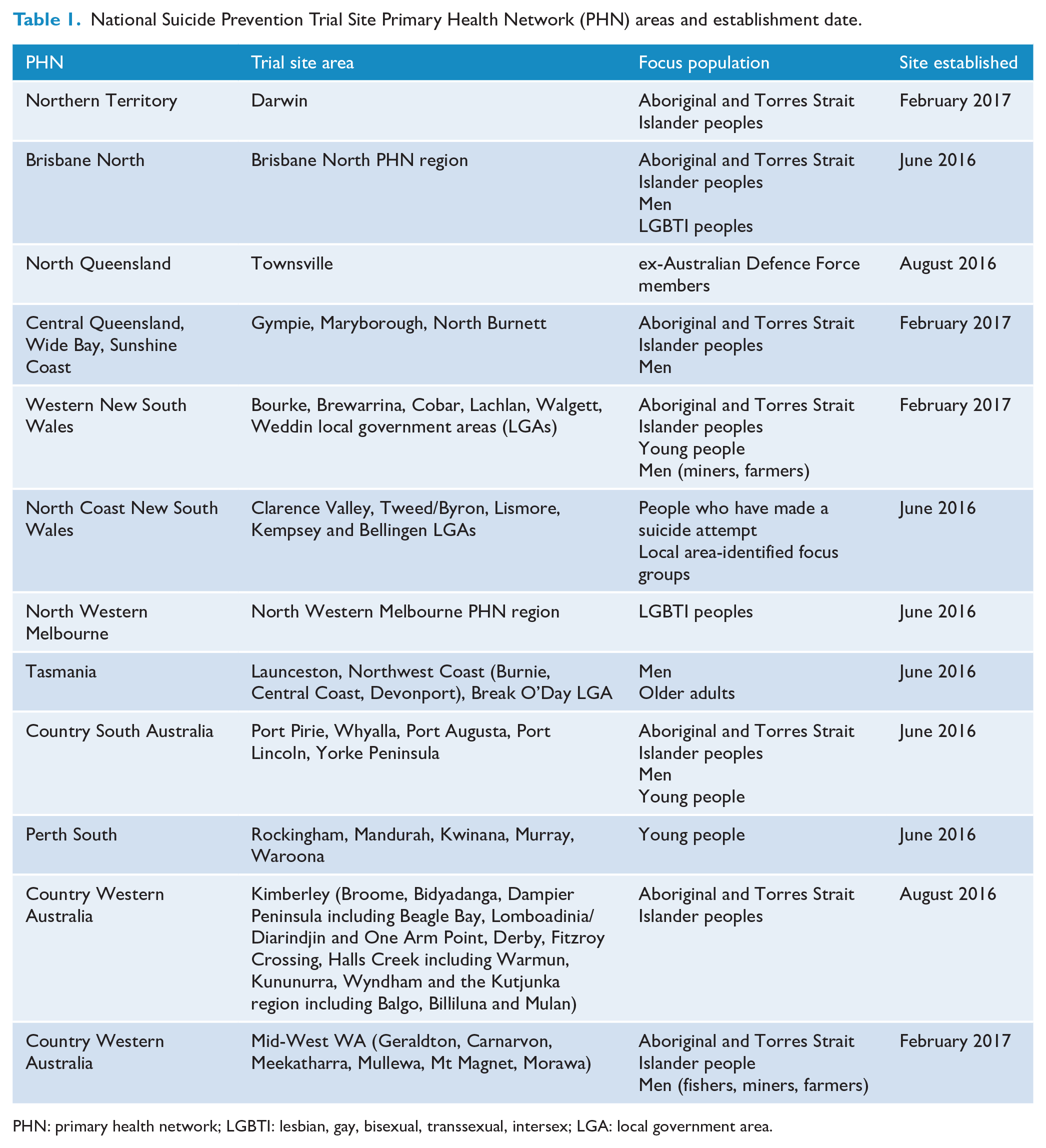
PHN: primary health network; LGBTI: lesbian, gay, bisexual, transsexual, intersex; LGA: local government area.
Four NSPT sites commissioned aftercare services for people who had self-harmed or were experiencing a suicidal crisis (Country South Australia; Brisbane North; Northern NSW; North Western Melbourne), and all NSPT sites commissioned a range of community-based activities. The majority of community-based activities were awareness raising and engagement activities, or capacity building activities, such as training for community members and frontline, health and allied health workers in suicide prevention and/or mental health response. Other types of community-based activities involved providing information or activities for at-risk groups, individuals and the general population, cultural strengthening activities for Aboriginal and Torres Strait Islander peoples and communities, and the development of information resources and care pathways. All NSPT sites also worked to increase integration and coordination among existing suicide prevention services and activity providers in their area. Over the initial 4-year trial period, services and activities were implemented at different times from 2017 to 2020, with additional funding subsequently allocated to continue activities into 2021 due to COVID-19-related disruptions, and then to June 2022 to prepare post-trial transition arrangements.
The current study aimed to investigate the preliminary impact of the NSPT on suicide rates and rates of admission to hospital for self-harm. Specifically, it investigated whether the implementation of the NSPT was (1) associated with subsequent declines in suicide and hospital admissions for self-harm in NSPT sites compared to non-intervention areas; and (2) assess if trends in suicide and hospital admissions for self-harm differed by key socio-demographic sub-populations.
