
Abstract

Medicinal cannabis use in Australia has rapidly expanded from its originally intended use in treatment-resistant conditions (e.g. Lennox-Gastaut syndrome, multiple sclerosis) (Dawson et al., 2025), to the prescription of high-concentration Δ-9-tetrahydrocannabinol (THC) products to treat mental health conditions including anxiety, depression and post-traumatic stress disorder (Australian Government, 2025). Simultaneously, single-purpose dispensaries are increasing, in which cannabis is prescribed to the exclusion of all other medications, despite prescribing guidelines explicitly stating that medicinal cannabis should never be used as a first-line treatment. It is doubtful that these dispensaries of medicinal cannabis lack conflicts of interest, given that they only prescribe and dispense a single type of pharmaceutical treatment (AHPRA, 2025) when several treatment options may be suitable. Some dispensaries advertise their services on social media in breach of Therapeutic Goods Administration (TGA) regulatory guidelines (Lim et al., 2025). These marketing efforts have arguably created an environment in which patients pursue cannabis prescriptions rather than pursuing a physician’s diagnosis of their medical condition followed by the provision of an appropriate treatment (Department of Health, Disability and Ageing, 2024).
The Australian Health Practitioner Regulatory Authority (AHPRA) has concluded that some single-purpose dispensaries engage in improperly short consultations, provide medical cannabis prescriptions without a legitimate indication and engage in a range of other breaches of guidelines (AHPRA, 2025). The current study assessed the extent of these practices by systematically searching for websites offering medicinal cannabis and analysing the likely experience of prospective patients who access these websites.
Methods
We conducted a systematic search of Google Maps and Google Search to identify websites which advertise medicinal cannabis services in Australia. The search terms used were medicinal cannabis terms combined with location terms (‘Medical Cannabis Clinic’, ‘Medical Cannabis Shop’, ‘Hemp Clinic’, ‘Hemp Shop’, ‘Herbal Clinic’, ‘Herbal Medicine Clinic’, ‘Medical Marijuana Clinic’, ‘Medical Marijuana Shop’ combined with ‘Brisbane’, ‘Gold Coast’, ‘Newcastle’, ‘Sydney’, ‘Melbourne’, ‘Canberra’, ‘Hobart’, ‘Launceston’, ‘Adelaide’, ‘Darwin’, ‘Alice Springs’, ‘Perth’ and ‘Broome’).
We analysed (1) the type of business (i.e. single-purpose dispensaries or standard GP clinic); (2) the type of appointments (i.e. telehealth-only, in-person only or both); (3) the duration and cost advertised; (4) delivery options; (5) whether a health summary or referral was required and (6) if a pre-screening questionnaire was present. Fisher’s exact test was used to test for differences between types of businesses. As these data are available in the public domain, the study was granted exemption from a human research ethics approval.
Results
Type of clinics and appointments
Among the 55 medicinal cannabis websites identified, 35 (64%) were single-purpose dispensaries, and of those, 25 offered telehealth-only consultations (see Table 1). Telehealth-only consultations were significantly more likely to be offered by single-purpose dispensaries than standard GP clinics (p < .001).
Characteristics of Single-Purpose Dispensaries compared to standard General Practitioner clinics.
