
Abstract
Objective:
Heterogeneous brief non-pharmacological interventions and guidelines exist to treat the burgeoning presentations to both emergency department and inpatient settings, for those in a crisis of mental ill-health. We systematically reviewed the literature to create a taxonomy of these brief non-pharmacological interventions, and review their evaluation methods and effectiveness.
Method:
We conducted a systematic review across Cochrane, CINAHL, DARE, Embase, MEDLINE, PsycINFO databases. Studies meeting quality criteria, using Joanna Briggs Institute tools, were eligible. Interventions were categorised, and outcomes synthesised.
Results:
Thirty-nine studies were included: 8 randomised controlled trials, 17 quasi-experimental, 11 qualitative studies, and 3 file audits. Taxonomy produced six coherent intervention types: Skills-focussed, Environment-focussed, Special Observation, Psychoeducation, Multicomponent Group and Multicomponent Individual. Despite this, a broad and inconsistent range of outcome measures reflected different outcome priorities and prevented systematic comparison of different types of intervention or meta-analysis. Few brief non-pharmacological interventions had consistent evidential support: sensory modulation rooms consistently improved distress in inpatient settings. Short admissions may reduce suicide attempts and readmission, if accompanied by psychotherapy. Suicide-specific interventions in emergency departments may improve depressive symptoms, but not suicide attempt rates. There was evidence that brief non-pharmacological interventions did not reduce incidence of self-harm on inpatient wards. We found no evidence for frequently used interventions such as no-suicide contracting, special observation or inpatient self-harm interventions.
Conclusion:
Categorising brief non-pharmacological interventions is feasible, but an evidence base for many is severely limited if not missing. Even when there is evidence, the inconsistency in outcomes often precludes clinicians from making inferences, although some interventions show promise.
Introduction
Background
Psychiatric presentations to emergency departments (EDs) continue to rise (Hill et al., 2021; Holland et al., 2021; Sara et al., 2022), leading to challenges related to ‘boarding’ in the ED that have proven difficult to address (Nordstrom et al., 2019; Zun, 2012). Many EDs rely heavily on ED staff to manage these presentations; however, various alternative system approaches have emerged (Coates, 2018; Fitz-Gerald and Takeshita, 2020). In Australia, one common model involves short-stay emergency psychiatric wards situated either adjacent to or within the ED. These wards are staffed with specialised psychiatric teams responsible for serving both the ED and the short-stay ward, known in Australia as Psychiatric Emergency Care Centres (Frank et al., 2005; Seymour et al., 2020) or Psychiatric Assessment and Planning Units (Mitchell et al., 2020). Similar services, known as Psychiatric Emergency Services (Haack et al., 2020), have been established in the United States, and the United Kingdom is also starting to adopt them (Sampson et al., 2022). Research supports their effectiveness in reducing the length of stay (LOS) in the ED (Anderson et al., 2022). Importantly, these units differ from outpatient or ‘partial programme’ settings, as they focus on brief admissions before either discharging to the community or transferring to longer-stay wards. These service models also offer the opportunity to ensure ethical, efficient and effective care by initiating psychiatric treatment within the ED and possibly continuing it through to the short-stay inpatient space.
Of course, effective care is vital not only to ensure efficiency. Central to our understanding are the people who are reaching out for help. People presenting to EDs may experience interpersonal, environmental, and system-related factors (Navas et al., 2022) that impact their willingness to return to EDs (Rosebrock et al., 2022). If we are to provide excellent person-centred care, we must understand how the ED and inpatient spaces can be used in an evidence-based way.
The specific brief interventions used in this population and setting can be broadly thought of as pharmacological (e.g. sedation) and non-pharmacological interventions (NPI). There are systematic reviews that evaluate brief pharmacological treatment for mental health crises in the ED showing, e.g., that ketamine, droperidol and midazolam are the safest options for managing severe agitation (deSouza et al., 2022). There are systematic reviews of longer-term NPIs started in the ED that are then continued in the outpatient setting, despite the very great differences between environments (Chaudhary et al., 2020; Johnston et al., 2019; McCabe et al., 2018; Ougrin et al., 2012; Wilson et al., 2020) which indicate that NPIs such as green or gold card clinics and postcards to people after self-harm attempts may show potential in reducing suicide and suicide attempts. Other reviews have evaluated environmental interventions in the ED (MohammadiGorji et al., 2021) showing that environment plays a central role in mitigating aggression, service-wide interventions (Baker et al., 2021) showing great need for better systems to manage restrictive practices, psychological therapies on adult inpatient units (Jacobsen et al., 2018) showing that inpatient research lacks rigour and organisation, and the evidence for environment, policy and practice changes addressed acute severe behavioural disturbance in the ED (Weiland et al., 2017) demonstrating a deficit in research surrounding acute severe behavioural disturbance.
However, a critical gap remains in systematic advice concerning brief non-pharmacological interventions (bNPIs) that could be offered by psychiatric teams across both the ED/short-stay inpatient environments, meaning that the goals and effectiveness of bNPIs that are delivered within a very brief timeframe remain largely unexplored. This is of clinical significance because so many clinicians work across this interface (Coates, 2018; Evans et al., 2019), particularly in Australia. Furthermore, an appraisal of international guidelines for emergency mental health care in hospital settings written 21 years ago (Allen et al., 2002; National Institute for Health and Care Excellence (NICE), 2022) emphasised the need for such a review. Peak bodies urge ‘a written protocol that specifies the most effective and least restrictive approaches to common behavioural emergencies seen in the [emergency] service’(Allen et al., 2002: 23), and that a ‘psychological intervention that is specifically tailored for adults who self-harm’ should be provided in an environment where ‘healthcare staff should be appropriately trained . . . in the therapy they are offering’(NICE, 2022: 33). Without an understanding of the underpinning evidence, such guidelines cannot be followed consistently. Given over 20 years have elapsed since this first call for evidence, it is critical this is now addressed. With steadily increasing service demand, Australian ED and short-stay inpatient units are flying blind.
For this area of study to progress, a clear ‘map’ of crisis interventions that can be ‘specifically tailored’ in these environments is imperative. This will enable a comprehensive understanding of which interventions are needed for which person and at what time (Kleiman et al., 2022), and ensure the ED and ward environments are used as efficiently as possible (Kleiman and Nock, 2020). This may give rise to interventions that can be brought from the inpatient to the ED space, and vice versa. To date, a systematic review of this scope has not been conducted, possibly because (1) bNPIs are highly heterogeneous, making this an ambitious project, and (2) Emergency Psychiatry is not yet ‘organised’ as a treatment group in the same way as other areas of psychiatry. Nonetheless, as a starting point, we must have the evidence summarised, synthesised and organised so that a path forward may be established.
Objectives
To systematically review the evidence for brief NPIs in EDs and psychiatric inpatient units by:
Creating a taxonomy of these interventions;
Appraising and synthesising outcome measures used to evaluate them; and,
Systematically reviewing their effectiveness.
Methods
Protocol and registration
This review was registered with PROSPERO (CRD42021287496).
Criteria for considering studies for this review
Randomised controlled trials (RCTs), non-RCTs, cohort and case–control studies, case series and case reports, surveys and qualitative studies were included. We planned to include non-randomised studies because of the expected dearth in RCTs (Johnston et al., 2019), even though this increases the risk of bias. We included qualitative studies because these help guide and interpret quantitative data. See Supplementary S1 for PRISMA flowchart and checklist. Risk of bias was measured using Joanna Briggs Institute Risk of Bias Checklists, with a plan to exclude high-risk studies.
Selection criteria
Population
Study participants were persons who were in crisis of mental ill-health. There is no standard definition of in crisis in the literature, thus we defined participants as being in crisis when they were presenting to ED with any complaint related to mental or behavioural health, or an inpatient on a psychiatric ward having self-harm thoughts/behaviours or agitation/aggression. This definition reflects the nature of crisis as time-limited and where an important change has occurred. Studies of interventions for people solely with drug- and alcohol-related presentations were excluded.
Interventions
All primarily brief NPIs aimed at addressing psychiatric complaints were included. Incidental medication use was not an exclusion criterion, but studies were excluded if medications were identified as a component of the intervention being evaluated. Given the short duration of admissions to crisis units, we excluded interventions that were longer than 1 week. Interventions that were used during crisis admissions, even if they were not used on a crisis unit, were included. We excluded seclusion and restraint-only papers but a priori included papers (and stratified results accordingly) where other bNPIs were used. We included solely clinical interventions, rather than processes of care pathways.
Treatment setting
We included studies that described treatment within EDs or psychiatric wards, including those that started in the ED and continued in inpatient settings. We excluded interventions that were commenced in the ED and continued in outpatient settings, e.g., brief courses of therapy because reviews of these already exist (Chaudhary et al., 2020; Johnston et al., 2019; McCabe et al., 2018; Ougrin et al., 2012; Wilson et al., 2020). We excluded bNPIs conducted on non-psychiatric (medical) wards; although these patients may well be in crisis, we expected that the interventions would be different due to the lack of mental health trained staff. We excluded studies conducted in aged care facilities, group homes, jails and other non-hospital settings.