Methods
Data
Suicide data (ICD-10 codes X60–X84) were obtained from the Australian Coordinating Registry for the period January 2010 to December 2020 (the latest available month) and stratified by sex, age group (0–19, 20–34, 35–44, 45–54, 55–64, 65–74, 75+ years), year, month and usual area of residence (Statistical Areal Level 2 [SA2] or Statistical Local Area, resolved to SA2 2016 codes). Self-harm was defined as any hospital admission for self-harm. Data on hospital admissions for self-harm (ICD-10 codes X60–X84) were obtained from the Australian Institute of Health and Welfare (AIHW) for the period January 2010–June 2020 (the latest available month) and stratified in the same strata as suicides. Corresponding annual estimated resident populations for the same period were obtained from the Australian Bureau of Statistics (ABS) (ABS.Stat Beta, 2020) with monthly stratum-specific population counts calculated via weighted interpolation.
For both suicide and self-harm, the usual area of residence was used to determine individuals’ area-based socio-economic status, urban–rural residence and PHN. Socio-economic status (SES) was based on the Socio-economic Indexes for Areas (SEIFA) (Australian Bureau of Statistics, 2018), and each usual area of residence was categorised into area-based quintiles based on Index of Relative Socio-economic Advantage and Disadvantage (IRSAD) scores. Similarly, urban–rural residence was also defined by assigning each usual area of residence, a score based on the ABS Remoteness Area index, categorising areas as either ‘Major City’, ‘Inner Regional’, ‘Outer Regional’, ‘Remote’ or ‘Very Remote’. Finally, each usual area of residence was assigned to its corresponding PHN, based on ABS concordance files mapping SA2 codes to PHN codes. Thus, for each stratum of sex, age group, year, month and usual area of residence (SA2), a corresponding category of SES quintile, Remoteness Area code and PHN code was assigned.
Definition of intervention groups
Two groups were defined for analysis: ‘NSPT areas’ (whole or sub-regions of the PHN as described in Table 1) and ‘Control areas’. ‘Control areas’ were 11 PHNs where there was no formal implementation of suicide prevention trial activity either as part of the NSPT or other contemporaneous suicide prevention initiatives, as described below, but where local commissioning of mental health and suicide prevention services may have occurred in the context of funds provided to all PHNs for suicide prevention. These ‘Control areas’ included Central and Eastern Sydney, Northern Sydney, Western Sydney, Nepean Blue Mountains, South West Sydney, Brisbane South, Gold Coast, Darling Downs and West Moreton, Western Queensland, Adelaide and Perth North.
During the period of implementation of the NSPT, there was also a range of contemporaneous suicide prevention initiatives occurring in the remaining PHNs (that is, those not categorised as ‘NSPT areas’ or ‘Control areas’), including the Lifespan trial at five sites in NSW and the Australian Capital Territory (ACT) (Shand et al., 2020), and the Victorian Place-Based Suicide Prevention Trials in six PHNs (Victorian State Government, 2017). Both of these initiatives were localised, multi-component interventions and were generally based within PHNs. These remaining ‘other trial type’ areas were excluded from the current analysis to allow a direct comparison between the areas implementing the NSPT with areas employing the ‘usual’ approach to suicide prevention. PHNs excluded from analyses were South Eastern NSW; Hunter New England and Central Coast; Murrumbidgee; Eastern Melbourne; South Eastern Melbourne; Gippsland; Murray; Western Victoria and Australian Capital Territory.
As indicated in Table 1, the timing of the onset of NSPT suicide prevention activity differed by participating PHNs, with planning commencing over a period spanning June 2016 to July 2017 and with commissioned activities not commencing until at least 12 months after this start date. For ‘Control areas’, a comparison period also needed to be defined. It was assumed that if there were any impacts of NSPT activities, that these would occur following initiation in the first PHN site, which was June 2016. As noted above, ‘NSPT areas’ and ‘Control areas’ were also stratified by key socio-demographic strata (sex, age, SES and urban–rural residence), given the different focus among some PHNs on specific sub-populations.
Data analysis
Monthly age-standardised rates (per 100,000) for both suicide and hospital admissions for self-harm were investigated for the period January 2010–November 2020 (for suicide) and January 2010–June 2020 (for attempted suicide), stratified by trial site status (‘NSPT areas’, ‘Control areas’) and sex. To evaluate the impacts of the NSPT, the relative difference in suicide and self-harm rates between ‘NSPT areas’ and ‘Control areas’ was investigated using a difference-in-difference method in a series of negative binomial models, modelling counts of suicide or attempted suicide in each SA2 (offset by the logarithm of the population), adjusting for sex, age group, SES, year and month. This approach compared the relative difference in rates of suicide and rates of self-harm in the period after the NSPT implementation (for each PHN-specific start date) to the period prior to implementation in (1) ‘NSPT areas’ and (2) ‘Control areas’. The incidence rate ratio (IRR) of the relative difference in the outcome between ‘NSPT areas’ and ‘Control areas’ was presented, and was derived from each model’s intercept term, the main effect of the intervention group (‘NSPT trial areas’ or ‘Control areas’), the main effect of the period (pre- and post-implementation of the NSPT) and the interaction term between the intervention group and the period, using the lincom function in Stata Version 15.1 (StataCorp LLC, 2019).