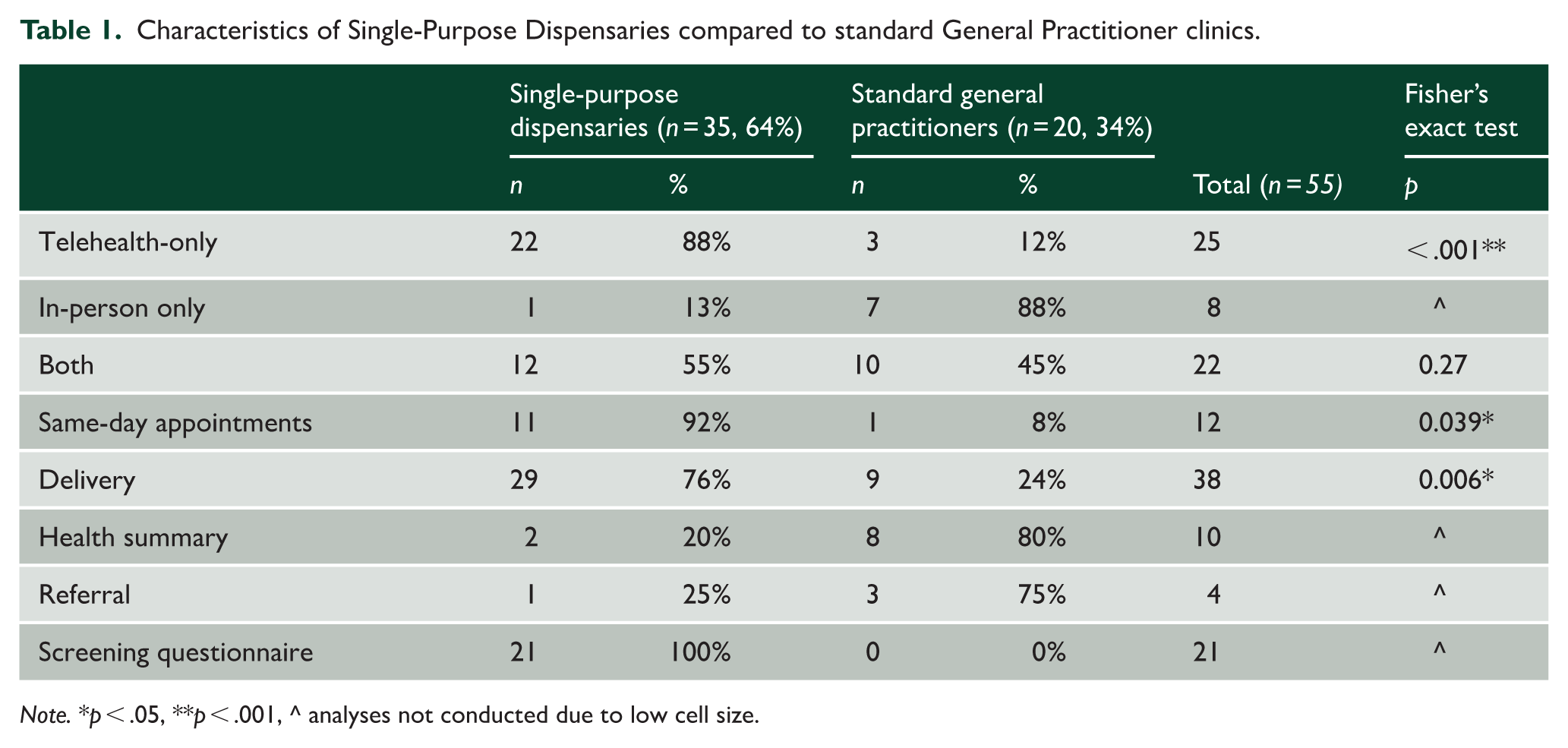
Note. *p < .05, **p < .001, ^ analyses not conducted due to low cell size.
Consultation characteristics
Cost of initial appointments was advertised on 37 websites and ranged from $0 to $204 (median $79).
Among websites that advertised the duration of initial medicinal cannabis consultations (n = 23), the minimum duration was 10 minutes. Same-day appointments were offered by 12 websites, and this was significantly more likely to be offered by single-purpose dispensaries than standard GP clinics (p = .039).
Delivery
Two thirds (69%) of websites (n = 38) offered a delivery service for prescribed medicinal cannabis products. This service was significantly more likely to be offered by single-purpose dispensaries (p = .006).
Medical history
Only four of the 55 websites requested a referral from the patient’s usual medical practitioner or specialist. Over a third (21 websites, all single-purpose dispensaries) had screening questionnaires for patients to check their ‘eligibility’ for whether medicinal cannabis could be prescribed.
