
Abstract

Introduction
Globally, psychotropic medication use for mental health problems is increasing among young people, despite debate regarding its safety and efficacy during critical stages of brain development (Karanges et al., 2014; Kovess et al., 2015; Piovani et al., 2016, 2019). Australian health register data indicate that the annual prevalence of psychotropic dispensing among young people (<18 years) in 2021 was 4.4% for attention deficit hyperactivity disorder (ADHD) medications, 2.0% for antidepressants, 0.6% for antipsychotics and 0.13% for anxiolytics (Wood et al., 2023).
Cumulative incidence data can augment prevalence estimates by providing useful information about lifetime prescriptions. Danish population register data show the cumulative incidence of psychotropic drug prescription by age 20 years to be 5.1% for antidepressants, 4.4% for anxiolytics, 2.0% for antipsychotics and 1.4% for ADHD medications (Kessing et al., 2023). Equivalent estimates for young people outside Europe are lacking. The current study used Australian government register data for a population cohort of >86,000 youth to determine the cumulative incidence of psychotropic prescriptions in the first 20 years of life.
Methods
Participants were 86,782 youth from the New South Wales (NSW) Child Development Study (Green et al., 2018), with a median age of 20 years (range = 19–22 years). Record linkages were conducted by the Centre for Health Record Linkage (www.cherel.org.au) and the Australian Institute of Health and Welfare (AIHW) (www.aihw.gov.au/our-services/data-linkage). Ethical approval was granted by the Australian Capital Territory (ACT) Health and NSW Population & Health Services Human Research Ethics Committees (HREC/18/ciphs/49) and the AIHW HREC (EO2020/4/1026) according to the ‘waiver of consent’ provision of the National Statement of Ethnical Conduct in Human Research (National Health Medical Research Council [NHMRC], 2023).
Psychotropic prescriptions across the first 20 years of life were identified in the Australian Commonwealth Department of Health’s Pharmaceutical Benefits Scheme (PBS; 2001–2024); the number of prescriptions for psychotropic drugs was coded according to World Health Organisation Anatomical Therapeutic Chemical therapeutic subgroups of antipsychotics (N05A), anxiolytics (N05B), sedatives and hypnotics (N05C), antidepressants (N06A) and stimulants (N06B). A young person could be prescribed more than one type of medication, and each type could be prescribed multiple times to each individual. Polypharmacy was examined as (1) the number of unique chemical substances prescribed within each of these five therapeutic subgroups (i.e. number of unique ATC level 5 codes prescribed to each child) and (2) across therapeutic subgroups (i.e. number of unique ATC level 3 codes prescribed to each child).
Analyses and figure generation were performed in R v4.0.3. Prescriptions after age 20 years were collapsed into a 20+ age bracket, as 44.4% of the cohort had not yet reached 21 years of age.
Results
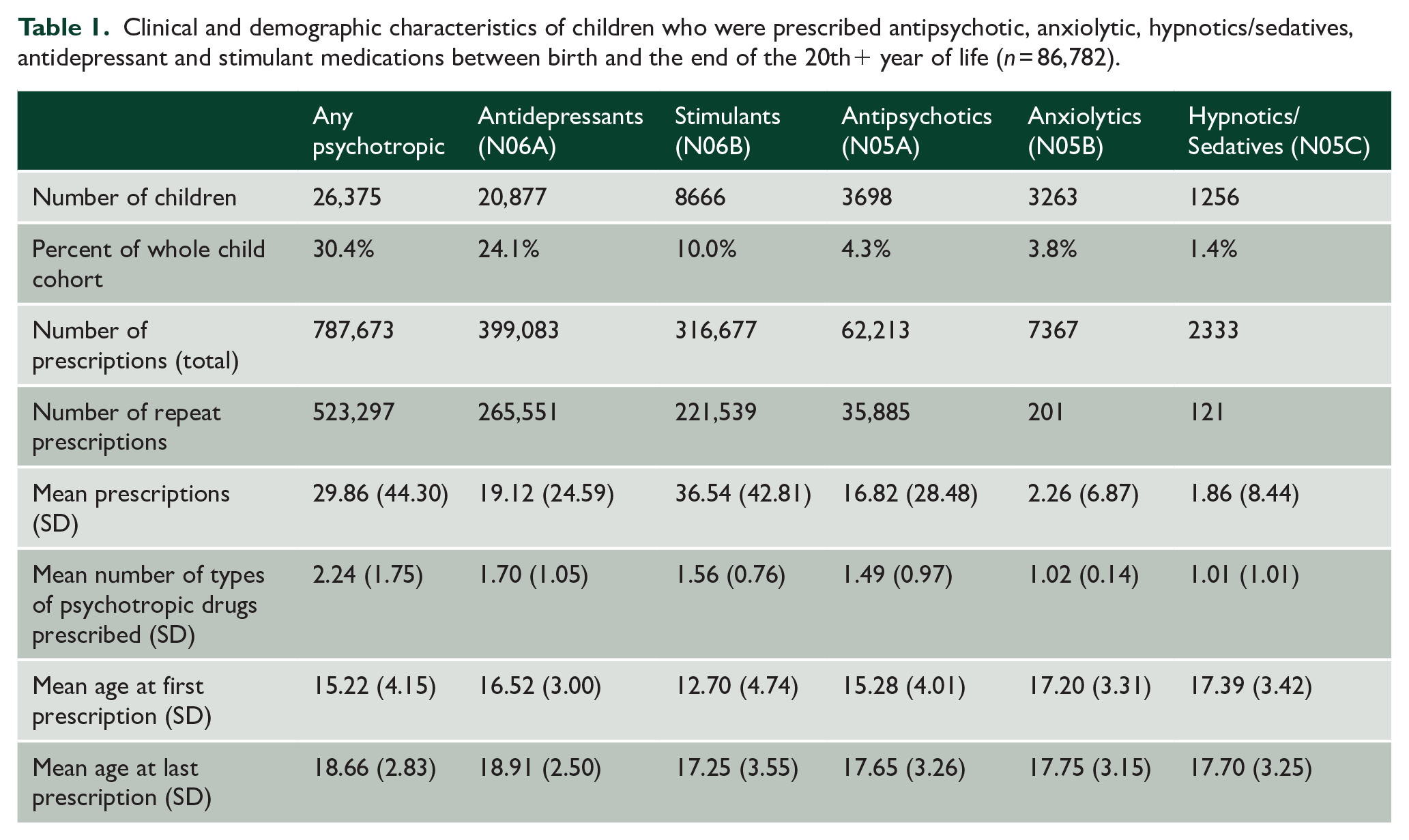
In total, 26,375 (30.4%) young people, 56.1% (n = 14,791) of whom were male, were prescribed psychotropic medication in their first 20+ years of life, comprising a total of 787,673 prescriptions. Descriptive information is detailed in Table 1. Of 86,782 children in the cohort, 24.1% received a prescription for an antidepressant, 10.0% for a stimulant, 4.3% for an antipsychotic, 3.8% for an anxiolytic and 1.4% for a hypnotic/sedative. Just over two-thirds of psychotropic prescriptions were repeat prescriptions (66.4%), with the highest rates of repeat prescriptions evident for stimulants (70.0%), antidepressants (66.5%) and antipsychotics (57.7%); relatively low proportions of repeat prescriptions were evident for anxiolytics (2.7%) and hypnotics/sedatives (5.2%). The majority (67.7%; n = 17,851) received a prescription for only one of the examined therapeutic subgroups, while 23.4% (n = 6162) received prescriptions for two therapeutic subgroups; 7.3% (n = 1918) received prescriptions for three therapeutic subgroups of psychotropics, 1.5% (n = 389) received prescriptions for four therapeutic subgroups and 0.2% (n = 55) received prescriptions for all five of the examined psychotropic therapeutic subgroups (i.e. across stimulant, antidepressant, antipsychotic, anxiolytic and hypnotic/sedative drugs). Within each therapeutic subgroup, the highest rate of polypharmacy was evident for antidepressants, followed by stimulants, antipsychotics, anxiolytics and hypnotics/sedatives.
Clinical and demographic characteristics of children who were prescribed antipsychotic, anxiolytic, hypnotics/sedatives, antidepressant and stimulant medications between birth and the end of the 20th+ year of life (n = 86,782).