The ‘period after the NSPT establishment’ was lagged for 12 and 24 months for both suicide and self-harm, acknowledging that there was likely a scale-up period between onset and full implementation in NSPT trials sites. Additional analyses also investigated whether the association between NSPT implementation and suicide and self-harm rates differed by key socio-demographic factors, namely sex, age group (0–19, 20–34, 35–44, 45–54, 55–64, 65–74, 75+ years), area SES (population quintiles categorised as low [20%], middle [60%] and high [20%]) and urban–rural residence (‘Major City’, ‘Inner Regional’, ‘Outer Regional’, ‘Remote’ or ‘Very Remote’).
Results
Suicide
There were no substantial differences in age-standardised suicide rates between ‘NSPT areas’ and ‘Control areas’, for males or females, and the rate of suicide remained reasonably stable over time (Figure 1). In ‘NSPT areas’, the average suicide rate per 100,000 for males prior to the intervention period was 17.9 (ranging from 8.2 to 31.4) and was 18.9 (ranging from 8.8 to 27.0) during the intervention period. For females, the average suicide rate per 100,000 prior to the intervention period was 5.4 (ranging from 1.2 to 10.5) and was 6.4 (ranging from 2.5 to 10.5) during the intervention period.
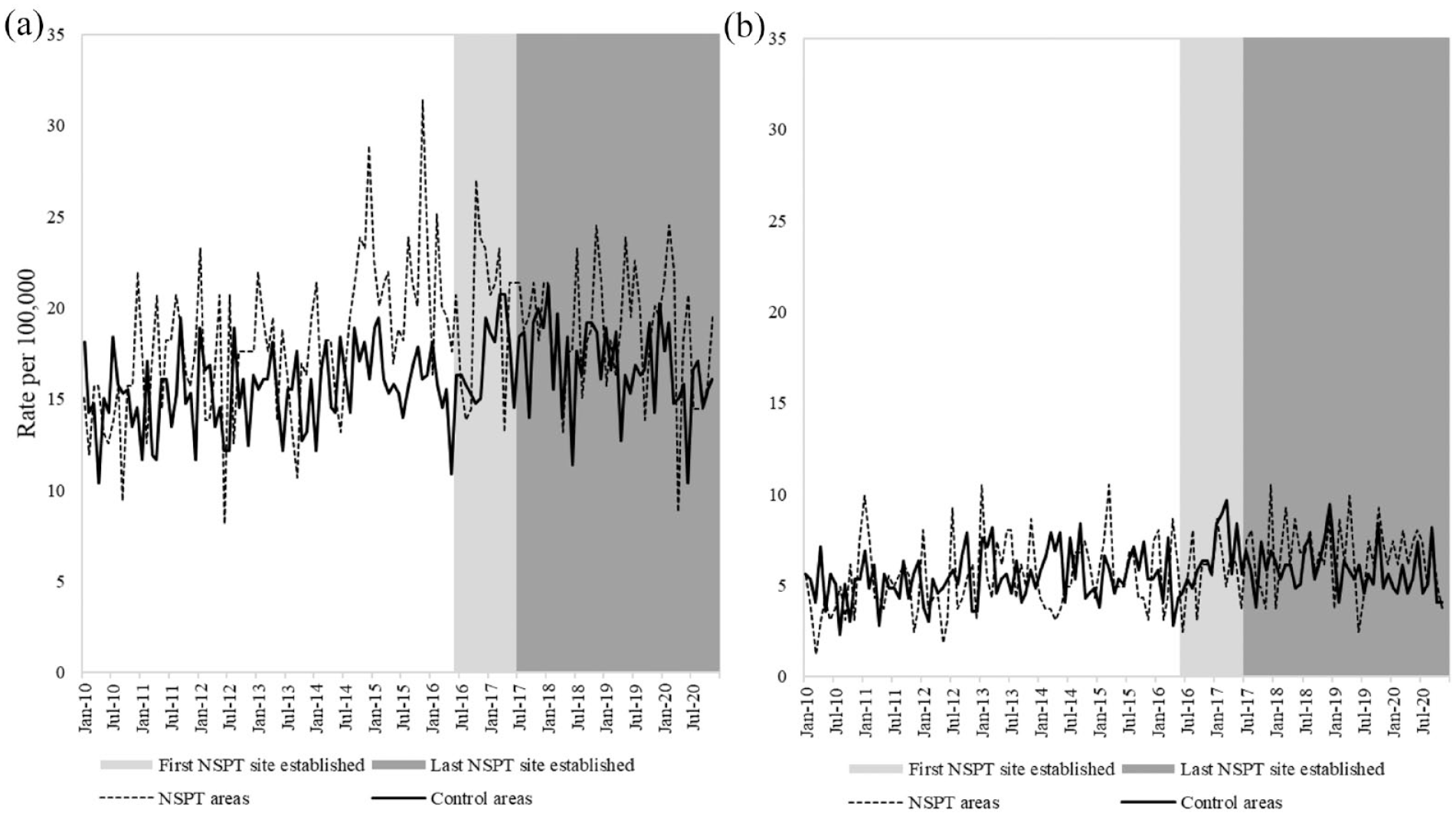
Age-standardised suicide rates per 100,000 by sex and area (‘NSPT areas’ and ‘Control areas’), January 2010–November 2020: (a) males and (b) females.