Discussion
Our study found that some medicinal cannabis clinics in Australia offer free consultations, same-day appointments and home delivery of medicinal cannabis. These practices facilitate a rapid progression from a patient contemplating a medicinal cannabis prescription to consumption, often occurring without involvement from the patients’ usual medical practitioners and in the absence of referrals or health summaries. These marketing strategies resemble the digital marketing employed by the alcohol industry in recent years, which also offer streamlined online services and delivery, to enable swift progression from initial interest to product consumption (Carah and Brodmerkel, 2021).
Our investigation indicates that most single-purpose dispensaries offer telehealth appointments and are more likely to do so than traditional GP clinics. Telehealth appointments in this context may function as another marketing strategy by reducing the need for an in-person appointment, particularly when providing costless, same-day appointments and home delivery. Many medicinal cannabis clinics advertise brief initial appointments, some as short as 10 minutes. It seems highly improbable that a consultation of this length would be sufficient to meet AHPRA guidelines that patients be assessed thoroughly prior to prescribing medicinal cannabis (AHPRA, 2025). These prescribing guidelines explicitly caution that brief online consultations are inadequate for conducting comprehensive assessments of a patient’s physical and mental health history.
Evidence from an Australian Early Psychosis service has identified a rise in referrals where the onset of psychosis occurred in temporal proximity to medicinal cannabis prescription (Lupke et al., 2023). The service also reported cases of patients who continued to obtain prescriptions after psychosis onset, as well as those who received a new prescription for high THC products following the onset of psychosis. These concerns are shared by AHPRA, which has highlighted failures to properly assess patients, resulting in psychotic episodes and other serious adverse outcomes (AHPRA, 2025; Lupke et al., 2023). It is also of concern that less than 10% of the medicinal cannabis clinics require a referral and only ~18% require a health summary. This means that the safety of prescribing rests entirely with the prescribing service and the practitioner’s assessment of the patient in often very brief consultations. Existing reports raise concerns that, during such consultations, some practitioners failed to inquire about other medications currently prescribed that may affect health outcomes independently or interact with medicinal cannabis. There is also often an underestimated risk of disordered cannabis use in medical settings, despite the literature finding that cannabis use disorder has an estimated prevalence of ~25% among medicinal cannabis consumers (AHPRA, 2025; Chopra, 2017; Dawson et al., 2024).
Taken together, our findings suggest that medicinal cannabis prescriptions in some single-purpose dispensaries differ fundamentally from other medications in that the selection of the medicine precedes diagnosis. The current system within which medicinal cannabis is being prescribed may be contributing to the risks associated with the dispensation of cannabis based on patients’ perceived needs rather than a medical indication. The abundance of websites offering medicinal cannabis in Australia (greater than 50 based on our search) is of concern because it suggests a breadth of avenues from which to seek a specific product (i.e. medicinal cannabis) rather than consulting a practitioner for a diagnosis and receiving evidence-based care for a medical condition, which may or may not include medicinal cannabis. To this end, the term ‘prescribed cannabis’ may be a more accurate descriptor compared to ‘medicinal cannabis’ within the Australian context.
This research has the limitation that our web search may not be representative of all practitioners who prescribe cannabis in Australia because it only presents information from clinics that advertised cannabis as a medicinal product and are indexed by Google. It is, therefore, not possible for us to comment on clinics that prescribe medicinal cannabis but do not explicitly state so on their website.
Regulatory agencies, professional bodies and Australian health practitioners must collaborate to ensure that medicinal cannabis prescribing practices are in line with those governing other prescription medicines and that appropriate clinical oversight is maintained to ensure patient safety.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: D.D.: Funded by The University of Queensland’s Research Training Stipend. C.L.: No funding for this study. A.G.: No funding for this study. J.L.: No funding for this study. V.L.: No funding for this study. W.H.: No funding for this study. D.S.: No funding for this study.