
Abstract
Background:
Psychiatric Emergency Care Centres do not have a clear treatment model or evidence base. An understanding of the patient population, clinical practice and approaches is needed to develop an evidence-based framework.
Objectives:
Identify staff perceptions of the purpose of Psychiatric Emergency Care Centres, who should be treated and how.
Methods:
A multidisciplinary sample of clinicians and administrators currently working in, or with administrative oversight of, Psychiatric Emergency Care Centres were interviewed. All New South Wales Psychiatric Emergency Care Centres were approached and staff self-selected. A total of 36 people participated, including nurses, doctors, social workers and managers. A critical realist qualitative thematic analysis approach was used, with an inductive orientation.
Results:
Having an achievable admission goal was important. Although ‘harm minimization’ was often cited as important, this meant conflicting, superimposed notions to different people, including minimizing self-harm, reducing iatrogenic harm from unnecessary or coercive intervention and limiting harm to a resource-constrained system. Participants reported significant clinical practice variation and confidence in their practice.
Conclusion:
The approach to the primary goal of ‘harm minimization’ reflects conflicting priorities in a complex system which are often not explicit. However, we identified a clinical practice framework upon which to base care pathways, training, intervention development and outcome assessment.
Introduction
Australian Psychiatric Emergency Care Centres (PECCs) are multidisciplinary units, introduced in New South Wales in 2005 to relieve the pressure of Psychiatric presentations on emergency departments (EDs) (Health, 2015). NSW is Australia’s most populous state and receives the highest number of psychiatric presentations to their EDs (Australian Institute of Health and Welfare AG, 2024). PECCs were attached to EDs, designed for people with low likelihood of aggression, expected to stay no longer than 48 hours. They differ from more recent ED ‘mental health hubs’ in that they are inpatient beds, under the governance of Psychiatry teams. Since their inception, while the rate of use has increased with a NSW average of approximately 860 patients per year (Huber et al., 2021), there has been little research performed on the function or effectiveness of PECCs (Brakoulias et al., 2010; Huber et al., 2021; Seymour et al., 2020). This paucity of data is reflected in the evaluation of short-stay psychiatric unit treatment interventions internationally (Anderson et al., 2022; Huber et al., 2024; Mitchell et al., 2020). Despite this, short-stay units proliferate.
The most recent PECC Model of Care (MoC), written 10 years ago, identifies that there is ‘no convincing evidence to support a “preferred” or “best practice” model’ (Health, 2015) and with a lack of research, PECCs still do not have a distinct clinical framework. A clear priority is to understand how PECCs are being used, and for whom, to enable our understanding of what is ‘best practice’ and what can be locally devolved. For instance, in Australia, PECCs have been described as the treatment site for people experiencing such intense suicidality that they require an inpatient admission, but the aims, MoC and clinical practice likely vary (Brakoulias et al., 2010; Huber et al., 2021; Seymour et al., 2020).
Best practice guidelines are important as they help reduce healthcare variation ‘by helping clinicians make the best evidence-based decisions for their patients in a time-efficient manner’ (Guerra-Farfan et al., 2023). Developing such guidelines is particularly difficult in psychiatry because diagnoses have significant overlap (Caspi et al., 2014), and PECCs in particular are designed to focus on behaviour and symptoms rather than any clearly defined condition. With these challenges in mind, to produce a best practice guideline, one must establish an explicit scope and purpose, have stakeholder involvement and go through a process of rigorous development (Brouwers et al., 2016; Song et al., 2022).
The aim of this current study is to take first steps towards developing this scope and purpose by identifying qualitatively who PECCs are treating, for what and using which treatment frameworks. This is a high priority area because suicide prevention remains at the forefront of public interest; PECCs are seen in Australia as the place where intense, active thoughts of suicide are treated (Huber et al., 2021; Seymour et al., 2020); and studies evaluating brief treatments for inpatient suicidality are grossly lacking (Huber et al., 2024). Aims will be addressed by building a qualitative understanding of clinician and manager perceptions of practice in PECCs to answer the research questions: whom do PECCs treat, how and to what purpose, in order to work towards eventually creating a best practice model.
Methods
Ethical standards
Approval was granted by the St Vincent’s Human Research and Ethics Committee (2022/PID00456).
Design
Group and 1:1 semi-structured interviews were analyzed thematically taking a largely inductive orientation with both semantic and latent focus on meaning (Braun and Clarke, 2013), though we used semi-structured interviews which added a deductive element. The framework was mostly critical relativist, with analysts aiming to ‘unpack’ the realities expressed within the data set (Clarke and Braun, 2021). There were 33 interviews of 35 participants across 12 sites (11 of 12 NSW PECCs and 1 Ministry of Health site), with a minimum of 2 and a maximum of 4 participants per site. Only one PECC site in the state could not be contacted. See Supplementary File 1 for the consolidated criteria for reporting qualitative research checklist (COREQ) (Tong et al., 2007).
A qualitative semi-structured interview schedule was developed by the initial research team including practicing Psychiatrist (JH and NG) and Psychologist (AM) researchers.
Setting
The setting was New South Wales (Australia) urban and metro PECC units. See Supplementary Table 1 for a description of staffing and service models.
Participants
Potential participants were Nurses, Social Workers, Psychiatrists, Psychiatry Registrars and Hospital Managers, as well as Ministry of Health staff. Participants had to be working on, or have management responsibilities over, a PECC.
Recruitment and consent
A local Principal Investigator invited staff to participate. Potential participants received information about the study from JH prior to consenting via an online form.
Data collection
Rather than evoking data saturation, this study instead aimed to comprehensively understand practices across all PECCs by purposively sampling all sites (Malterud et al., 2016). Participants from various fields and seniority levels, including medicine, nursing, social work and management, were invited to ensure diverse representation.
Following informed consent, interviews were conducted and audio-recorded via Microsoft Teams by a psychiatrist (JH) or psychologist (AM, at JH’s employment site), with no other people present, between June 2023 and February 2024. Interviews averaged 50 minutes in duration. Participants did not receive compensation.
Data analysis
Interviews were transcribed using Microsoft Teams, cleaned and anonymized by JH. Analysis team included a Psychiatrist (JH), Peer worker (KF), Aboriginal Health Worker (JC), Clinical Nurse Consultant (MB) and Senior Manager/nurse (SE). Steps included: 1) familiarization with all data (JH) or 1-4 transcripts (KF, JC, MB, SE); 2) each member generated initial codes; 3) team meetings compared coding, searching for themes from specific observations to broader generalizations; 4) JH coded all transcripts in NVivo 14, with others coding 1-3 transcripts each, aiming for deeper understanding and assessing code appropriateness. Coding was compared and discussed, leading to theme development and a code-book; 5) team meetings refined themes in detail through a reflexive process, iteratively coding sub-themes and overarching themes, updating the code-book. All transcripts were coded and checked, with 27% double coded. The results were written by the team. A lay summary was returned to participants.
