
Abstract

Introduction
Cognitive behavioural therapy for psychosis (CBTp) is an effective psychological intervention for people with psychotic disorders (Turner et al., 2020). Australian guidelines recommend it is routinely available, particularly for persistent positive symptoms (Galletly et al., 2016). Unfortunately access to CBTp remains limited in Australia, with only 10% of people with psychosis receiving CBTp (Harvey et al., 2019).
Traditionally, provision of psychological support for people with psychotic disorders has largely been provided within secondary care, however in our clinical experience individuals with enduring, but stable, psychotic symptoms are increasingly discharged for management within primary care and are thus moving towards private practice for their additional support needs (including for psychological interventions).
This shifting service landscape provides an opportunity for a much-needed increase in access to CBTp, through the private practice psychology workforce. There are no data on the availability of CBTp through private practice psychologists. In order to harness the potential capacity of the private practice psychology sector to increase access to CBTp it is important to understand the willingness of private practice psychologists to treat psychotic symptoms and any potential implementation barriers. This study aimed to assess the proportion of private psychologists willing to accept a referral to treat psychotic symptoms and factors influencing this decision.
Methods
Two hundred and sixty-one Australian private practice psychologists were recruited through advertising with the Australian Psychological Society and on social media. Seventy-seven percent of the sample were female, with a mean of 6 years since registration as a psychologist (SD, 8.11). Twenty-five percent had endorsement as a clinical psychologist with the remainder being generally registered (51%) or provisionally registered (21%). Participants completed an anonymous online survey hosted on QualtricsTM. The survey asked whether participants would accept a referral for someone with active psychotic symptoms for psychological therapy to address those symptoms. Participants then had to rate the importance a number of clinical or contextual factors in their decision. In addition, data was gathered on variables that previous research has found to be relevant in the implementation of CBTp, including training (total hours of learning activities completed in psychotherapy for psychosis), experience (total hours of direct client work completed with people experiencing psychosis), supervision (access to a peer or supervisor with specialist knowledge of psychosis), stigma (The Social Distance Scale, Link et al., 1987), causal beliefs about psychosis (the extent psychologists believed psychosis is caused by biological factors) and therapeutic optimism (optimism towards psychological interventions for psychosis; the Therapeutic Optimism Scale, Byrne et al., 2006).