Outcome measures
We included papers with either quantitative or qualitative analysis. No outcome measures were excluded.
Articles
Articles were those written in English, in peer-reviewed journals, without date restriction. Searches were performed between 25 August 2021 and 8 December 2021, and again on 7 September 2022. Studies not yet complete were excluded.
Search methods
The database search was carried out by one researcher in Cochrane Central Register of Controlled Trials (CENTRAL), CINAHL, DARE, Embase, MEDLINE and PsycINFO, and peer reviewed by a librarian specialising in systematic reviews. Search criteria for each database are found in Supplementary S2. We excluded all evidence syntheses, expert opinion and descriptive studies; the reference lists of the former were hand-searched. Researchers also reviewed government health websites, including UK NHS, Canada, NZ and USA for references, plus key non-government organisation crisis resources for relevant articles.
Method of inclusion/exclusion
All studies were title screened by one author (J.P.H.). Four authors then reviewed abstracts of all screened inclusions, and conducted full text reviews, with each paper being reviewed by two authors independently for content and quality (J.P.H., M.C.B., L.M.N. and S.M.H.). When disagreement arose, authors discussed inclusion versus exclusion explicitly. This was particularly the case when differentiating between ‘service’ and ‘clinical’ interventions, as many interventions take into account the structure, staffing, models of care and care pathways. These studies were discussed at length and disputes adjudicated by A.M. and N.G.
Data extraction and management
One author (J.P.H.) systematically extracted data from all papers using Covidence and Microsoft Excel. Two authors (L.M.N. and M.C.B.) independently extracted the data and checked it against the original author’s data.
The Cochrane Handbook for Systematic Reviews of Interventions (Higgins et al., 2019) and the JBI Manual Evidence Synthesis Chapter 8: Mixed methods systematic reviews (Lizarondo et al., 2020) guided the process of data extraction and management. We piloted a data extraction form in Covidence using a pre-specified tabular format. Supplementary Table 2 shows itemised data for each paper after piloting multiple data collection formats. If data were missing, the authors were contacted in order of authorship. Data extraction was first conducted on 15 December 2021.
Intervention taxonomy
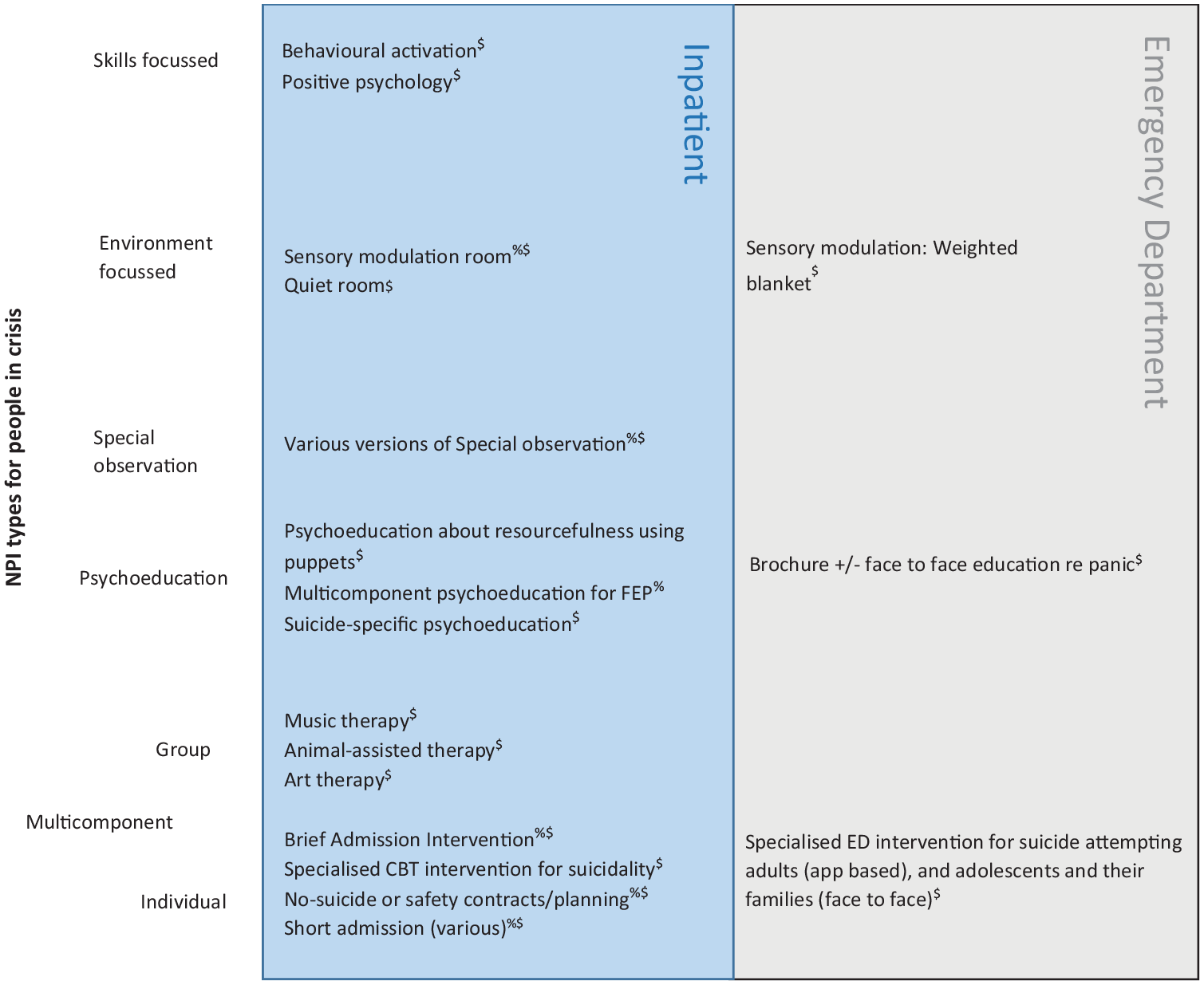
There was a high level of clinical heterogeneity of NPIs. To organise the interventions in a way that is helpful for clinicians, and potentially allow for data synthesis, the interventions were classified into a taxonomy. Multiple iterations of this taxonomy were discussed by three authors (J.P.H., N.G. and A.M.). The ‘Categories’ were created to provide a structure by which to understand the focus, form and content of the intervention, on the premise that similar interventions are expected to have similar theories of change. There was no a priori specific grouping of intervention prior to extracting the data. After being classified into Categories, similar interventions were then further grouped into intervention ‘Types’ (Supplementary Table 3 and Figure 1).
Taxonomy of NPIs found in EDs and inpatient units for people in crisis. Measures of treatment effect.
Data were selected for reporting:
If there was a primary outcome defined in the paper, this was used;
If no primary outcome was reported, then any outcome used consistently across studies within each category;
If an effect size was reported in the paper, this was extracted;
If no effect size was reported, then effect size was calculated where possible.
Effect size types reported by papers assessing quantitative outcomes include partial η2, Cohen’s d and odds ratios (ORs). Effect size types calculated by the authors of this paper include Cohen’s d and ORs. For continuous data, Cohen’s d was calculated by subtracting the means of the two groups and dividing by the pooled standard deviation (SD) (Lenhard and Lenhard, 2016). For groups of different sample sizes, the pooled SD was adjusted with weights for the sample sizes (Lenhard and Lenhard, 2016). For categorical data, ORs were calculated. The data used for calculation of effect sizes are presented in Supplementary Table 4. There were insufficient data to perform a sensitivity analysis.
The intervention types that were deemed to be similar were grouped and analysed together.
Results
Included studies
Thirty-nine studies met inclusion criteria. Eight studies were RCTs, 17 were quasi-experimental, 11 were qualitative, and 3 were file audits. Thirteen studies were high quality (Tables 1–6) but no interventions had sufficient data to allow for meta-analysis. To aid understanding of upcoming sections, readers should repeatedly refer to Figure 1.
PICO table of ‘Skills-focussed’ intervention category. Studies are ordered by study type (randomised controlled trial, quasi-experimental) and date (most to least recent).