Reflexivity statement
See Supplementary File 2.
Results
Supplementary Table 2 summarizes participant characteristics. One person decided not to participate after initial interest. The number who declined initial invitation was not recorded.
Participants emphasized that PECC units need clear goals, with the primary aim being Harm Minimization, though the specifics were unclear. Themes focused on service-user self-harm and the harm caused by clinicians or the system. In terms of who PECCs are designed to best serve, participants viewed them as appropriate for individuals experiencing suicidality or self-harm, but less appropriate for adolescents, the elderly and overflow patients. Treatment goals included understanding a person’s predicament, managing dysregulated mental states, mapping peoples’ psychosocial situation and addressing what they can and aiming to provide a physical, cultural and clinical environment tailored to manage people ‘in crisis’. Clinicians used a variety of approaches to meet these goals.
What do PECCs aim to do?
Clinicians frequently emphasized the importance of goals of admission and effective interventions (‘If we can’t have an intervention, is there a point in in having them in the unit, if there’s not something to do . . . If that’s not gonna make a difference, then let’s not do it’. P21). The broadest theme pertained to ‘Harm minimization’. (Figure 1).
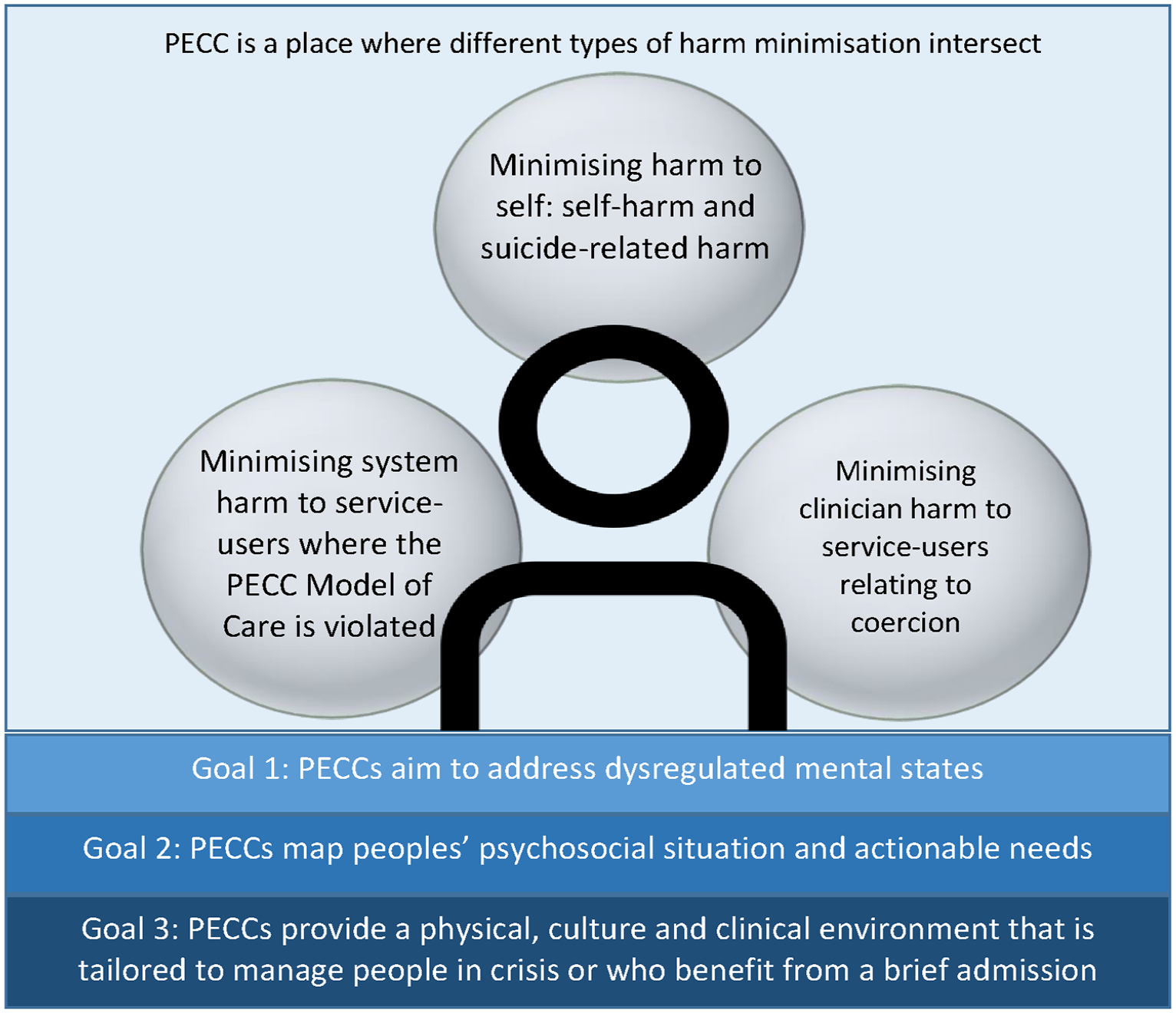
Co-occurring potentials for harm that PECC would ideally minimize and the treatment goals that participants felt may help PECCs minimize harm.
PECC is a place where different types of harm minimization intersect
This was the most frequently coded set of themes and pervaded all admission and management themes. Generally speaking, PECCs were seen to have the goal of ‘harm minimisation’, with multiple definitions of co-occurring ‘harm’ that need to be balanced.
‘So absolutely always take a harm minimization view. There are all kinds of trade-offs in PECC. In fact when you look at those things, there are some where maybe you could do something, but you decide to cut your losses because you think you’re going to get a bigger win in another area’. (P22)
Clinicians were uncertain about whether PECCs should aim to reduce harm related to suicidality (Table 1(1)) given the unpredictability of suicide and self-harm. Admissions were often intended to temporarily reduce suicidal thoughts (Table 1(2)), viewed through the lens of ‘containment’, providing a safe space for self-regulation away from home (Table 1(3)). It was postulated that recurrent admissions might both increase harm through ‘reliance on the service’ and iatrogenic regression for some individuals (Table 1(4)) while, conversely, indicate effective PECC performance because if a person finds an intervention helpful, they are likely to return to receive that intervention again (Table 1(5)). This ambivalence was found both between and within participants.
Quotes pertaining to PECC ‘harm minimization’ goals.