Statistical analyses were performed using Statistical Package for the Social Sciences (SPSS; Version 29). To assess the variables associated with participants’ likelihood of accepting the referral, binomial logistic regressions were conducted. The impact of registration type (provisional, general or clinical) on acceptance of the referral was assessed using a chi-square test of contingencies.
Results
Only 38% of private practice psychologists indicated that they would accept a referral and offer treatment to address active psychotic symptoms. There were no significant differences in the rate of acceptance of the referral between generally registered, provisionally registered or clinically endorsed psychologists (χ2 = 2.39, p = 0.303). Figure 1 shows how important participants considered various contextual factors to be in making their decision to accept the referral.
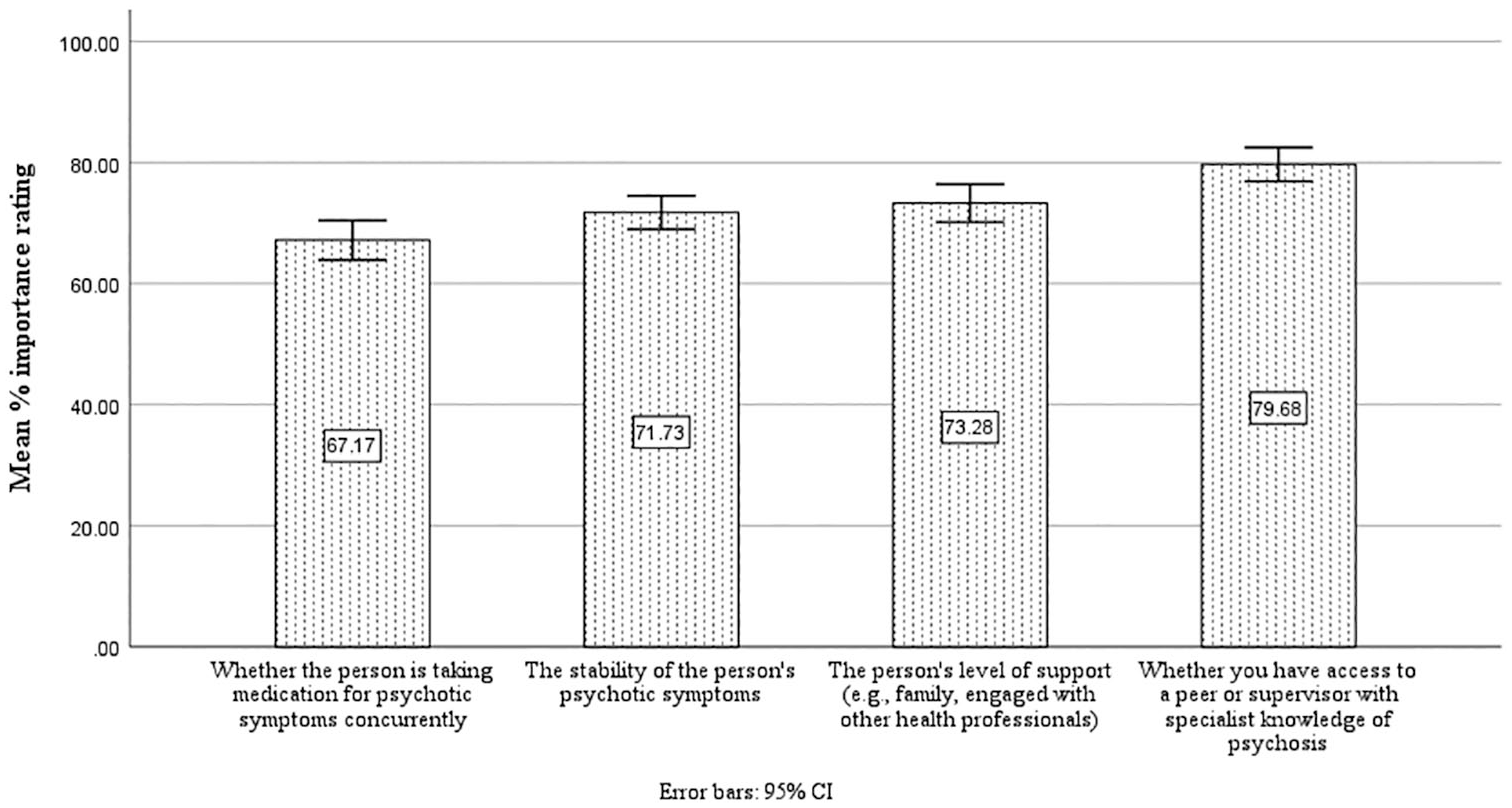
Importance of clinical and contextual factors in psychologists’ decision to take on a referral to treat psychotic symptoms.
Participants reported a median of 20 hours of experience working with people with psychosis (IQR, 98) and 5 hours of formal training (IQR, 15). Access to a peer or supervisor with specialist skills in working with psychosis was available to 43.3% of the sample. The sample showed a relatively high desire for social distance from people with psychosis (mean 1.54 out of 3, SD 0.56) compared to a previous sample of healthcare workers (Reddyhough et al., 2021). Causal beliefs trended towards the belief that psychosis is biological in nature with psychotic symptoms rated on average as 58.47% (SD, 18.38) biological in nature. Therapeutic optimism was above the midpoint (mean 38.80 out of 50, SD 6.47) in our sample; thus, on average, participants believed that individuals with psychosis could be helped by psychotherapy.
The omnibus model for the logistic regression analysis was statistically significant, χ2 (df = 6, N = 261) = 76.01, p < 0.001, Cox and Snell R2 = 0.25, Nagelkerke R2 = 0.34. The model was 77% accurate in its predictions of accepting the referral for psychosis treatment. Hosmer and Lemeshow results confirmed the model was a good fit for the data, χ2 (df = 8, N = 261) = 10.56, p = 0.228.
Table 1 shows the predictor coefficients for the logistic regression model. Experience, stigma, causal beliefs and therapeutic optimism were significant predictors of accepting the referral. As experience increased, the participant was more likely to accept the referral. Moreover, if the score on the measure of therapeutic optimism increased by one unit, the participant was 1.10 times more likely to accept the referral. If the score on the measure of stigma increased by one unit (i.e. greater desire to distance themselves from individuals experiencing psychosis), there was a predicted 40.7% reduction in the probability of accepting the referral. Finally, if the score on the measure of causal beliefs increased by one unit (i.e. greater belief that psychosis is biological in nature), there was a predicted 2% reduction in the probability of accepting the referral.
Predictor coefficients.