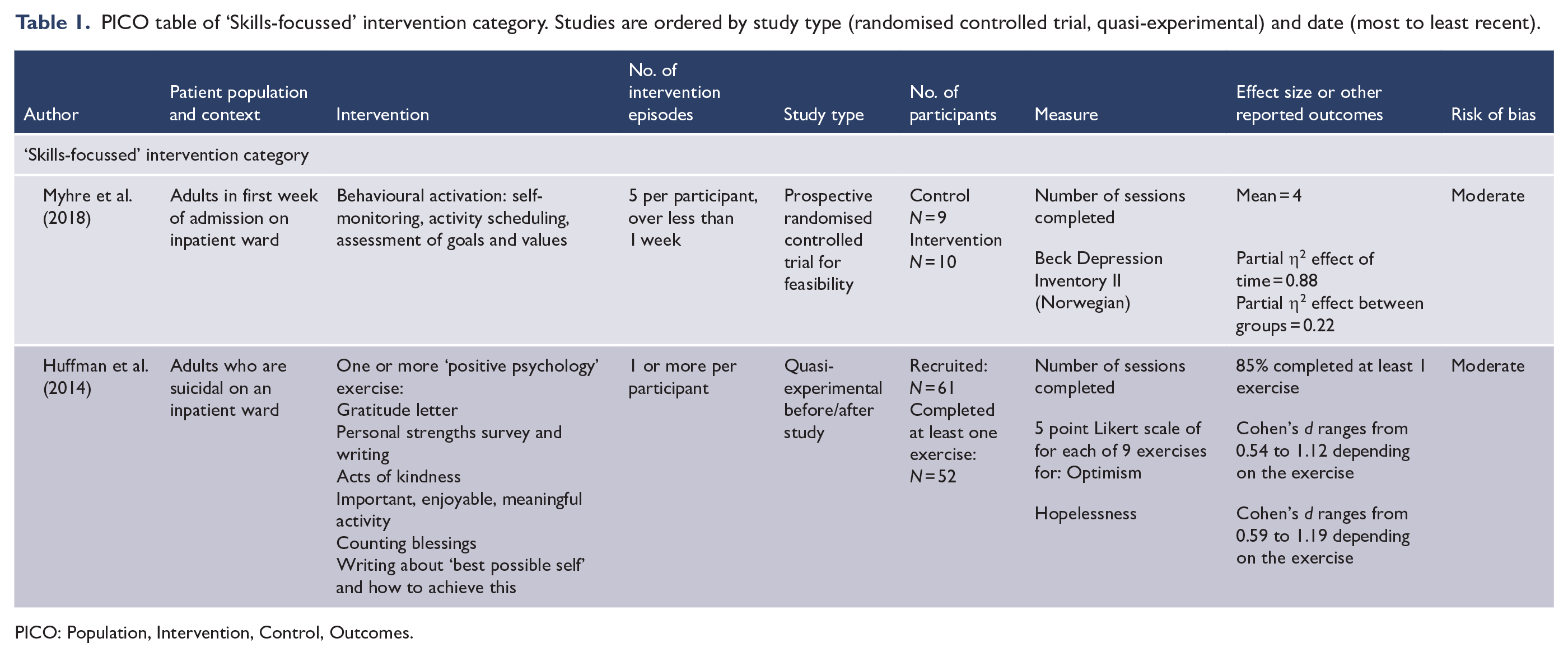
PICO: Population, Intervention, Control, Outcomes.
PICO table of ‘Psychoeducation’ intervention category. Studies are arranged according to study type (quantitative then qualitative) and then alphabetically according to author.
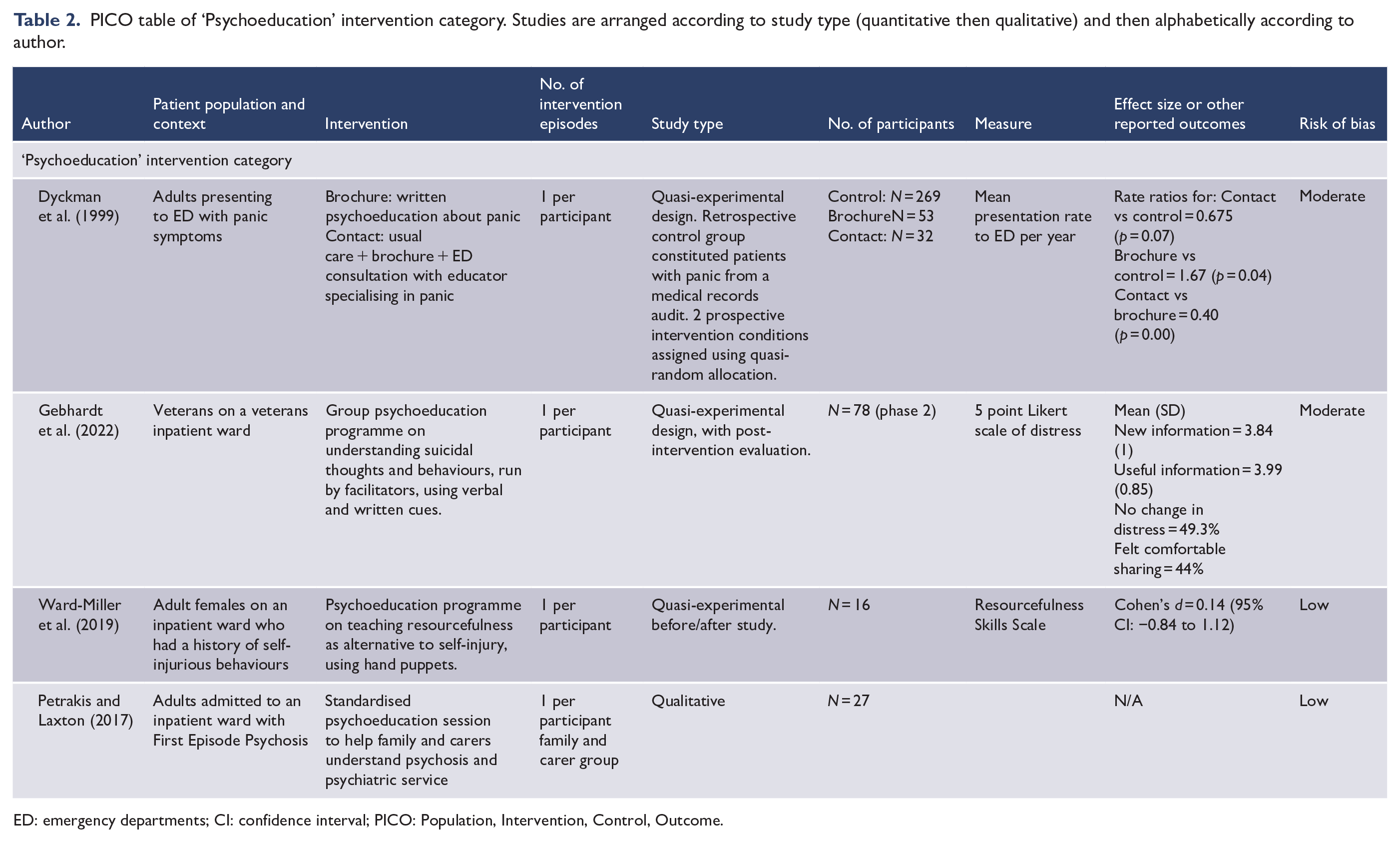
ED: emergency departments; CI: confidence interval; PICO: Population, Intervention, Control, Outcome.
PICO table of ‘Environment-focussed’ intervention category.