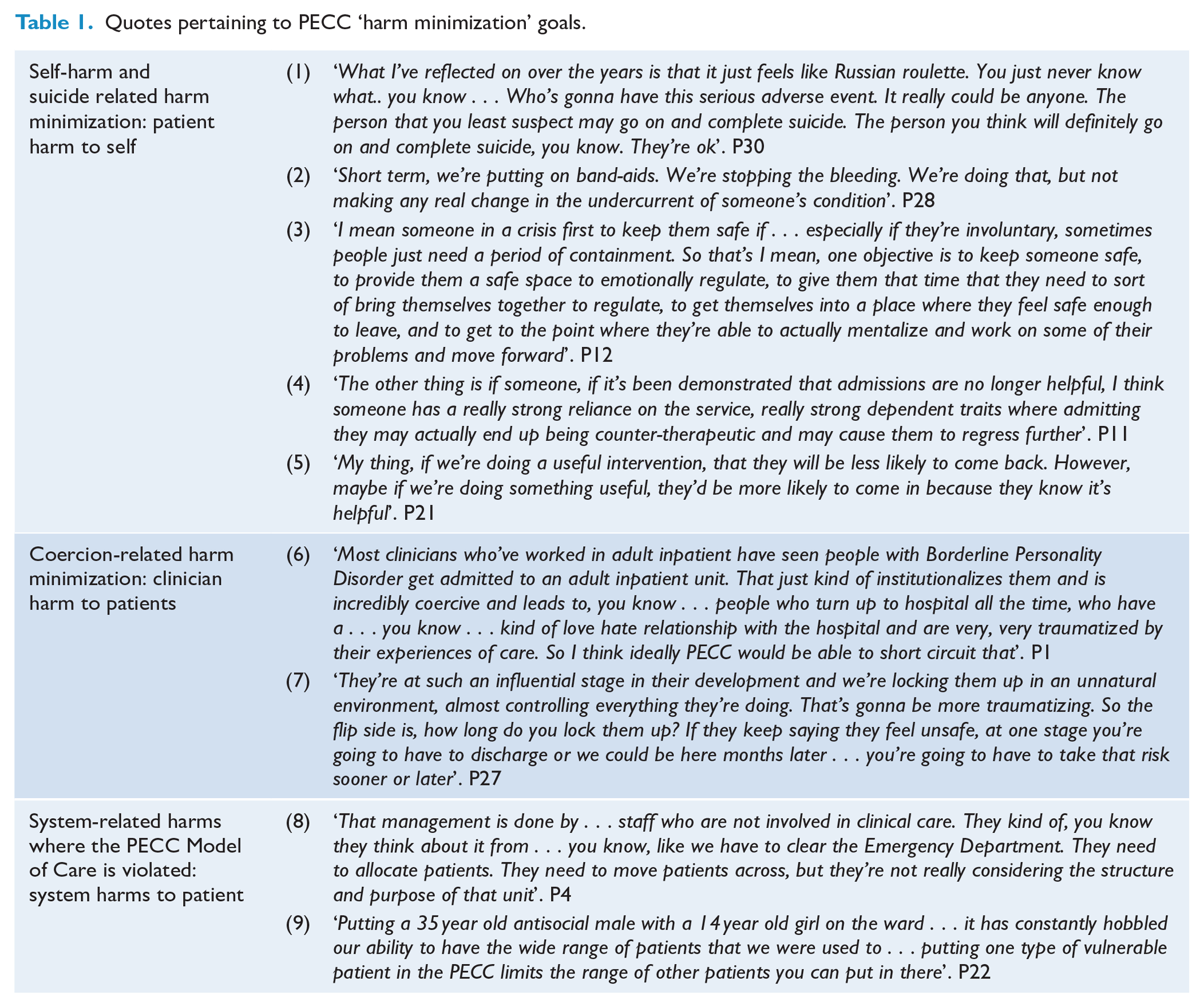
The goal of managing harm from coercion was a priority. PECCs were seen as a way to reduce coercive practices and emphasize autonomy (Table 1(6)). Clinicians expressed distress over using coercion, viewing it as harmful, upsetting and unlikely to impact long-term outcomes (Table 1(7)).
Also, those in system-related roles noted that the PECC model was often misunderstood or ignored, leading PECCs to be used as ‘dumping grounds’ during hospital pressure, which compromised treatment and goals (Table 1(8)). One unit even closed their PECC due to low occupancy, transferring service-users to the general adult ward. Clinicians and managers felt this indiscriminate bed allocation increased harm to both the transferred service-users and those waiting for PECC access (Table 1(9)).
These potentials for harm were considered to co-occur (Figure 1), with the idea that as one risk is contained (eg self-harm) another (eg coercion) can become uncontained (Table 1(7)).
Whom do PECCs treat?
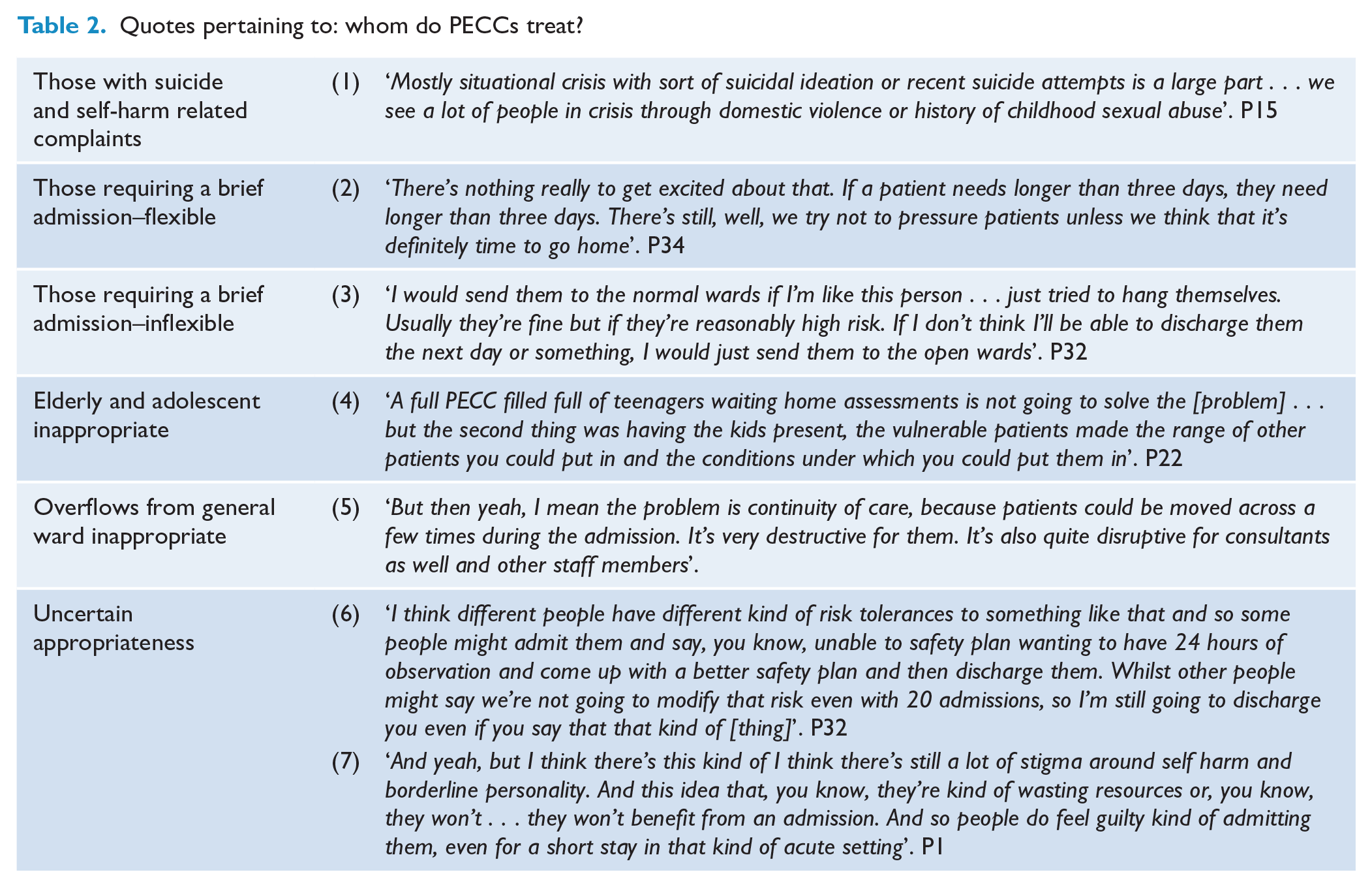
Participants generally agreed whom PECC should be treating, though one PECC had particularly narrow criteria. It was stated by almost all clinicians that PECCs are for people with suicide and self-harm-related complaints and for those who require a brief admission; that PECCs are not for adolescents and elderly people, who should have dedicated, age-appropriate units; and that there is genuine uncertainty about whether some groups should go to PECC.
PECCs are for suicidality and brief admissions