The annual and cumulative incidence of psychotropic prescriptions and the number of prescriptions for each type of psychotropic medication, across the first 20 years of life, are shown in Figure 1. Stimulants were prescribed earlier in childhood and comprised almost 51% of prescriptions dispensed, increasing steadily from age 4 years, before plateauing in early-to mid-adolescence. In contrast, the age of first antidepressant use was later, with the sharpest rise between ages 12 and <16 years. There was also a further slight incline in the cumulative percentage of children being prescribed stimulant prescriptions between 16 and 20+ years. Prescriptions for antidepressants increased rapidly from age 10 years, overtaking stimulants as the most prescribed psychotropic from age 15 years onwards. Similar, yet less pronounced trends were also observed for antipsychotics and anxiolytics, with anxiolytic and sedative/hypnotic prescriptions beginning to increase later in adolescence (~17 years) relative to antipsychotics (~15 years).
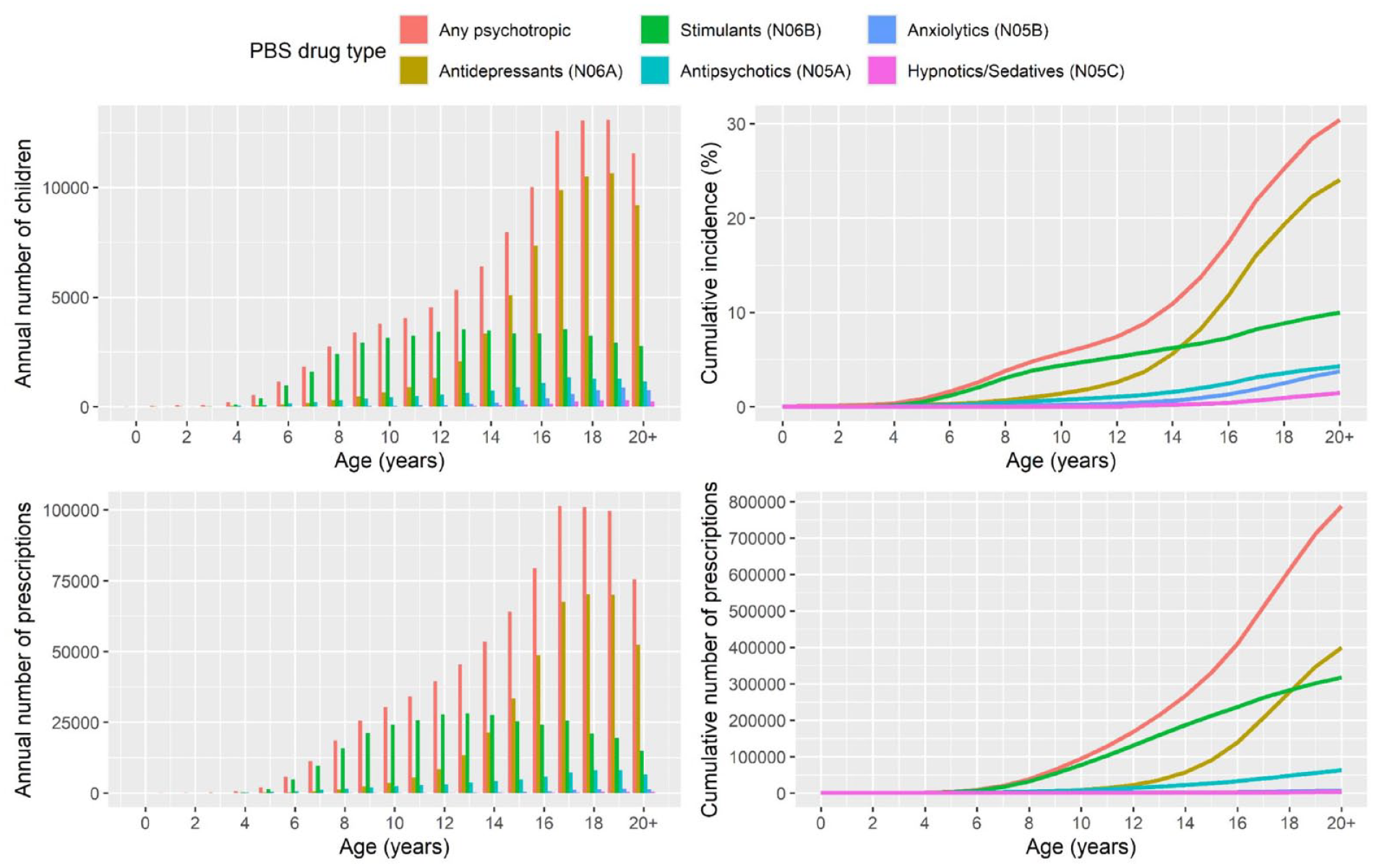
Annual and cumulative incidence in terms of the percentage of children with a psychotropic prescription and the number of children prescribed psychotropic medications between birth and 20+ years.