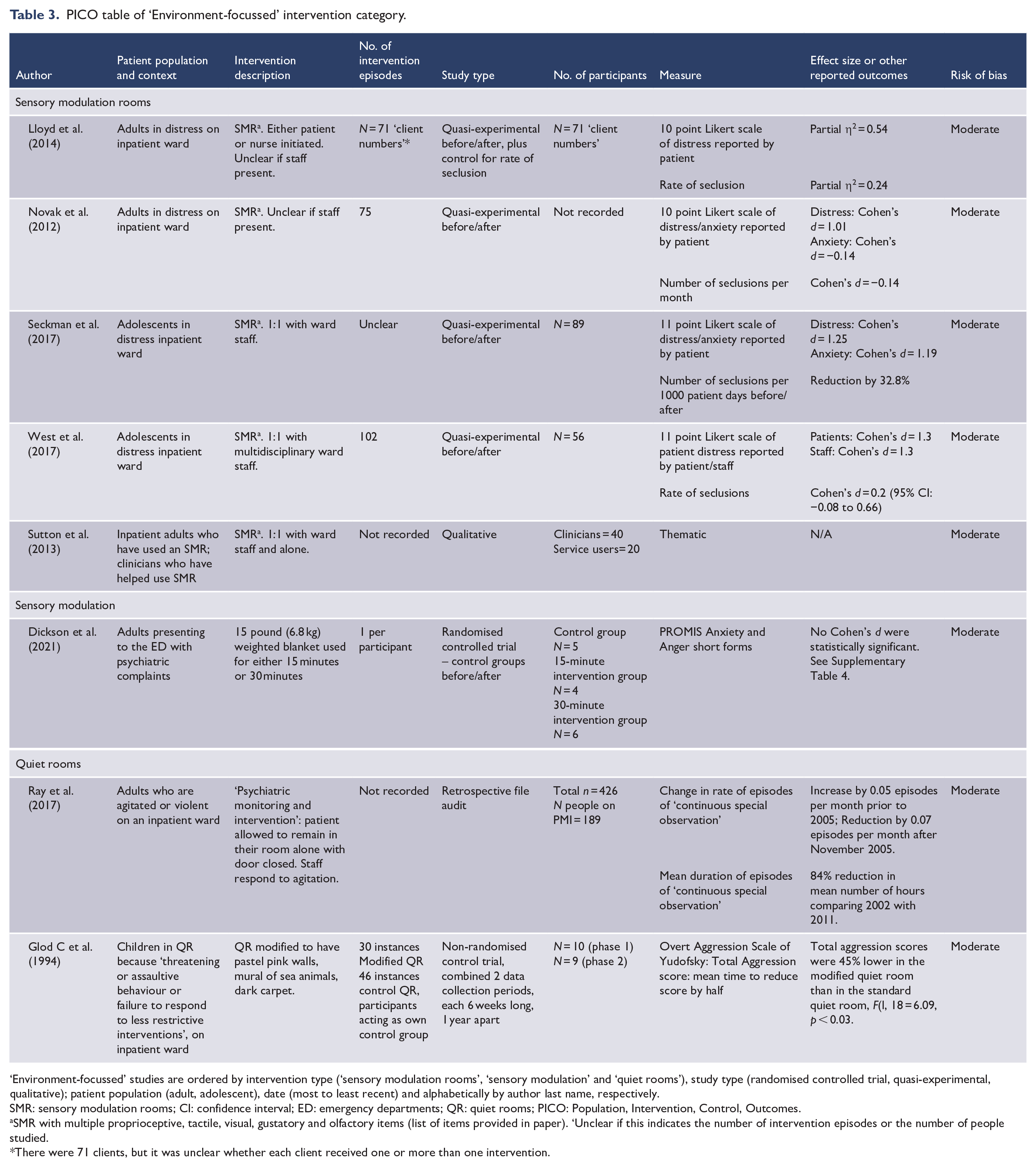
‘Environment-focussed’ studies are ordered by intervention type (‘sensory modulation rooms’, ‘sensory modulation’ and ‘quiet rooms’), study type (randomised controlled trial, quasi-experimental, qualitative); patient population (adult, adolescent), date (most to least recent) and alphabetically by author last name, respectively.
SMR: sensory modulation rooms; CI: confidence interval; ED: emergency departments; QR: quiet rooms; PICO: Population, Intervention, Control, Outcomes.
SMR with multiple proprioceptive, tactile, visual, gustatory and olfactory items (list of items provided in paper). ‘Unclear if this indicates the number of intervention episodes or the number of people studied.
There were 71 clients, but it was unclear whether each client received one or more than one intervention.
PICO table of ‘Special Observation’ intervention category.
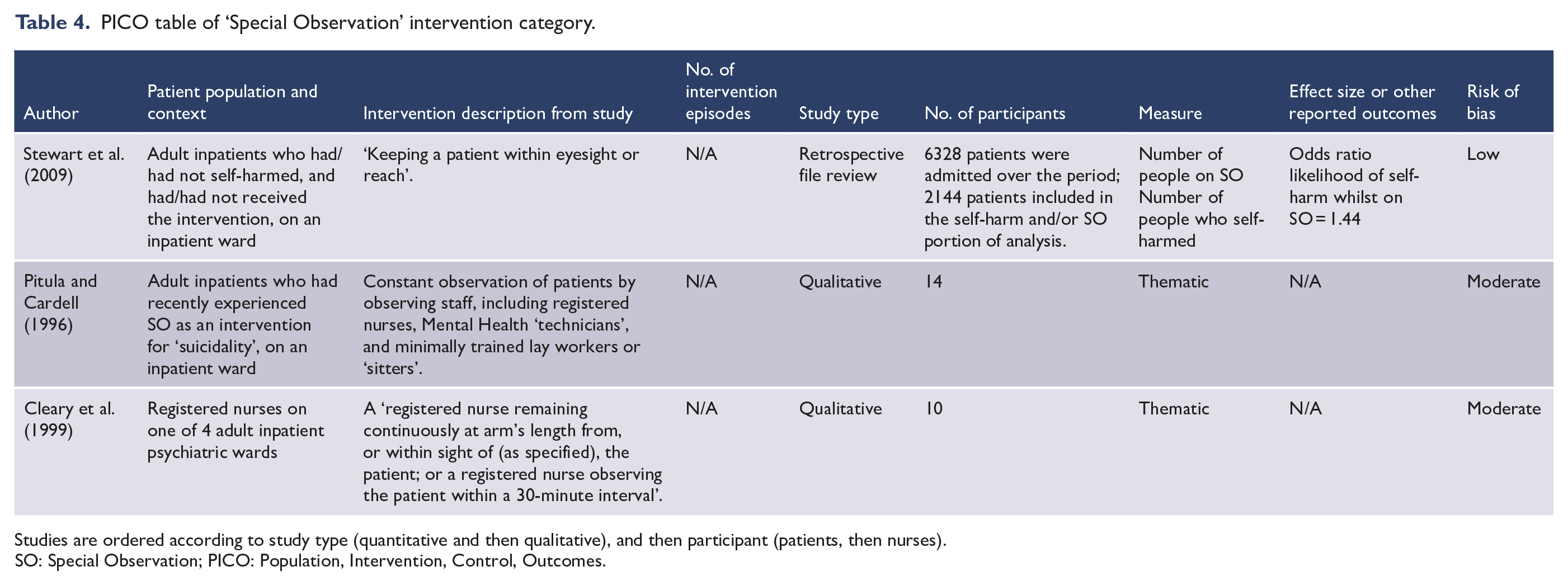
Studies are ordered according to study type (quantitative and then qualitative), and then participant (patients, then nurses).
SO: Special Observation; PICO: Population, Intervention, Control, Outcomes.
PICO table of ‘Multicomponent Group’ intervention category.
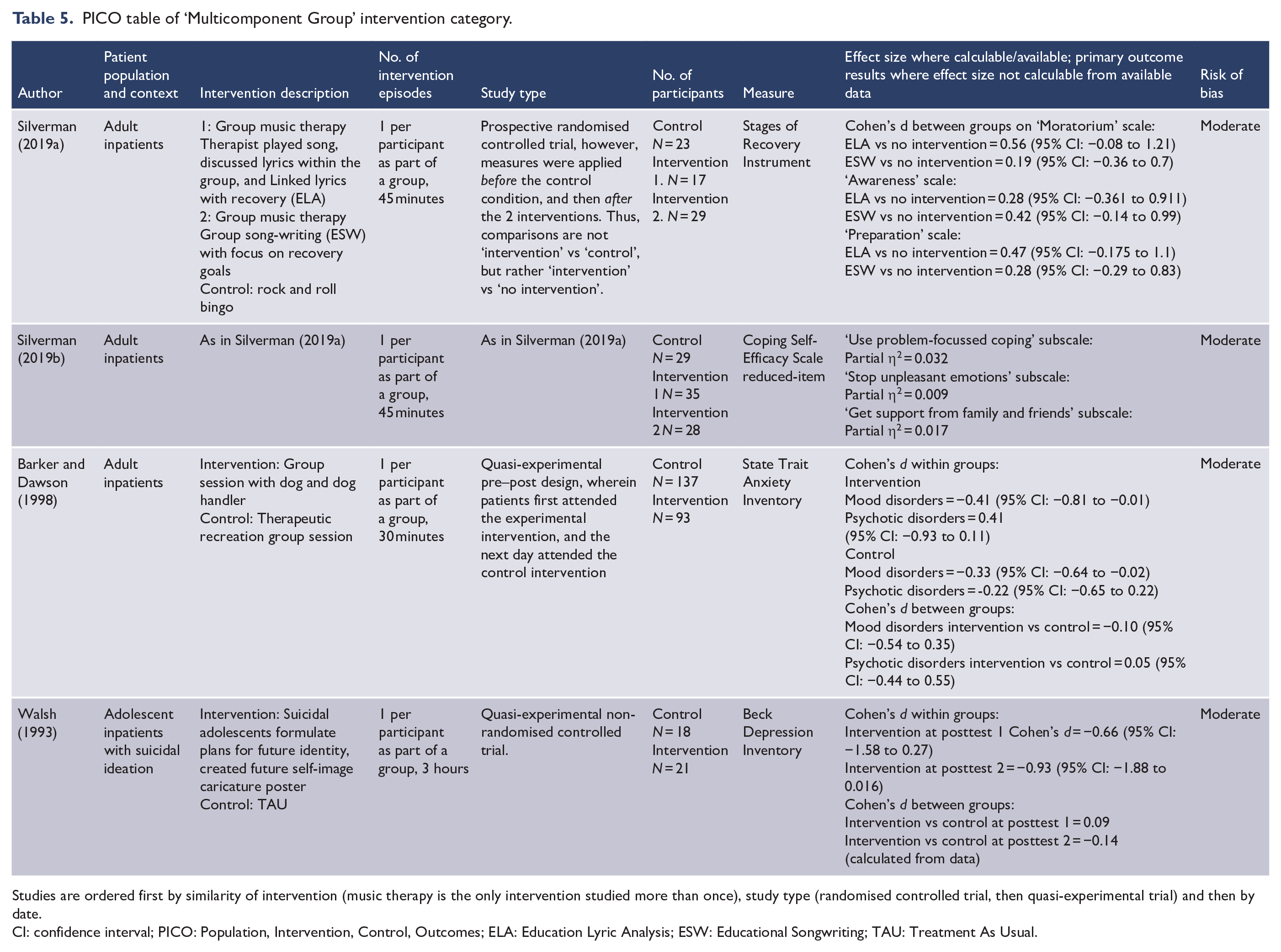
Studies are ordered first by similarity of intervention (music therapy is the only intervention studied more than once), study type (randomised controlled trial, then quasi-experimental trial) and then by date.