As shown in Figure 2, participants used phrases like ‘suicidality’ and ‘self-harm’ interchangeably to describe mood and behaviour linked to psychosocial distress, often rooted in early life trauma (Table 2(1)). This was clearly, frequently, confidently stated. Participants also noted that PECC admissions were intended to be brief, though the 48 hour stay was flexible (Table 2(2)). However, one PECC strictly enforced the 48-hour limit, avoiding admissions for severe crises, exacerbated Personality Disorder symptoms or complex psychosocial stressors, referring such cases to the Inpatient Unit instead (Table 2(3)). However even when experiencing suicidal crises, elderly and adolescent service-users were seen as inappropriate for PECC. This was because patient mix (e.g. very young, very old, sufferers of trauma, perpetrators of violence and gender sensitivities) was viewed as particularly challenging in these populations (Table 2(4)). Similarly, overflow from general wards or individuals transferred from ED awaiting a general bed were viewed as unsuitable, with this practice considered harmful (Table 2(5)). Clinical uncertainty existed for groups with high readmission rates (Table 2(6)) and Borderline Personality Disorder, especially (according to participants) by teams working after hours and on weekends, unfamiliar with PECC (Table 2(7)).
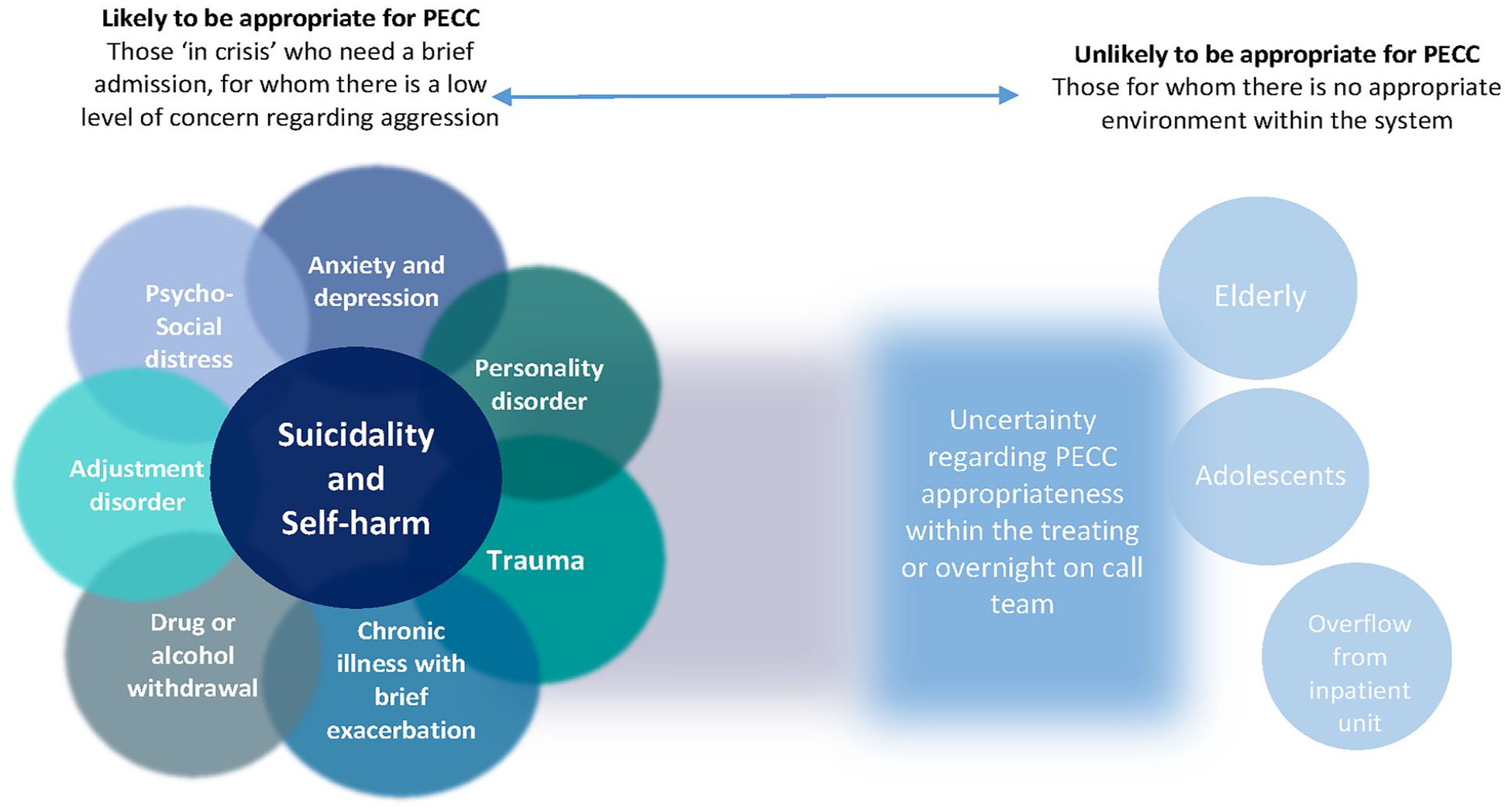
This figure provides a visual conceptualization of participants’ opinions on who PECCs should be for. Opinions lay on a continuum from ‘likely to be appropriate’ to ‘unlikely to be appropriate’, with uncertainty in between.