In ‘Control areas’, the average suicide rate for males prior to the intervention period was 15.4 (ranging from 10.4 to 19.4) and was 16.9 (ranging from 10.4 to 19.4) during the intervention period. For females, the average suicide rate per 100,000 prior to the intervention period was 5.4 (ranging from 2.3 to 8.4) and was 6.0 (ranging from 3.8 to 9.7) during the intervention period.
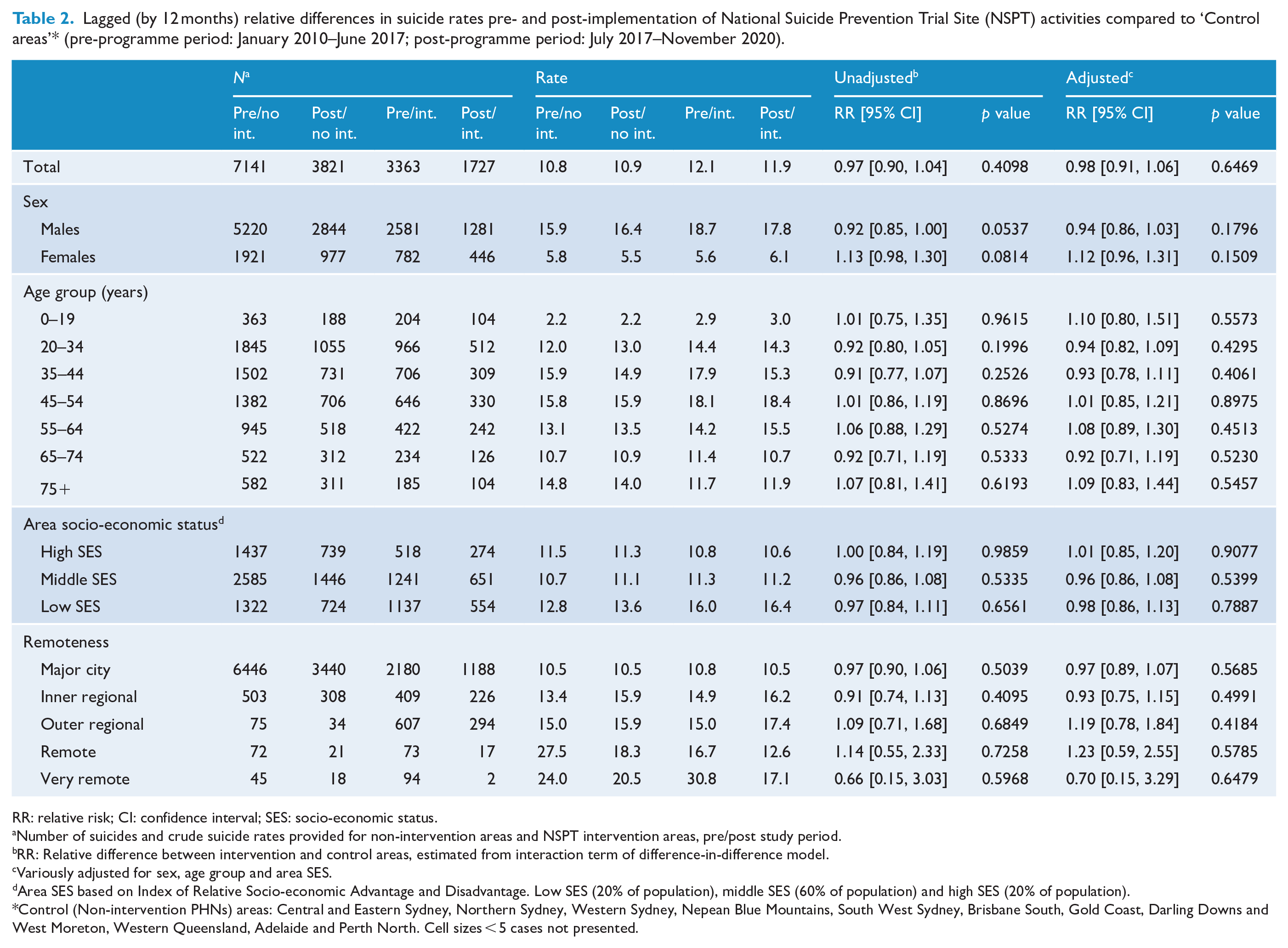
There were also few substantial differences in models investigating the relative difference in suicide rates between intervention and non-intervention areas (Table 2) with a 2% relative decrease (relative risk [RR] = 0.98, 95% confidence interval [CI] = [0.91, 1.06]) for ‘NSPT areas’ (compared to ‘Control areas’), adjusting for sex, age group and SES. Similarly, lagging models by 24 months did not result in any substantial differences in the magnitude of associations (Supplemental Table 1). At a 24-month lag, there was an 0% relative decrease (RR = 1.00, 95% CI = [0.92, 1.09]) for ‘NSPT areas’ (compared to ‘Control areas’), adjusting for sex, age group, SES and period (year and month).
Lagged (by 12 months) relative differences in suicide rates pre- and post-implementation of National Suicide Prevention Trial Site (NSPT) activities compared to ‘Control areas’* (pre-programme period: January 2010–June 2017; post-programme period: July 2017–November 2020).
RR: relative risk; CI: confidence interval; SES: socio-economic status.