CI: confidence interval; PICO: Population, Intervention, Control, Outcomes; ELA: Education Lyric Analysis; ESW: Educational Songwriting; TAU: Treatment As Usual.
PICO table of ‘Multicomponent Individual’ intervention category, ‘suicide-specific’ intervention type.
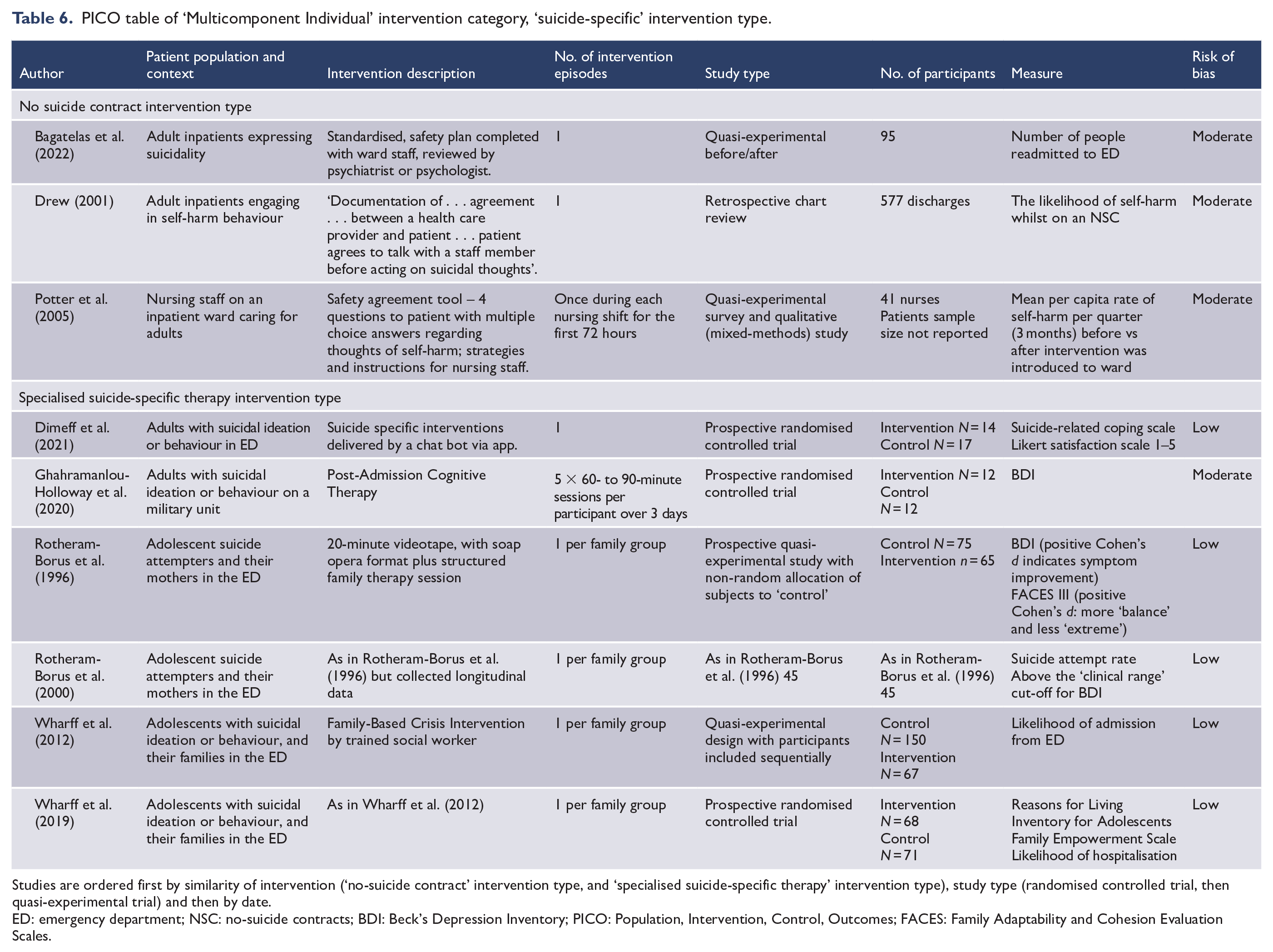
Studies are ordered first by similarity of intervention (‘no-suicide contract’ intervention type, and ‘specialised suicide-specific therapy’ intervention type), study type (randomised controlled trial, then quasi-experimental trial) and then by date.
ED: emergency department; NSC: no-suicide contracts; BDI: Beck’s Depression Inventory; PICO: Population, Intervention, Control, Outcomes; FACES: Family Adaptability and Cohesion Evaluation Scales.
Outcome measures
The outcome measures used to evaluate NPIs were highly variable (Tables 1–6 have outcome measures identified for use in potential meta-analyses, and Supplementary Table 17 for all outcome measures). We identified 26 primary outcome measures from the 39 studies where a primary outcome was specified, and 71 measures in total. Outcome measures used in the four quantitative sensory modulation room (SMR) studies were consistent, using either 10 (Lloyd et al., 2014; Novak et al., 2012) or 11 (Seckman et al., 2017; West et al., 2017) point Likert scales of distress, and number/rate of seclusions (Dickson et al., 2021; Lloyd et al., 2014; Novak et al., 2012; Seckman et al., 2017; West et al., 2017). Rate of self-harm was measured across all multicomponent-individual studies (Drew, 1999; Potter et al., 2005). Both quantitative short admission studies reported on ‘days admitted to hospital’; both commented on rates of self-harm but the measures were different (Berrino et al., 2011; Westling et al., 2019). Four ‘specialised suicide-specific intervention’ studies used comparable measures of depression symptoms (Beck’s Depression Inventory [BDI] or Children's Depression Inventory [CDI]) (Ghahramanlou-Holloway et al., 2020; Rotheram-Borus et al., 1996, 2000; Wharff et al., 2012), and three measured family constructs (Family Adaption and Cohesion Scale II/III) (Rotheram-Borus et al., 1996, 2000; Wharff et al., 2012). Outcome measures were otherwise dissimilar.
Clinical, methodological and statistical results
Results and heterogeneity are discussed in each section, ordered according to category and type.
Skills-focussed intervention category
We identified one controlled and one uncontrolled quantitative trial (Table 1; Supplementary Table 7). Myhre et al. (2018) reported a statistically significant between-groups improvement on BDI-II score using Behavioural Activation. Huffman et al.’s (2014) feasibility study of ‘positive psychology’ interventions reported a high participation consent rate and statistically significant within-group improvement in ‘optimism’, but there was no control group.
Psychoeducation intervention category
We identified three quantitative and one qualitative study. Table 2 has PICO study characteristics and data, with more detail presented in Supplementary Tables 15 and 16.
Dyckman et al. (1999) found a comparative reduction in panic attack presentations following face-to-face psychoeducation with a trained specialist primarily because the presentation rate for the ‘brochure-only’ group increased by 67% compared to control (p = 0.0417).
Ward-Miller et al. (2019) found that participants’ scores on a ‘Resourcefulness Scale’ did not improve following a resourcefulness-related psychoeducation programme using puppets. Gebhardt et al. (2022) found that a single-session suicide-focused group psychoeducation programme for veterans was feasible and acceptable. Forty-nine percent reported no change in distress, but participants ‘learned useful information’. Petrakis et al. (2017) identified several themes pertaining to a psychoeducation programme regarding first episode psychosis (Supplementary Table 16), although the philosophical perspective, research methodology and reflexive influence of the authors were not clear.