Quotes pertaining to: whom do PECCs treat?
What are the PECC goals for treatment?
According to participants, to identify goals of treatment one must understand why
‘You can break it down to what registrars call the list of P’s. So they have precipitants, predisposing factors, and perpetuating factors, and then protective factors. And what we need to do during the admission is.. the vast majority of them are in some kind of predicament with a balance between all those P’s and they become . . . overwhelmed in distress, suicidal, you name it. And what we have to do is look at which of these factors might be changeable in some way that helps them get back on a path where they may no longer be in an acute crisis’. P22
However, regarding goals specific to PECCs: three discrete treatment goal themes to help people minimize harm were identified in the data: ‘Managing dysregulated mental states’; ‘PECCs map peoples’ psychosocial situation and actionable needs; and ‘PECCs aim to provide a physical, culture and clinical environment tailored to manage people “in crisis”’.
Managing dysregulated mental states
Almost all clinicians noted that most people are admitted to PECC in a state of severe dysregulation. They describe the goal of reducing the level of dysregulation in order to establish a mental state that is ready to consider next steps (Table 3(1)). Lack of motivation to engage was identified as a central barrier to people moving past a stance of suicidality (Figure 1). Maximizing motivation to participate in treatment was seen as essential (Table 3(2)).
Quotes pertaining to PECC treatment goals.
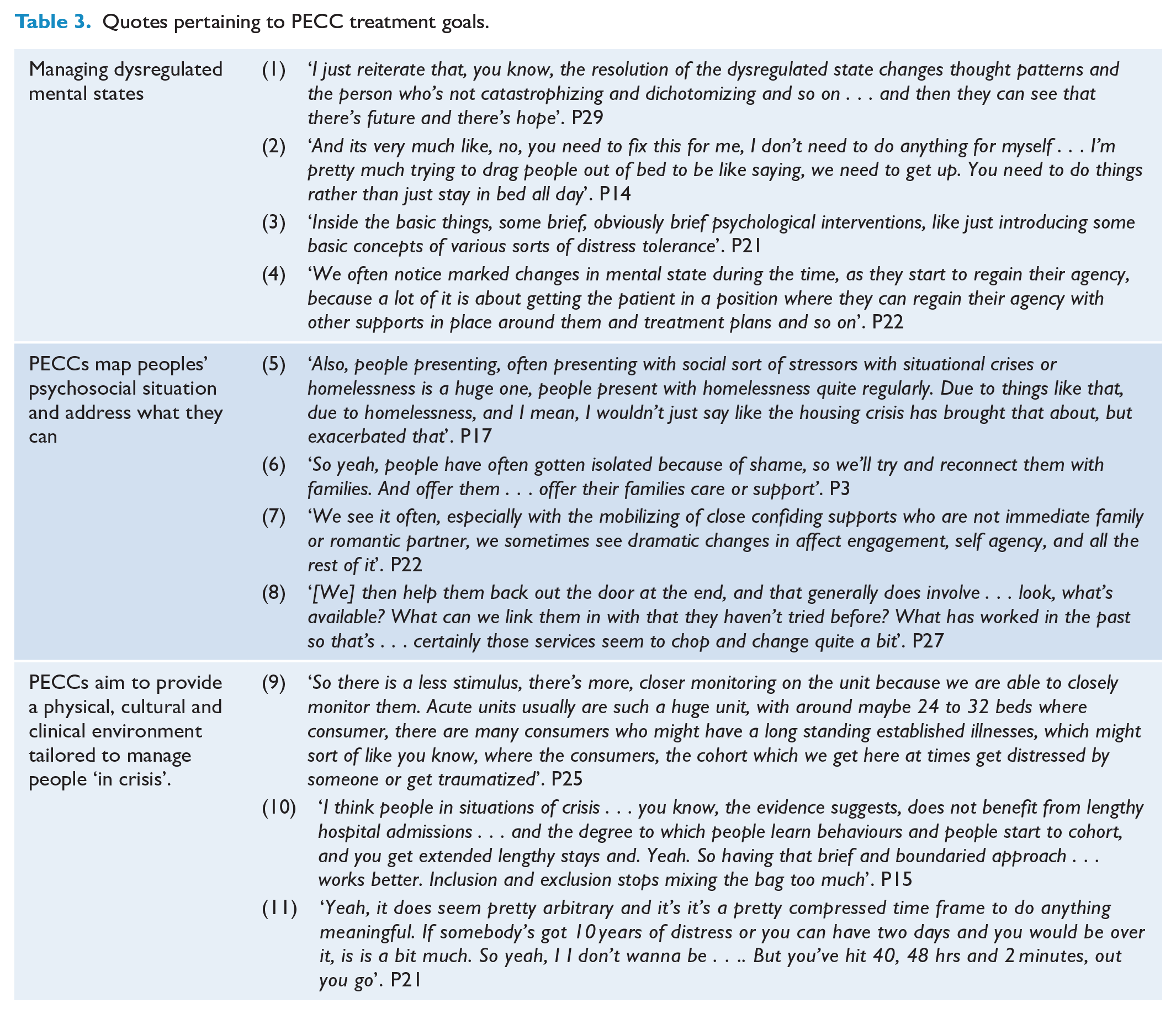
Emotion regulation was identified as an important skill to teach, after addressing dysregulation and motivation. Senior clinicians aimed to introduce emotion regulation skills, to prepare individuals for future emotion management (Table 3 (3)).
Agency and perceived control over their wellbeing were crucial for individuals to act on future plans, indicating emotional regulation, flexibility and readiness for discharge planning. This involved focusing on what they can and cannot realistically control (Table 3(4)).
Mapping peoples’ psychosocial situation and actionable needs
Most clinicians emphasized finding ‘safe’ accommodation as crucial during admission, addressing both physical safety and the psychological impact of homelessness (Table 3(5)). Accommodation issues were highlighted more at some sites, reflecting varying needs across different PECCs.