Number of suicides and crude suicide rates provided for non-intervention areas and NSPT intervention areas, pre/post study period.
RR: Relative difference between intervention and control areas, estimated from interaction term of difference-in-difference model.
Variously adjusted for sex, age group and area SES.
Area SES based on Index of Relative Socio-economic Advantage and Disadvantage. Low SES (20% of population), middle SES (60% of population) and high SES (20% of population).
Control (Non-intervention PHNs) areas: Central and Eastern Sydney, Northern Sydney, Western Sydney, Nepean Blue Mountains, South West Sydney, Brisbane South, Gold Coast, Darling Downs and West Moreton, Western Queensland, Adelaide and Perth North. Cell sizes < 5 cases not presented.
Associations differed by selected socio-demographic factors in the period prior to implementation compared to post-implementation in ‘NSPT areas’ (compared to ‘Control areas’). Relative decreases appeared to be stronger among younger age groups (20–44 years) and those aged 65–74 years, and in ‘very remote’ areas, although these differences were not statistically significant.
Hospital admissions for self-harm
There were also no substantial differences in age-standardised self-harm rates between ‘NSPT areas’ and ‘Control areas’, for males or females (Figure 2). The rate of hospital admissions for self-harm remained reasonably stable over time, with a slight decline in the most recent period among females (Figure 2). In ‘NSPT areas’, the average self-harm rate per 100,000 for males prior to the intervention period was 88.0 (ranging from 63.1 to 105.6) and was 86.2 (ranging from 62.5 to 120.1) during the intervention period. For females, the average self-harm rate per 100,000 prior to the intervention period was 151.1 (ranging from 111.2 to 187.8) and was 153.5 (ranging from 123.2 to 197.9) during the intervention period.
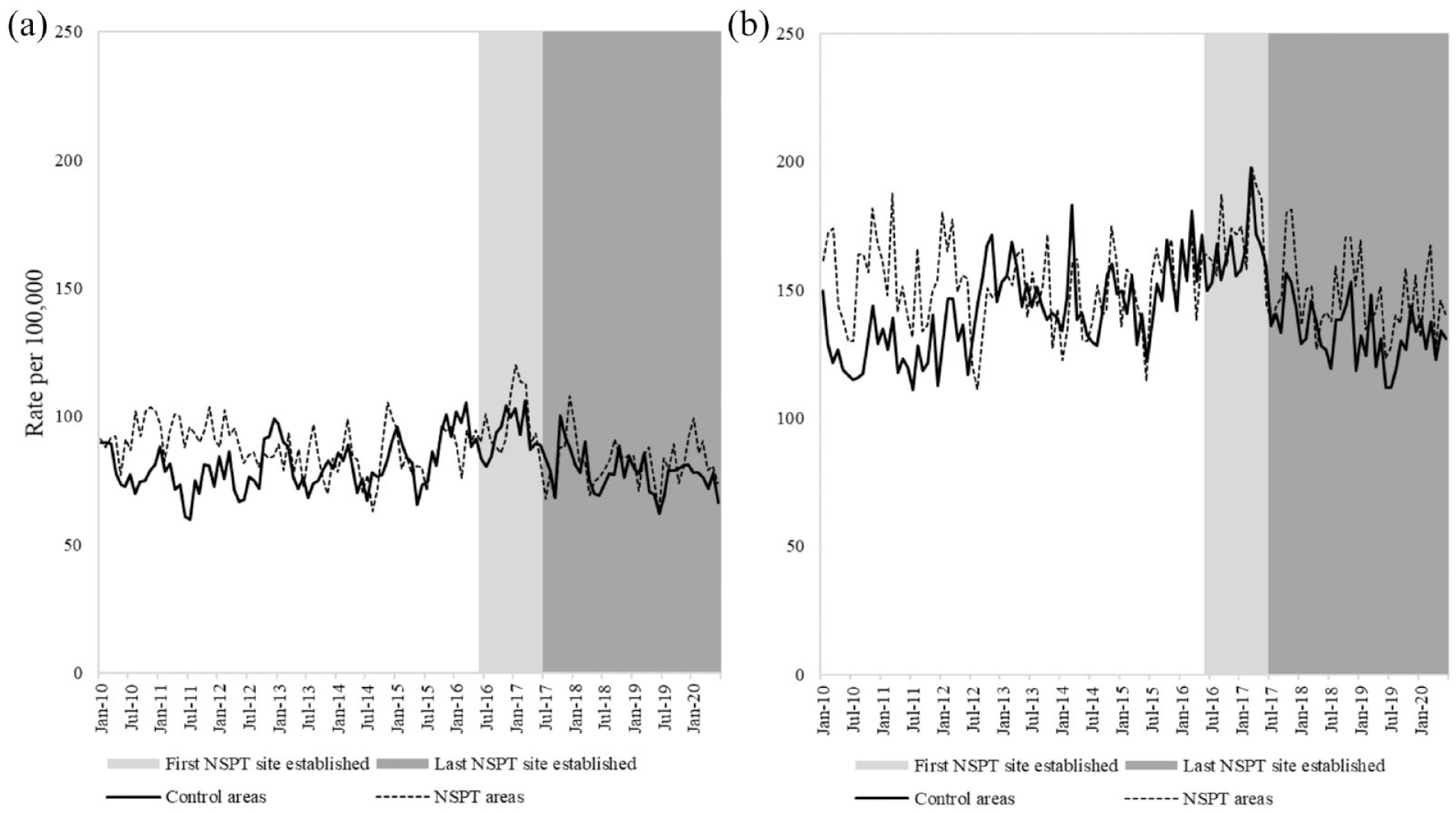
Age-standardised rates of hospital admissions for self-harm per 100,000 by sex and area (‘NSPT areas’ and ‘Control areas’), January 2010–June 2020: (a) males and (b) females.