Environment-focussed intervention category
Sensory modulation and SMRs intervention type
Five quantitative (Lloyd et al., 2014; Novak et al., 2012; Seckman et al., 2017; West et al., 2017) studies (all quasi-experimental) and one qualitative study (Sutton et al., 2013) were identified. All five experimental studies found showed a significant within-group reduction in ‘distress’, but between-group effect sizes were small and did not reach statistical significance (Table 3). A qualitative analysis (Sutton et al., 2013) (Supplementary Table 5) attributed this distress reduction to the soothing nature of the SMR and staff–patient interaction. Two reported reduced seclusion rates (Lloyd et al., 2014; Seckman et al., 2017), but two others found no such effect (Novak et al., 2012; West et al., 2017) (Table 3; Supplementary Table 4).
Dickson et al. (2021) reported that weighted blankets in the ED reduced anxiety, but the small sample size reduced result reliability (Supplementary Table 4).
Quiet rooms intervention type
We identified two quantitative studies (Table 3; Supplementary Table 6). Glod et al. (1994) found a statistically significant reduction in total aggression for children in modified quiet rooms (QRs). In Ray et al.’s (2017) study, it was not possible to determine whether the intervention caused the observed reduction in ‘continuous special observation’.
Special Observation intervention category
We identified only one quantitative and two qualitative studies of this clinically common bNPI (Table 4; Supplementary Tables 8 and 9). The sole quantitative study (Stewart et al., 2009) retrospectively analysed data from 16 psychiatric units over a 3-year period and found that the use of Special Observation (SO) did not influence the incidence of self-harm in the following week.
In Pitula and Cardell’s (1996) qualitative study (Table 4; Supplementary Table 9), participants reported that the presence of staff made them feel less likely to lose control over self-harm impulses. Conversly, participants also reported feeling like prisoners, and high staff turnover of those conducting SOs made them feel like a burden. A study of nurses perceptions yielded nine themes (Cleary et al., 1999) (Supplementary Table 9) which pertained to patient safety and those undertaking observations feeling unseen by doctors.
‘Multicomponent Group’ intervention category
We identified four quantitative studies of group-based multicomponent interventions (Barker and Dawson, 1998; Silverman, 2019a, 2019b; Walsh, 1993). They are presented together in Table 3 and Supplementary Table 10, but are otherwise dissimilar. No studies showed significant changes on any outcome compared to controls. There was a within-group reduction in state anxiety associated with animal-assisted therapy (Barker and Dawson, 1998) in people experiencing psychosis, and within-group reductions in state anxiety for both animal-assisted therapy and the control group in those with mood disorders. Brief music therapy yielded no significant within-group effects (Silverman, 2019a, 2019b) (Table 5).
‘Multicomponent Individual’ intervention category
No-suicide contracts or safety planning intervention type
Two quantitative studies, and one mixed methods study evaluating no-suicide contract (NSC) or safety planning (SP) were identified (Table 6; Supplementary Table 11 effect sizes).
Potter et al. (2005) found no difference in the rate of self-harm following the introduction of NSCs (where patients are asked to contract that they will seek help when distressed and agree upon useful emotion management interventions) on an inpatient ward. Drew’s (2001) retrospective file review reported significantly higher levels of self-harm in patients with an NSC to those who had no such contract which they speculated was because people who were likely to self-harm were more likely to be placed on a NSC, rather than this being an adverse effect of the contract. Bagatelas et al. (2022) evaluated the quality of SP and found that those who completed a ‘high-quality’ SP were less likely to subsequently present to ED than those with a ‘low-quality’ SP. Whether this was because of the quality of the SP itself, or whether the quality of the SP reflected levels of motivation to engage in treatment, was not explored.
Specialised suicide-specific therapies intervention type
We identified six studies. Four were quantitative studies by two different research groups evaluating two different specialised suicide-specific multicomponent interventions, and only in the ED. Both investigated child and adolescent participants and their mothers (Table 6; Supplementary Table 12 has effect sizes).
Rotheram-Borus et al. (1996, 2000) reported that both mothers and adolescents scored persistently lower than control groups on depression and suicidality measures at 3 and 18 months. Outpatient follow-up was significantly higher for adolescents in the intervention group, and for those who rated their family as higher on adaptability on the FACES III (a measure of adaptation and cohesion of the family). FACES III scores were significantly higher for the intervention group than the control group for mothers, but not for adolescents.
Wharff et al. (2012, 2019) pilot study suggested that a family-based crisis intervention reduced hospitalisation in adolescents and replicated this comparative efficacy in an RCT. The Reasons for Living Inventory and Family Empowerment Scale scores improved significantly for both intervention and control groups (p < 0.001), but with no between-group differences.
An app-based suicide-specific ED intervention investigated by Dimeff et al. (2021) was found to be feasible and acceptable. There was a statistically significant improvement between groups for the Suicide-Related Coping Scale compared to Treatment As Usual (TAU), as well as distress, agitation and coping ability, and a non-significant increase in readiness to go home, on the Safety and Imminent Distress Questionnaire (Supplementary Table 12).
Ghahramanlou-Holloway et al. (2020) conducted a feasibility study of a brief Cognitive Behavioural Therapy (CBT) intervention on an adult inpatient military ward. While 24% declined to participate, none of the participants dropped out of the study. There were no significant changes in any measures.
‘Multicomponent Individual’: short admissions
We identified two quantitative studies, five qualitative studies, and one case study (Table 7; Supplementary Tables 13 and 14). Qualitative data pertaining to patient or clinician experiential evaluation of the ‘Brief Admission’ (BA) intervention were retained. Data pertaining to intervention components were excluded.
PICO table of ‘Multicomponent Individual’ intervention category – ‘short admission’.
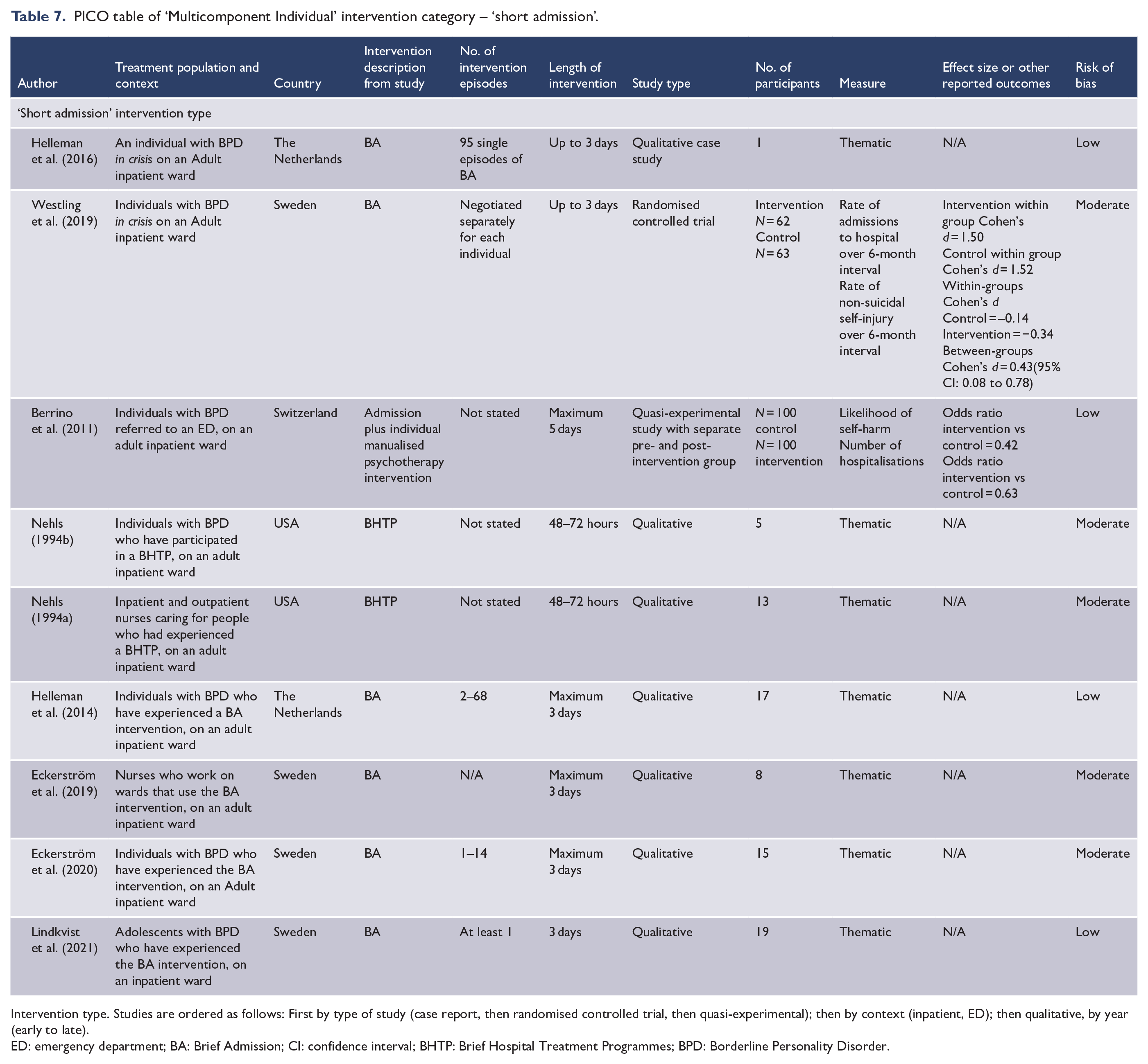
Intervention type. Studies are ordered as follows: First by type of study (case report, then randomised controlled trial, then quasi-experimental); then by context (inpatient, ED); then qualitative, by year (early to late).