Connection with families and friends was seen as a major goal of a PECC. They associated a lack of interpersonal connection, due to shame about the person’s actions or illness, and that reconnection is one of the most therapeutic experiences for people who come to PECCs (Table 3 (6)). Some psychiatrists, senior nurses and both social workers said that reconnection allows a person to feel less trapped within the shame and isolation that connected them to a cycle of self-harm, and instead to break free into a state of forward movement (Table 3 (6, 7)) and Figure 1.
All clinicians felt it was important to identify non-hospital management options, as many people were unaware of these alternatives. Providing information and referrals was considered a key aspect of treatment (Table 3(8)).
PECCs aim to provide a physical, cultural and clinical environment tailored to manage people ‘in crisis’
PECCs were seen as less intimidating, quieter and better staffed than Adult Inpatient Wards. Clinicians cited a preference for PECC if their family was in a crisis, believing it was less likely to traumatize patients (Table 3(9)) and Figure 1.
The short PECC length of stay was regarded as positive. Participants were worried that people may regress with longer admissions, ‘learning’ behaviours from other service-users and making their symptoms worse. Participants also noted a ‘regression to the mean’ that seemed to participants to yield high lengths of stay on Adult Inpatient Wards, which participants worried may be damaging to the service-users (Table 3 (10)). However the specific length of stay of 48hrs cited in the NSW Health MoC (Health, 2015) was not widely endorsed. Participants wondered where this specific time period had come from and, except for the sole PECC that chooses their service-user cohort in order to strictly abide by that Key Performance Indicator (KPI), wondered whether it should be longer (Table 3 (11)).
How do PECCs achieve their goals?
Participants described various goal-oriented intervention types, often without distinguishing between general approaches and specific interventions. Some provided detailed responses linking theories with personality styles. Two sites identified specific interventions for particular personality types or psychodynamic processes, with Psychiatrists, Psychiatry Registrars and one Senior Nurse most likely to identify detailed interventions. Psychiatrists and Registrars provided the most framework-related responses, possibly due to the project’s Psychiatrist-led nature. Clinical Directors and managers’ responses were least often coded, as questions focused on clinical practice, not system-related issues.
Responses were grouped into the following categories: ‘Practical interventions’ (eg finding accommodation); ‘Philosophies of care’ (eg Trauma-informed care); ‘Principles of care’ (eg Establish trust); ‘General interventions’ (eg Family work); ‘Medication management’; ‘Manualised therapy frameworks’ (eg Dialectical Behaviour Therapy); and ‘Standalone techniques’ (eg TIPP skills). Figure 3 illustrates these, with Supplementary Table 3 providing further details.
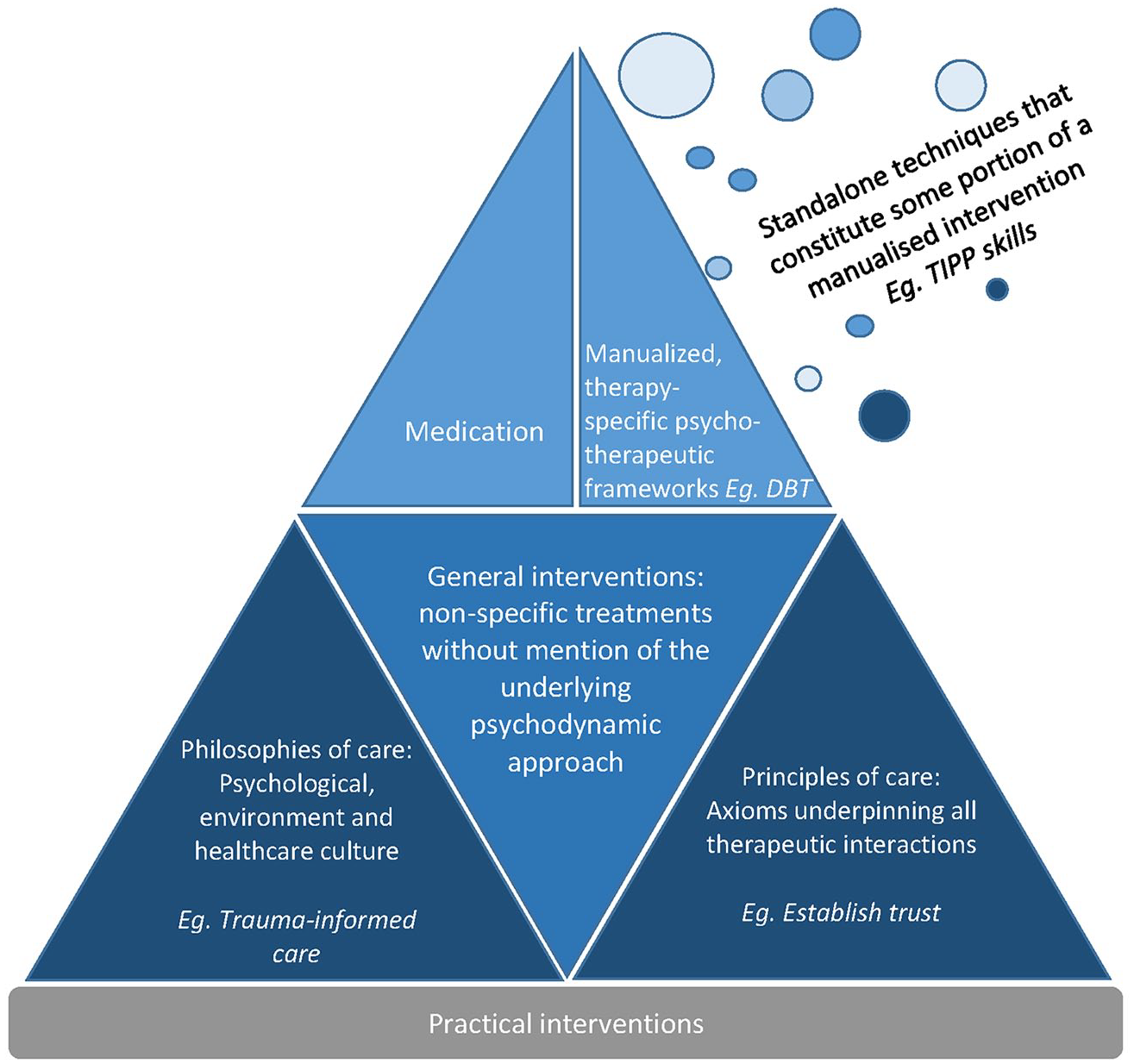
A visual representation of treatment strategies that PECCs use to achieve their goals, according to participants. This figure identifies ‘principles’ and ‘philosophies’ as underlying requirements for the more specific interventions, at the top of the pyramid. Practical interventions reflect all ‘real-life’ changes that service-users need to engage in, or need help with, in order to return more safely to the world outside hospital.