In ‘Control areas’, the average rate for hospital admissions for self-harm for males prior to the intervention period was 80.8 (ranging from 59.6 to 105.2) and was 82.1 (ranging from 62.2 to 106.3) during the intervention period. For females, the average self-harm rate prior to the intervention period was 140.5 (ranging from 110.9 to 183.1) and was 141.4 (ranging from 111.7 to 197.4) during the intervention period.
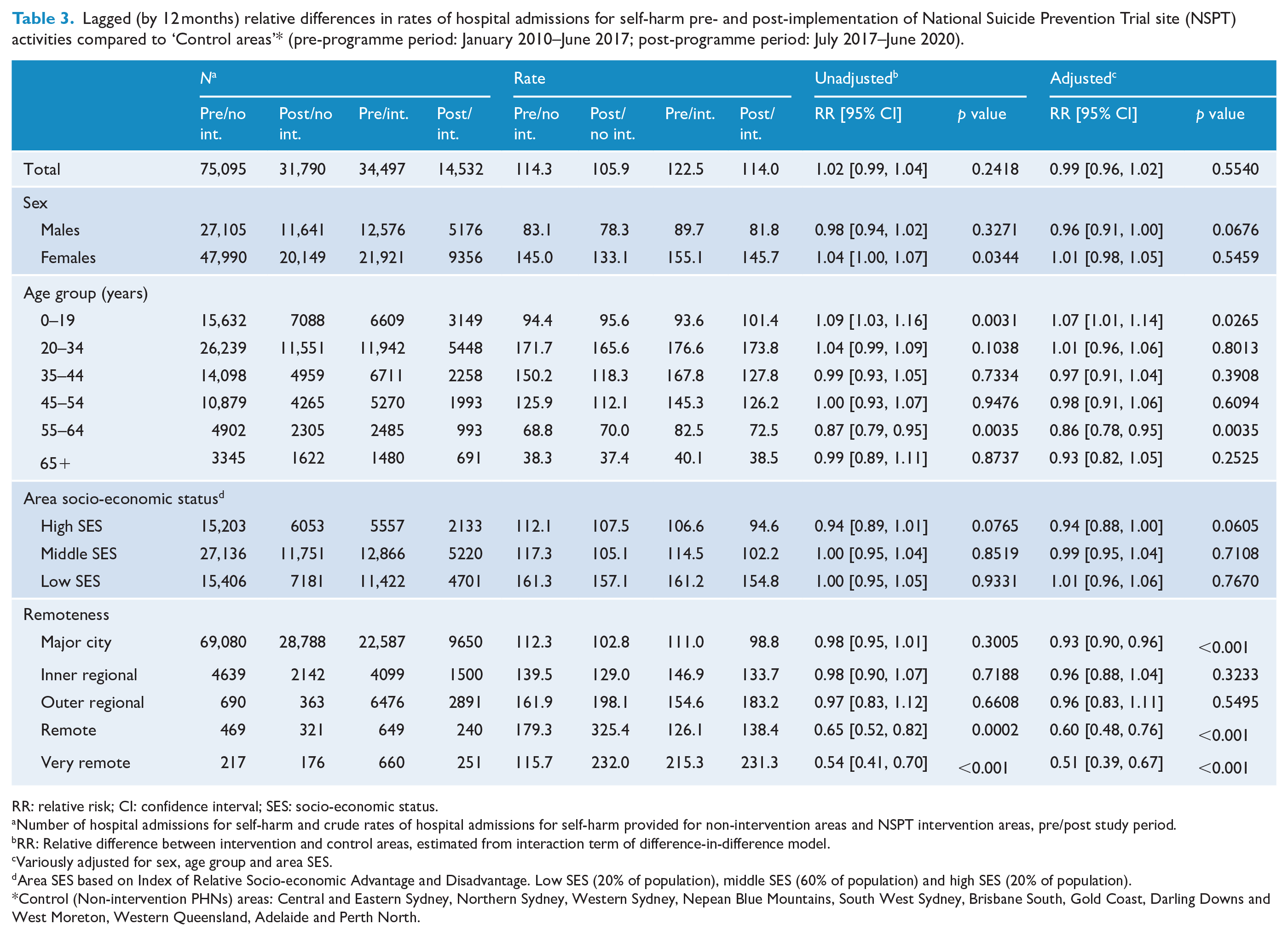
There were also few substantial differences in models investigating the relative difference in self-harm rates between intervention and non-intervention areas (Table 3), with a 1% relative decrease (RR = 0.99, 95% CI = [0.96, 1.02]) for ‘NSPT areas’ (compared to ‘Control areas’), adjusting for sex, age group and SES. Similarly, lagging models by 24 months did not result in any substantial differences in the magnitude of associations (Supplemental Table 2). At a 24-month lag, there was an 1% relative increase (RR = 1.01, 95% CI = [0.97, 1.04]) for ‘NSPT areas’ (compared to ‘Control areas’), adjusting for sex, age group, SES and period (year and month).