ED: emergency department; BA: Brief Admission; CI: confidence interval; BHTP: Brief Hospital Treatment Programmes; BPD: Borderline Personality Disorder.
The two quantitative studies were undertaken in Scandinavia. At 3-month follow-up, Berrino et al. (2011) found that a short admission with concurrent manualised psychological intervention yielded a statistically significant reduction compared to TAU, in suicide attempt repetition, mean suicide attempt day survival, hospitalisation survival and mean number of days in hospital.
Westling et al. (2019) compared a BA which is ‘an intervention allowing individuals to hospitalize themselves. Duration . . . and frequency . . . are limited’ (p. 14), and specific goals of the intervention were discussed prior to admission to TAU. Over a 6-month period, they found significant reductions in days in hospital, number of visits to ED and self-harm rates within both intervention and controls but no between-group differences, probably reflecting regression to the mean. The intervention group achieved statistically significant improvements on the World Health Organization Disability Assessment Schedule (WHODAS) II mobility domain. At 12 months, those who had a BA maintained some improvement in function, but showed no reduction in repeat hospitalisations compared to TAU.
Qualitative studies
Supplementary Table 14 shows detailed qualitative results.
Five papers included patient participants and one qualitative case study; four were conducted in Scandinavia among research teams who have common affiliations, evaluating the BA approach (Eckerström et al., 2020; Helleman et al., 2014, 2016; Lindkvist et al., 2021) (Table 3), and the other investigated Brief Hospital Treatment Programmes (BHTP) in the United States (Nehls, 1994b). Commonalities included hospital as a ‘timeout when times were tough’ (Eckerström et al., 2020), ‘respite’(Nehls, 1994b), ‘feeling safe and relieved’(Lindkvist et al., 2021), ‘time out from daily life’(Helleman et al., 2014) and ‘crisis containment’(Helleman et al., 2016).
Two papers included nurse participants. In both studies, the nurses identified ‘empowerment’ of the patient as a key outcome and emphasised that the environment needed to be ‘caring’, though the participants in Nehls’ (1994a) study identified the inherent conflict within the term ‘mandated caring’. Participants in Eckerström’s (2019) study emphasised the goal of partnership between patient and nurse.
Discussion
Principal findings
This is the first systematic review of evaluations of bNPIs for people in a crisis of mental ill-health, in EDs and inpatient units. Studies that found between-group differences on inpatient units include Behavioural Activation (improved BDI) (Myhre et al., 2018), QR (reduction in total aggression in children) (Glod et al., 1994), Safety Planning (reduction in ED readmissions as long as they were ‘high quality’) (Bagatelas et al., 2022), BAs with a manualised psychological intervention (reduced suicide attempt repetition, mean suicide attempt day survival, hospitalisation survival and mean (number of days in hospital) (Berrino et al., 2011) and BAs without a manualised psychological intervention (improvements on the WHODAS II mobility domain) (Westling et al., 2019).
In the ED setting, between-group differences were found in suicide-specific ED interventions (reduced depression and suicidality measures immediately; Dimeff et al., 2021) and at 3 and 18 months (Rotheram-Borus et al., 2000), higher outpatient follow-up rates (Rotheram-Borus et al., 2000), reduced rates of hospitalisation (Wharff et al., 2019) and face-to-face specialist psychoeducation on panic (reduced ED presentation rate) (Dyckman et al., 1999). However, common interventions such as sensory modulation, weighted blankets, psychoeducation, continuous SO, animal therapy, music therapy and ‘no suicide’ contracting failed to show between-group benefits. Very few studies were replicated, making patterns difficult to identify.
Intervention settings
A visual map of the studies (Figure 1) indicates that the bNPIs evaluated in ED and inpatient settings are different and that considerably fewer interventions have been studied in EDs. This is significant, as it highlights an untapped opportunity to initiate interventions within the ED context and seamlessly extend their treatment into inpatient settings. While it is understandable that group therapies have not been evaluated in EDs, other bNPIs such as sensory modulation and SMRs, the use of SO, and skills-focussed interventions are used in this setting have not been evaluated. Conversely, suicide-specific interventions that have some evidence of effectiveness in the ED have potential for implementation in short-stay inpatient environments. Although there may be less if any impact in reducing suicide mortality (Fox et al., 2020), there appears to be other valuable therapeutic effects. Having said that, of the four interventions tested in ED, only one was even partially performed by ED clinicians. Investigating the feasibility of ED clinicians delivering psychiatric interventions (as has been done for drug health–related intervention (Kaner et al., 2018)) is vital, given the majority of EDs do not have access to a sub-specialised psychiatric services. Finally, almost all ED interventions were studied in the United States, a possible reflection of geographically specific priorities.
Synthesis of effectiveness of brief NPIs
This review found that the evidence base for crisis-related brief NPIs is insubstantial, with such inconsistency in outcomes that it seems impossible to claim that patients are being treated in an evidence-based way. We found little evidence on which to base education, clinical practice, guidelines and policy and significant gaps for many commonly used NPIs. Table 8 summarises the discussion regarding each intervention category (Supplementary Table 18 for extended discussion).
Main findings and future research recommendations according to intervention category and type.
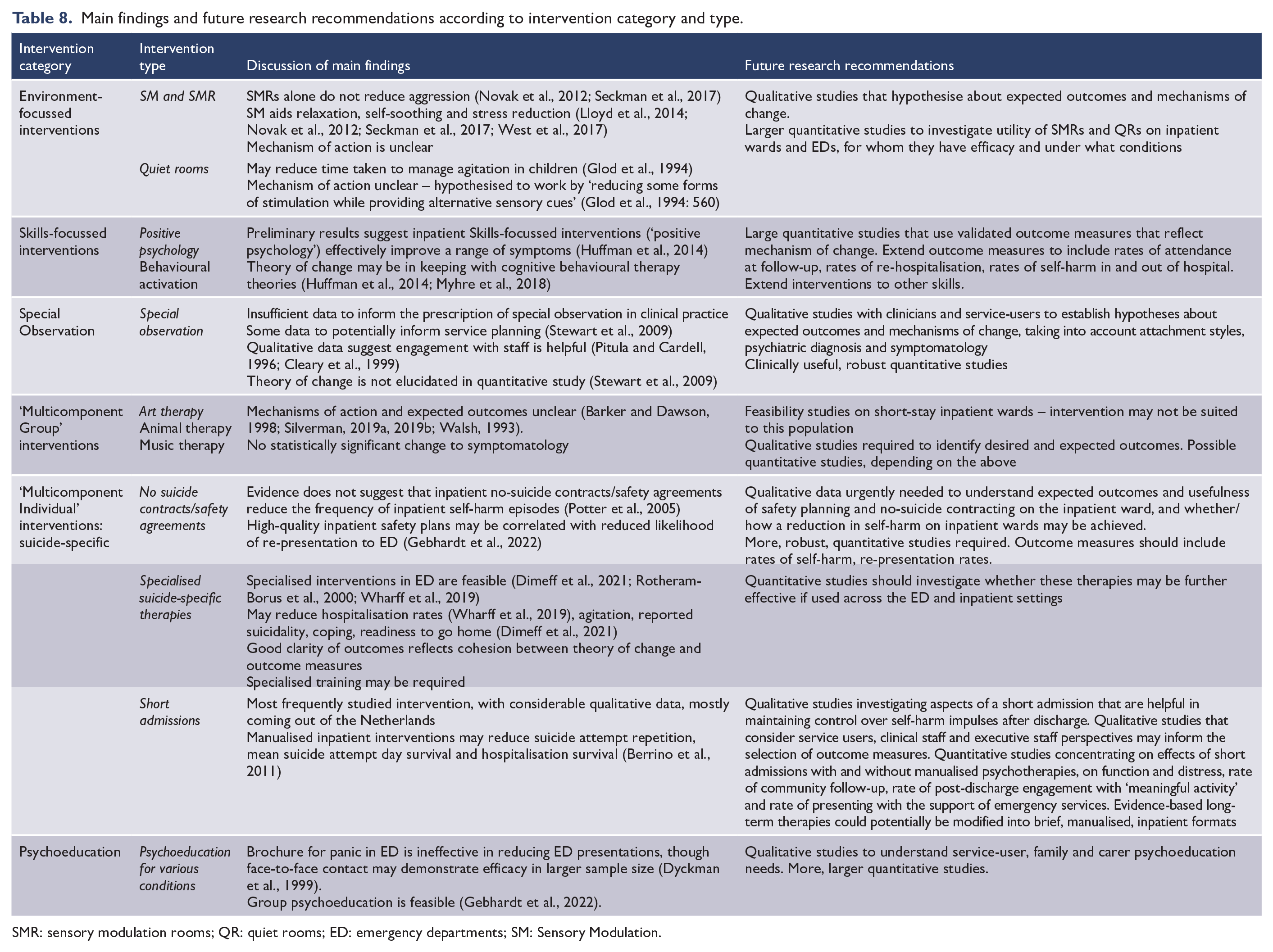
SMR: sensory modulation rooms; QR: quiet rooms; ED: emergency departments; SM: Sensory Modulation.