Participants distinguished between PECCs and high-staff respite, wishing for interventions that could be tailored to specific service-user groups (Table 4 (1)). Multiple clinicians lamented the lack of a psychologist, feeling uncertain or unable to offer interventions themselves, and that service-users expected psychological input (Table 4 (2)). However some senior clinicians identified specific interventions without the benefit of a psychologist (Table 4 (3)).
Quotes pertaining to themes of: how do PECCs achieve their goals?
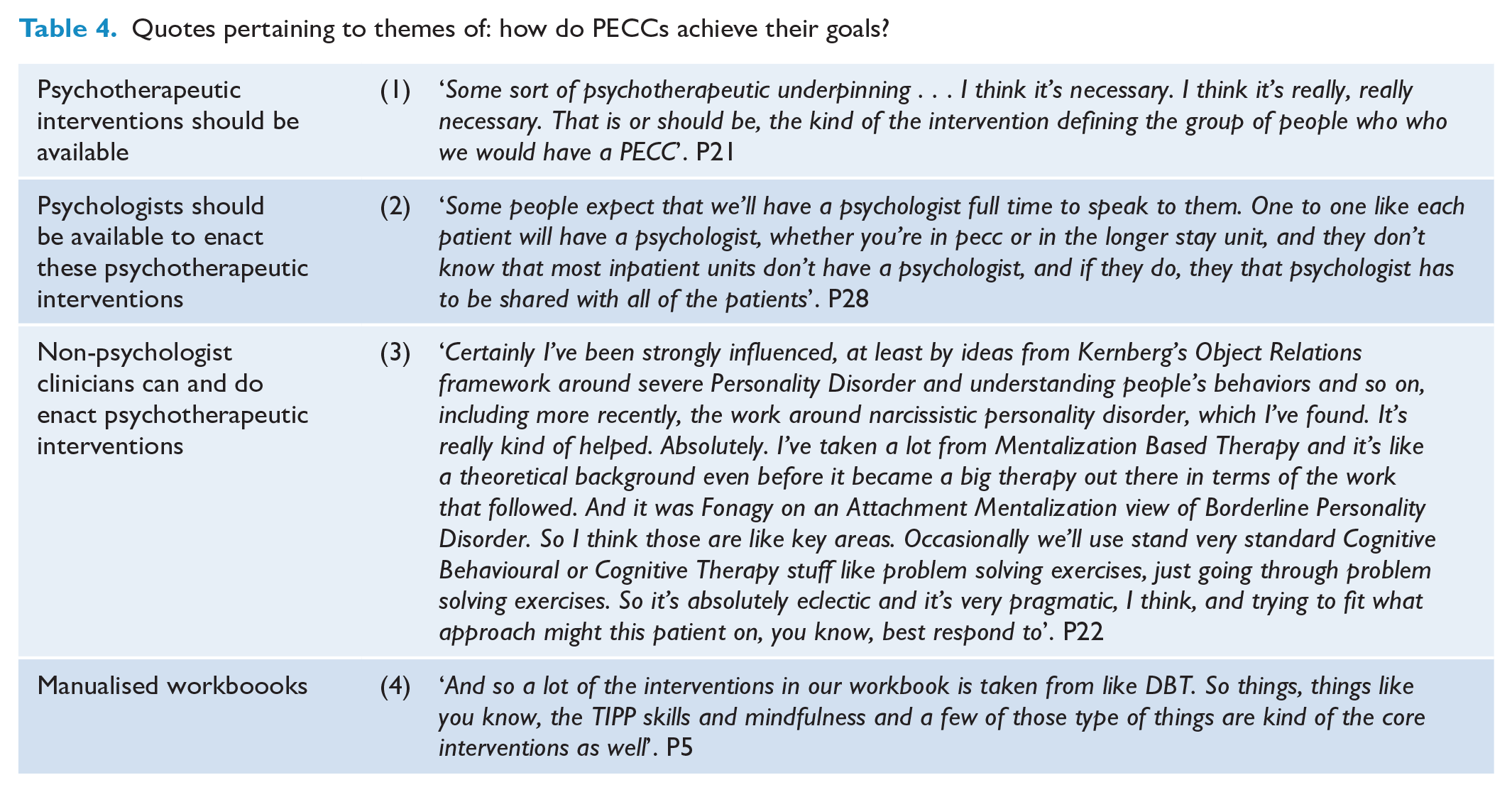
One PECC unit had developed a workbook, while 3 others were in the process (Table 4 (4)). Participants from these units more frequently mentioned on ‘standalone techniques’, potentially because their workbooks contained such interventions.
Discussion
This is the first qualitative assessment of psychiatric short-stay crisis unit staff in Australia, one of few internationally to qualitatively evaluate short-stay crisis units from the clinician perspective (Eckerström et al., 2019; Nehls, 1994), one of only two (to the authors’ knowledge) to include non-nurse healthcare provider participants (Lindkvist et al., 2019) and the only one to investigate units that treat all presenters, not solely those with Borderline Personality Disorder. Given there exists a NSW PECC MoC, we discuss how our results compare to that pre-existing framework, our finding that the primary goal is ‘harm minimization’ via a clearly defined treatment framework, as well as future research and clinical implications.
PECCs no longer reflect the 2015 PECC MoC
This study found that, except one unit, PECCs have diverged from the original ‘48 hr brief observation unit’ described by the PECC MoC as laid out by the NSW Ministry of Health(Health, 2015). The MoC emphasizes ED integration, patient flow and KPIs, including ‘in-reach’ to the ED and ED oversight of non-psychiatric health needs. This appears to have left clinicians to create their own treatment protocols and a natural drift towards the contemporary needs of each service.
Some of the original protocol remains. PECCs still admit low-aggression service-users for brief stays – but now they focus on treating suicidality and crises rather than observation. Many do not offer an assessment, treatment or advice service to ED.
This drift is accompanied by frustration around the 48 hour length of stay expectation. Participants noted that while guidelines drive the expected stay of less than 48 hours (Health, 2015)services users tend to need longer than 48 hours. There is a circularity here that suggests a need to clarify PECC goals. If PECCs primarily treat suicidality, trauma, Personality Disorder and psychosocial crises, a 48 hour length of stay may be inappropriate, lacking evidence for effectiveness in these cases(Berrino et al., 2011; Westling et al., 2019). A parallel could be drawn here with the allocation of 4 hour KPIs in EDs across Australia, which may or may not be appropriate for each specific clinical presentation.
The data also seems to argue against the presumed ‘low acuity’ of PECCs, given the potential high symptom acuity of people experiencing suicidality and severe Personality Disorder.