Lagged (by 12 months) relative differences in rates of hospital admissions for self-harm pre- and post-implementation of National Suicide Prevention Trial site (NSPT) activities compared to ‘Control areas’* (pre-programme period: January 2010–June 2017; post-programme period: July 2017–June 2020).
RR: relative risk; CI: confidence interval; SES: socio-economic status.
Number of hospital admissions for self-harm and crude rates of hospital admissions for self-harm provided for non-intervention areas and NSPT intervention areas, pre/post study period.
RR: Relative difference between intervention and control areas, estimated from interaction term of difference-in-difference model.
Variously adjusted for sex, age group and area SES.
Area SES based on Index of Relative Socio-economic Advantage and Disadvantage. Low SES (20% of population), middle SES (60% of population) and high SES (20% of population).
Control (Non-intervention PHNs) areas: Central and Eastern Sydney, Northern Sydney, Western Sydney, Nepean Blue Mountains, South West Sydney, Brisbane South, Gold Coast, Darling Downs and West Moreton, Western Queensland, Adelaide and Perth North.
Associations differed by selected socio-demographic factors in the period prior to implementation compared to post-implementation in ‘NSPT areas’ (compared to ‘Control areas’) (Table 3). Relative decreases were stronger among males (RR = 0.96, 95% CI = [0.91, 1.00]), in high SES areas (RR = 0.94, 95% CI = [0.88, 1.00]), among those aged 55–64 years and in metropolitan and remote geographic areas. A relative increase was evident for those aged 0–19 years (RR = 1.07, 95% CI = [1.01, 1.14]).
Discussion
This analysis found limited preliminary impacts of suicide prevention activity on either suicide rates or hospital admissions for self-harm rates in ‘NSPT areas’ compared to ‘Control areas’. Overall, there were very few differences between ‘NSPT areas’ and ‘Control areas’, with perhaps the exception of relative decreases in hospital admissions for self-harm among males, high SES areas, and metropolitan and remote geographic areas.
There are a number of methodological considerations in the current study. A key strength of the analysis is the use of small-area codes, stratified by key socio-demographics, allowing detailed analyses within, and between, ‘NSPT areas’ and ‘Control areas’ over time. This partial ecological design allowed analyses to capture, and adjust for, some of the heterogeneity within ‘NSPT areas’ and ‘Control areas’ (and within each usual area of residence). While there were geographic coding changes over the study period, these were accounted for to ensure comparability within small areas (in both the numerator and denominator) over the study period. A limitation of resolving small-area codes to SA2 2016 codes, and the use of SEIFA and Remoteness Area codes for the same period, meant that any large changes in SES and urbanisation within small areas over the study period may not have been captured. However, aggregating these small areas into larger strata for analyses would mitigate against misclassification of SES and urban–rural residence over time.
The analysis also covered an extensive period (131 months for suicide and 126 months for attempted suicide), allowing a clear assessment of secular changes in both suicide and hospital admissions for self-harm in the lead up to the NSPT intervention, and during the immediate implementation period. In addition, the analysis examined different lag periods for analyses of hospital admissions for self-harm (given the longer period of available data post-implementation of the NSPT) in an attempt to reflect the differing onset times of activities in different areas.
A key limitation of the analysis is not being able to ascertain what suicide prevention activity might have been implemented contemporaneously in the ‘Control areas’. It is important to note that all PHNs received Australian Government funding for the commissioning of local suicide prevention services and activities, the effect of which might have been to attenuate any differences between NSPT sites and non-intervention sites. It is also possible that there may have been cross-contamination of ‘NSPT areas’ and ‘Control areas’ where PHN sites were geographically adjacent. Based on secular trends in both suicide and self-harm in these ‘Control areas’, there appears to have been little decline in suicide or hospital admissions for self-harm.
Additionally, there are likely to be PHN-specific factors that may have influenced the selection and uptake of particular suicide prevention initiatives that differed between ‘NSPT areas’ and ‘Control areas’, particularly given the lack of randomisation of sites (to either intervention or control areas). The remaining PHNs used as ‘Control areas’ (those areas that were not ‘NSPT areas’, or other areas where contemporaneous suicide prevention trials were implemented) were predominantly metropolitan PHNs and may reflect differential accessibility to relevant services in ‘NSPT areas’ compared to ‘Control areas’. These differences were controlled in analyses by adjusting for urban–rural residence (using the ARIA code for a given SA2); however, this is likely an imperfect proxy measure of access to services in more rural and remote regions of Australia.
This analysis also was not able to ascertain impacts of the NSPT for specific at-risk groups, based on the routinely available suicide and hospital data, particularly people with a mental disorder, Aboriginal and Torres Strait Islander peoples, and people identifying as LGBTI. Although Aboriginal and Torres Strait Islander status is captured in mortality and hospital data, establishing corresponding small-area denominators for this group is problematic. Similarly, there is little routinely collected information in suicide or self-harm data relating to LGBTI identification, or history of current or previous mental illness or substance use to stratify analyses by these sub-groups. Furthermore, the definition of self-harm was limited to individuals admitted to hospital. Individuals presenting to emergency departments for self-harm (but not admitted) and individuals who self-harm within community were therefore not captured in the study, potentially biasing estimates.