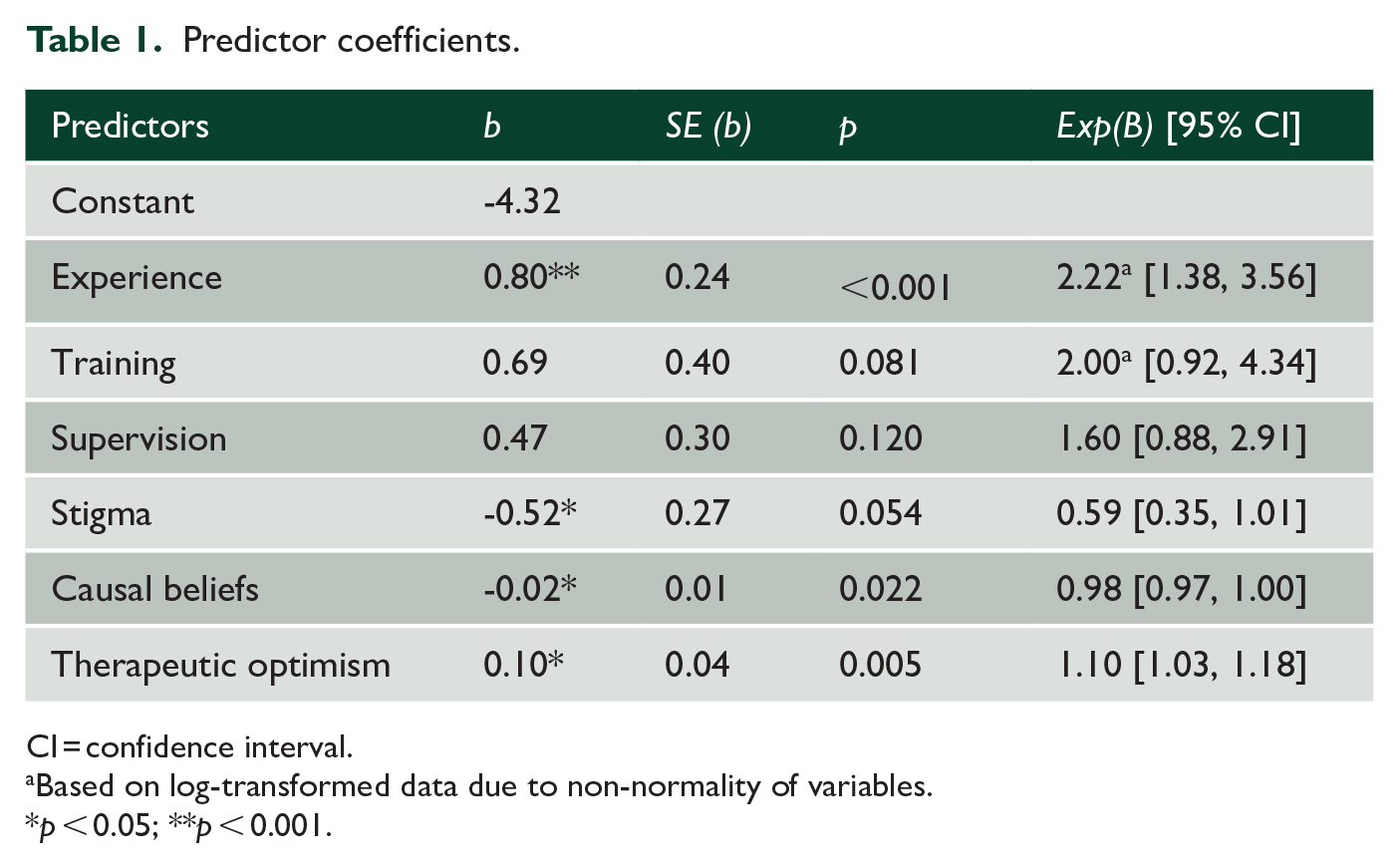
CI = confidence interval.
Based on log-transformed data due to non-normality of variables.
p < 0.05; **p < 0.001.
Discussion
The majority of private practice psychologists indicated they would not accept a referral to treat psychotic symptoms (62%), suggesting a shortage of service provision for people with psychosis in private practice. There were no significant differences between provisionally, generally or clinically registered psychologists. These findings suggest that if private practice psychologists are to be part of the solution to increasing access to psychological therapies for psychosis, there is a need to upskill our private practice psychology workforce.
Results suggest that private practice psychologists have somewhat limited training and experience in psychological therapies for psychosis and that experience in particular is a predictor of taking on referrals for CBTp. Increasing practicum experience with psychosis in Australian postgraduate psychology programmes should be a priority in the goal of upskilling the workforce. Previous research has indeed indicated that the majority of psychologists (75%) finish their professional training without practicum experience with psychosis (Rackemann et al., 2024).
Private practice psychologists showed relatively high levels of stigma but did largely recognise the role of psychological factors in psychosis and have optimism that psychological approaches could be helpful for this population. These beliefs and attitudes were also predictive of taking on a referral for CBTp. As such, training and interventions that reduce stigma, increase awareness of the efficacy of psychological interventions for psychosis and educate on the role of psychological factors in psychosis would be a valuable focus in postgraduate psychology training and as continuing professional development opportunities offered to private practice psychologists.
It is also key to note that clinical and contextual aspects of the referral were important considerations for participants. It was important that psychologists felt that that they had access to supervisory support and that clients were symptomatically stable, had support systems in place and were taking medication. Future research can explore clinical and systemic barriers in more detail to inform changes needed to support the provision of CBTp in private practice settings.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This project was supported by student research funds from the School of Health, the University of the Sunshine Coast.