If PECCs are the primary inpatient treatment facilities for those experiencing suicidality, trauma- or Personality Disorder-related symptoms, this may explain the considerable differences in approach, given the international uncertainty regarding the inpatient treatment of this population (Helleman, Goossens et al., 2018).
Harm minimization could be the overarching purpose, though there is ambivalence about whether PECCs minimize the likelihood of suicide and no clear framework for achieving this
‘Harm minimization’ was a key theme, encompassing various aspects of ‘harm’, with suicide-related harm being most common. The ambivalence regarding whether PECCs do actually prevent suicide mirrors the wider literature (Hofstra et al., 2020; Huber et al., 2024; Zalsman et al., 2016). Harm minimization was often linked to reducing suicidality intensity and seemed to be associated with ideas of respite: a calm environment, being watched by staff and the perception that PECCs may remove options for self-harm. This raises the question of whether hospitals should offer a ‘respite only’ service, and if yes, whether it satisfies the ‘harm minimization’ goal. Although such units exist (Eckerström et al., 2019; Helleman et al., 2014a, 2014b; Helleman, Lundh et al., 2018; Liljedahl et al., 2017; Lindkvist et al., 2019; Westling et al., 2019), the quantitative evidence regarding their utility is limited.
‘Harm minimization’ was a fraught concept, often intertwined with coercion concerns. Tension between these two concepts extended to service-user wellbeing and autonomy, fear of scrutiny from the hospital and the coroner, bed pressure, reigniting traumatic experiences and uncertainty about what specifically containment aimed to achieve. There was a sense of having to balance community expectations of ‘safety’ with clinicians’ experience that people cannot always be ‘kept safe’. Clinicians and executive staff described pressure to offer an effective safety-driven treatment, but this was side by side with the observation that there exists no evidence-based inpatient suicide-specific safety-driven treatment framework.
Nonetheless, harm minimization considerations seemed to drive participant decision-making and could be the bases for discussions regarding a set of expected outcomes. Outcome measures could focus on harm minimization related to clinical, social and system-related issues. Goals associated with harm minimization seem to be associated with practical interventions, managing distress and hospital setup. Analysts viewed themes differently, and this is likely to reflect the different priorities of clinicians, hospitals and governing bodies. Clinicians and peer analysts emphasized patient streaming, staff specialty, practical interventions and environmental impacts; whereas administrators highlighted system-induced harm on service-users due to bed-management decisions and the impact of bed pressure and over-attention to KPIs. If PECCs are to establish an identity, then standardization of goals and outcome measures would be a useful step.
Importantly, though suicide prevention is a worthwhile goal, there is no evidence that PECCs do reduce suicide incidence or indeed keep people safe; however, this nonetheless arises as an internalized expectation of clinicians. This research would suggest that PECC goals may include harm minimization of many kinds, with or without suicide prevention specifically.
Treatment framework is important
Variability in treatment approaches reflects participants’ training, diagnostic lens and treatment preferences. However, PECCs’ unclear purpose and expected outcomes complicate protocol development. This is interesting because participants repeatedly stated that PECCs need clear goals to guide admissions, treatments and outcome measurement. This variability underscores the need to investigate the efficacy of different treatment types for this population.
The frequent call for psychologists in PECCs suggests many clinicians feel unqualified to provide psychotherapies, reflecting the well-known phenomenon that staff feel ill-equipped to manage emergency psychiatric presentations (Bull et al., 2024). This stance was taken by most units, except two where participants specified their own psychotherapy frameworks. Since none had access to a psychologist, it raises the question of whether psychologists are inherently better equipped, or whether any trained Mental Health clinician can manage crises(Choi-Kain and Hersh, 2021; Wharff et al., 2019), notwithstanding the lack of clear definitions or strong evidence for ‘crisis’ interventions in inpatient settings.
Research, policy and practice implications and future directions
Input from service-users is the topic of an upcoming paper; however, based on these results, there is a way forward for PECC and short-stay unit research. Having interviewed clinicians from almost all NSW PECC units and staff from the NSW Health, it is clear the goals of PECCs must be crystalized. These data can be used to establish goals that can then be taken back to the wider psychiatric population for consideration.
A next clear step would beto establish a Core Outcome Set (COS), with standardized outcome measures allowing comparison of outcomes. A COS for psychological therapy trials on acute psychiatric inpatient wards exists (Jacobsen et al., 2024) consisting of 12 overarching outcomes (including self-harm and suicidal thoughts). The applicability of this COS to inpatient crisis psychiatry warrants evaluation(Jacobsen et al., 2024)
Finally, frameworks for the inpatient treatment of people with intense suicide and self-harm ideation need to be co-designed and trialled.
Strengths and limitations
This study captured participants from almost every PECC in NSW, with a good range of multidisciplinary team members, though it did not capture peer worker participants, nor Aboriginal Health Workers. This should be the subject of future research. Analysts were all health researchers or clinicians. A non-health lens would have broadened the analytical perspective. It is likely that participants are highly engaged clinicians, introducing selection bias. Full representation across all sites was chosen to increase completeness, instead of data saturation which could have caused interviews to cease prematurely.
Conclusion
The qualitative data yielded by this study have provided depth and nuance to our understanding of the nature of PECC units and were summarized by a clinician who said, ‘We have to stop thinking about PECCs as being defined by what they
Supplemental Material
sj-docx-1-anp-10.1177_00048674251331466 – Supplemental material for What is the purpose of Psychiatric Emergency Care Centres? A qualitative study of health care staff
Supplemental material, sj-docx-1-anp-10.1177_00048674251331466 for What is the purpose of Psychiatric Emergency Care Centres? A qualitative study of health care staff by Jacqueline Huber, Alyssa Milton, Matthew Brewer, Katherine Fry, Sean Evans, Jason Coulthard and Nick Glozier in Australian & New Zealand Journal of Psychiatry
Footnotes
Acknowledgements
The authors would like to thank the following people who acted as principle investigators: Dr Nicholas Babidge, Dr Tad Tietze, Dr Raphael Fraser, Ms Alison Sutton, Dr Katherine McGill, Dr Kristof Mikes-Liu and Dr Tuni Bhattacharayya.
Author Contributions
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Australian Government through the Australian Research Council’s Centre of Excellence for Children and Families over the Life Course (Project ID CE200100025). AM is partially supported by a Medical Research Future Fund (MRFF) Clinician Researchers Applied Research in Health (GNT 2032279) and a National Health and Medical Research Council (NHMRC) Grant (GNT 2025098).
Ethical Considerations
Approval was granted by the St Vincent’s Human Research and Ethics Committee (2022/PID00456) on 28th April 2022.
Consent to Participate
Participants gave written consent for review and signature before starting interviews.
Data Availability
Due to the nature of the research and resulting ethical restrictions, data are not available
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.