The findings of the current study show limited changes in suicide and hospital admissions for self-harm in the period after the establishment of the NSPT. The exception was for apparent decreases in hospital admissions for self-harm among males, higher SES areas and metropolitan areas, although effect sizes were not large (~10% relative risk reduction), and also for remote geographic areas (~40–50% relative risk reduction). It may be that the decline in remote areas is an artefact of the small underlying numbers and the multiple between-group comparisons that were made in analyses. Alternatively, it may be that suicide prevention initiatives were better implemented and targeted to relevant at-risk populations in more remote areas. The qualitative evaluation of the processes associated with the selection and implementation of initiatives in these areas is a priority for future research.
One interpretation of the limited overall changes in suicide and hospital admissions for self-harm is that it is premature to try to ascertain large NSPT impacts based on the currently available follow-up period in the suicide and hospital admissions data. While NSPT areas were funded to begin in 2016–2017, it was not until the second half of 2018 and 2019 when the majority of community-based activities and aftercare services began to be implemented at scale. It may be that the impacts of these prevention activities will not emerge for some time. Previous modelling of the potential impact of the sustained implementation of similar interventions as employed in the NSPT suggests that declines may take 3–5 years to emerge (Page et al., 2017). The implication of this is that continued monitoring of trends in suicide and self-harm with timely data is imperative over the next 2–3 years to ascertain whether there are any subsequent impacts of the NSPT (and other trial) area activities. There are few examples of immediate impacts of suicide prevention activities, with the exception of restricting access to means (Kreitman, 1976; Oliver and Hetzel, 1972; Zalsman et al., 2016), and rapid reductions in alcohol consumption (Razvodovsky, 2011; Wasserman et al., 1994).
It is possible that interventions may be affecting intermediate factors associated with suicidal behaviour (such as social connections, psychological distress, suicidal ideation and health service access), but that changes in these intermediate outcomes are not yet having an impact on objective measures of suicidal behaviour. It may also be possible that interventions targeting specific sub-populations that represent a minority of the population (such as Aboriginal and Torres Strait Islander peoples and people identifying as LGBTI) may have been associated with the prevention of suicidal behaviour, but that these effects were not observable when aggregated over a whole population.
However, it also may be possible that the types of interventions selected in trial sites were not implemented with the appropriate fidelity, or with sufficient resources, or over a sufficiently sustained time period to have general population-level impacts. The majority of initiatives in ‘NSPT areas’ related to awareness raising and engagement activities, or capacity building activities, that took time to implement and scale. An alternative combination of interventions with a greater focus on more distal economic and psychosocial determinants, and corresponding investments in mental health-related services, may have had a greater population-level impact on suicidal behaviour in the short term.
In summary, there was little evidence that the NSPT has resulted in reductions in suicide or hospital admissions for self-harm in the intervention areas, in comparison to non-intervention areas, at least in the preliminary period. There may be some evidence that suicide rates were lower in NSPT trial sites for males and younger age groups, and that hospital admissions for self-harm were lower in NSPT trial sites for males, high SES areas and in metropolitan and remote areas. Overall, both suicide and hospital admissions for self-harm appear not to have changed substantially over this preliminary intervention period. The effects of suicide prevention interventions on suicidal behaviour may take some years to materialise, and continued monitoring of trends in suicide and self-harm with timely data is imperative over the next 2–3 years to ascertain whether there are any subsequent impacts of NSPT activities.
Supplemental Material
sj-docx-1-anp-10.1177_00048674231166330 – Supplemental material for Early impacts of the ‘National Suicide Prevention Trial’ on trends in suicide and hospital admissions for self-harm in Australia
Supplemental material, sj-docx-1-anp-10.1177_00048674231166330 for Early impacts of the ‘National Suicide Prevention Trial’ on trends in suicide and hospital admissions for self-harm in Australia by Andrew Page, Jane Pirkis, Piumee Bandara, Sanne Oostermeijer, Teresa Hall, Philip M Burgess, Meredith Harris and Dianne Currier in Australian & New Zealand Journal of Psychiatry
Footnotes
Author contributions
A.P. led the conception and design of the study, conducted the data analyses and drafted the manuscript. J.P. contributed to the conception and design of the study, provided oversight of evaluation implementation and provided critical revisions of the manuscript. P.B. contributed to study design, data interpretation and critical revision of the manuscript. S.O. contributed to data collection of trial site interventions and critical revisions of the manuscript. T.H. contributed to data collection of trial site interventions and critical revisions of the manuscript. P.M.B. contributed to the conception, design and analytic strategy of the study, and provided critical revisions of the manuscript. M.H. contributed to the conception, design and analytic strategy of the study and provided critical revisions of the manuscript. D.C. contributed to the conception and design of the study, provided oversight of evaluation implementation, contributed to data collection of trial site interventions and study design, obtained the mortality and hospital admissions data, and provided critical revisions of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by the Australian Government Department of Health as part of evaluation of the National Suicide Prevention Trial.
Ethical approval
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees. Ethical approval was obtained from the University of Melbourne Human Research Ethics Committee (HREC 1851745; 2021-12103-15560-3).
Data availability
Data from this study cannot be shared due to Data Custodian Agreements relating to the access and use of unit record hospital admissions and mortality data.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.