There are positives for bNPIs. Of the single modality intervention, there seems promising evidence for interventions that modulated the environment via sensory reduction and/or weighted blankets and positive skill approaches that need replication. More complex multicomponent suicide-specific interventions seem effective for some aspects of symptoms and coping, and had additional impact on the family and service use, and one coordinated research group has published several papers providing support for coordinated BAs.
Conversely, given the widespread use of SOs and NSCs, the lack of effectiveness demonstrated in the few evaluations is concerning, especially given existing evidence that safety planning is effective in other settings (though the intervention is yet to be subjected to meta-analysis) (Ferguson et al., 2022). Psychoeducation was thought acceptable although was ineffective, and the limited evaluations of brief group-based interventions of less ‘clinical’ interventions, e.g., using animals or music, showed no benefit. We found no studies evaluating other commonly used interventions such as the quantitative effects of SO, specific verbal de-escalation strategies or evidence-based psychotherapy modalities (such as mentalisation-based or transference-focussed psychotherapy) that could be adapted for crisis settings.
Outcome measures
Evaluations of bNPIs have used a wide range of outcome measures, with limited consistency even among studies with similar interventions, indicating an inconsistency in the alignment of bNPI objectives. This might arise from insufficient research appraisal, a fragmented research landscape or a disconnection between research and clinical aims. Outcome measures need to align with intervention’s theory of change, patients’ treatment expectations and anticipated rate of change in short-stay environments. It is imperative that researchers ask clinicians, patients, families and carers: what do we expect to change in such a short time, or be affected in the longer term from a bNPI? This might include questions about whether clinicians expect rates of self-harm and suicide to reduce, given their long-term often recurrent nature, or whether it is more appropriate to expect a shift in motivation to engage in treatment, a temporary change in mood and anxiety levels, intensity of suicidal thoughts, increased linkages in the community or a comprehensive follow-up plan.
Recognising the significance of outcome measures, the development of a shared core outcome set (Mestre Navas et al., 2022) is recommended, defining the minimum best-practice measurement requirements. In the absence of such a set, researchers can turn to resources like the COSMIN (COnsensus-based Standards for the selection of health Measurement Instruments) website or engage in collaborative design through methods like Delphi studies (as has been done in Australia (Hill et al., 2019)) or consensus statements (co-produced by stakeholders).
How do we progress from here
The identified quantitative studies predominantly had low sample sizes limiting power to show an effect, and most studies had a moderate risk of bias (high-risk studies were excluded). There are challenges in performing trials of complex interventions (Skivington et al., 2021), and in sourcing funding for interventions that are difficult to commercialise; however, the lack of organisation and consistency may also imply a de-prioritisation of EDs as treatment environments.
Across most studies, there was a lack of comprehensive discussion around theory of change. While most studies mentioned theory of change, it was not always clear whether, or how, the theory of change related to outcome measures. While this is difficult to quantify (Aggarwal et al., 2021; Mestre Navas et al., 2022), as goals and mechanisms of action become clear, outcome measures can be chosen so as to reflect change mechanisms. Ideally, valid and reliable measures should be prioritised over untested outcome measures.
As well as identifying possible theories of change, researchers and clinicians would benefit from a clearly defined set of patient groups and intervention goals. This is not straightforward. To understand which interventions work for whom, researchers may wish to group individuals into symptom-based groups such as suicidal thoughts or behaviours (O’Connor et al., 2020; Schuck et al., 2019), behavioural disturbance and psychosis. However, goals will not be clear without further qualitative exploration. Attempts have been made to define goals of treatment and research (D’Onofrio et al., 2010; Wilson et al., 2019) but this is demonstrably difficult to achieve (Wilson et al., 2019).
Instead, future studies may have to consider comparative effectiveness pragmatic trials, stepped-wedge studies, cluster randomised studies and studies where individuals are randomised to various TAU alternatives (Briffa et al., 2021). These should utilise pre-existing frameworks for developing and evaluating complex interventions (Skivington et al., 2021). Suicide-specific interventions in EDs show promise for outcomes other than suicide mortality, emphasising the value of using EDs for treatment rather than solely assessment.
Limitations of synthesis
There are several limitations to this review. For example, the PICO elements may have been too restrictive. Ideally, this review would be considered with reviews investigating interventions that continue into outpatient settings, otherwise the reader may have an incomplete understanding of interventions that may be offered in EDs and crisis settings. Useful studies may have been excluded because there is no standardised definition of ‘crisis’ in the literature, though the definition was designed in such a way as to maximise study capture. It may also have been reasonable to include papers on interventions on medical wards. In addition, the taxonomy of interventions was subjective. We did not review educational documents, cannot guarantee we appraised all the grey literature and we only evaluated English language documents. Thus, some papers were likely missed, although our approach minimised the risk of missing high-quality, publicly available articles with low bias.
Recommendations for policy and practice
The evidence base for NPIs in inpatient settings offers weak recommendations across the board, leaving clinicians with minimal evidence-based guidance upon which to base their practice or satisfy the requirements of guidelines. This may be why guideline documents generally do not stretch to recommending specific interventions (NICE, 2022; Wales, 2015). However, several interventions show promise, such as short admissions with accompanying psychotherapies, SMRs and suicide-specific interventions. Interestingly, reviews have found a similar lack of structure in the fields of managing restrictive practice (Baker et al., 2021), inpatient NPIs (Jacobsen et al., 2018) and acute severe behavioural disturbance (Weiland et al., 2017). This could be attributed to the inherent challenges of conducting research in emotionally charged and hectic environments. One significant challenge, understandably, pertains to obtaining informed consent, although relevant frameworks are available (Larsen and McMillin, 2011; Manti and Licari, 2018; Vitiello, 2008). Notably, informed consent was not thoroughly discussed in any of the papers included herein.
Primarily then, funding should be allocated to studies investigating bNPIs for those in a crisis that (1) clearly identify the need they are fulfilling; (2) are translatable into the clinical environment; (3) utilise outcome measures that are reliable, valid and appropriate to the theory of change; (4) that may replicate studies done in other treatment centres; (5) that look at the effects of starting bNPIs within the ED and continuing them to the inpatient ward, recognising the potential for the ED as a treatment setting; and (6) identify how they will manage the barriers of performing research in such a challenging clinical setting. Such funding should take into account other aspects of effective treatment for those in crisis that are not investigated here, such as structural environment and service model changes.
Conclusion
This systematic review indicates that there is great need for high-quality research into brief NPIs. The current evidence base is very limited; inconsistent and outcome measures are too varied to identify which NPIs may be best for which people. It might be argued that many NPIs such as ‘means restriction’ or ‘special observation’ are too obviously clinically required to need evidence, but all interventions can have risks and benefits that need to be weighed. To address this, researchers should define theories of change of their chosen interventions and map the outcome measures that pertain to the goals of treatment, as well as using pre-existing frameworks so that clinicians and policy makers can make better choices.
Supplemental Material
sj-docx-1-anp-10.1177_00048674231216348 – Supplemental material for The effectiveness of brief non-pharmacological interventions in emergency departments and psychiatric inpatient units for people in crisis: A systematic review and narrative synthesis
Supplemental material, sj-docx-1-anp-10.1177_00048674231216348 for The effectiveness of brief non-pharmacological interventions in emergency departments and psychiatric inpatient units for people in crisis: A systematic review and narrative synthesis by Jacqueline P Huber, Alyssa Milton, Matthew C Brewer, Louisa M Norrie, Saskia M Hartog and Nick Glozier in Australian & New Zealand Journal of Psychiatry
Footnotes
Acknowledgements
The authors would like to acknowledge Dr Zeeshan Shahnawaz for her essential role in editing this paper.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was support by the St Vincent’s Hospital AMR Clinician Buyback Grant.
Registration number
PROSPERO: CRD42021287496
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.