Discussion
In a population cohort of >86,000 Australian youth, more than 30% were prescribed psychotropic medication by 20+ years of age and, consistent with international data (Piovani et al., 2019), the annual rate of prescriptions increased steadily with age. Polypharmacy across the psychotropic therapeutic subgroups was relatively common, with more than one-third of youth on psychotropics (9.8% of the total cohort) receiving two or more therapeutic subgroups of psychotropic medication. The cumulative incidence of psychotropic prescriptions was higher than annual prevalence estimates reported up to age 18 years in Australia (Wood et al., 2023), and there were further increases by age 20 years. For example, in the current study (2024), the cumulative incidence of stimulants up to age 18 years was 8.8% (4.4% prevalence in 2021), with 19.3% for antidepressants (2.0% prevalence in 2021), 3.6% for antipsychotics (0.6% prevalence in 2021) and 2.5% for anxiolytics (0.13% prevalence in 2021).
Relative to rates of psychotropic prescribing to people of the same age in Denmark, the cumulative incidence of psychotropic prescriptions reported here was 7.1 times higher for stimulants, 4.7 times higher for antidepressants and 2.2 times higher for antipsychotics, while anxiolytics were prescribed at roughly the same rate (Kessing et al., 2023). This is consistent with reports of lower annual stimulant prescription rates in some European countries (Piovani et al., 2019) and relatively greater prescribing of stimulants in Australia (Wood et al., 2023). Variation in the rate of prescriptions between Europe and Australia may be attributed to differences between countries in policies, accessibility and attitudes towards psychotropics (Piovani et al., 2016, 2019).
The primary limitation of this study is that not all psychotropic drug prescriptions were captured by the PBS (e.g. excludes prescriptions provided as an inpatient or privately funded patient, off-label prescriptions or those below the co-payment threshold), although the majority of prescriptions are captured (Karanges et al., 2014). This limitation should be considered against the strengths of this study, namely, the large sample size, length of follow-up and low selection bias.
In conclusion, more than three in every 10 youth up to the age of 20 +years were prescribed psychotropic medication in this population cohort study, and around 10% were prescribed two or more such medications. The rates of psychotropic drug prescribing for children and adolescents in Australia are high and appear to exceed those found in comparable countries; rates of polypharmacy are similarly high. Quantification of the cumulative incidence of psychotropic prescription provides important information for policymakers when planning mental healthcare for children and adolescents.
Footnotes
Acknowledgements
This research used population data owned by the NSW Department of Education; Australian Curriculum, Assessment and Reporting Authority (ACARA), managed by the NSW Education Standards Authority; NSW Department of Communities and Justice; NSW Ministry of Health; ACT Health; NSW Registry of Births, Deaths and Marriages; the Australian Coordinating Registry (on behalf of Australian Registries of Births, Deaths and Marriages, Australian Coroners and the National Coronial Information System); Australian Bureau of Statistics; Australian Institute of Health and Welfare; Department of Social Services; NSW Bureau of Crime Statistics and Research; NSW Department of Justice and NSW Police Force. This research used data from the Australian Early Development Census (AEDC). The AEDC is funded by the Australian Government Department of Education. The findings and views reported are those of the authors and should not be attributed to these Departments or the NSW and Australian Government. Record linkages were conducted by the NSW Centre for Health Record Linkage (CHeReL) and the Australian Institute of Health and Welfare Data Integration Service Centre.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This research was conducted by the University of New South Wales with financial support from the National Health and Medical Research Council (NHMRC) Project Grant (APP1148055) and Investigator Grant (APP1175408 awarded to K.D.); Australian Research Council (ARC) Discovery Project (DP230101990), Future Fellowship (FT170100294 awarded to K.R.L.) and Discovery Early Career Researcher Award (DE210100113 awarded to S.T.); Department of Health and Aged Care Medical Research Future Fund Million Minds Mental Health Grant (APP2006436); and a Postdoctoral Fellowship from Suicide Prevention Australia (awarded to O.J.W.).
Data Availability Statement
Data used in this project have been provided by government or other agencies for the research purposes of the NSW Child Development Study and are unable to be shared with third parties or deposited into data repositories. Researchers wishing to access these data need to apply in writing to relevant data custodians.