
Abstract
Objective:
We aimed to assess the alignment in defining and measuring psychosocial disability and/or mental health challenges across major Australian national mental health data sources.
Methods:
We reviewed the definition and measurement of psychosocial disability and mental health challenges in two stages. First, we examined the data items across five national data sources: the Survey of Disability, Ageing and Carers (SDAC), the National Health Survey (NHS), the National Study of Mental Health and Wellbeing (NSMHW), the Census and the National Disability Insurance Scheme (NDIS) administrative data. In the second stage, we analysed the prevalence of psychosocial disability and mental health challenges across the datasets.
Results:
The definition and measurement approaches for psychosocial disability and mental health challenges vary across data sources, reflecting differences in the conditions included and the purpose for which data were collected. Psychosocial disability is inconsistently defined: broad population surveys (SDAC, NHS) include neurodevelopmental and neurodegenerative conditions, whereas the NDIS captures only severe mental illnesses with substantial functional impairment. Prevalence across Australia varied widely from 42.9% for lifetime mental disorders (NSMHW) and 26.1% for long-term conditions (NHS), down to 6% when strictly defining psychosocial disability (SDAC).
Conclusions:
There are variations in definitions and measurement across major Australian mental health data sources with respect to conditions captured in the datasets and the definitions used. Researchers and policymakers should therefore critically appraise – and where possible adjust for – these variations when using these data to inform strategic decisions and resource allocation.
Keywords
Introduction
Disability arising from mental health challenges accounts for a significant proportion of global disability, contributing roughly one-sixth of all years lived with disability (Global Burden of Disease Mental Disorders Collaborators, 2022). The associated economic impact is significant, with the global burden of mental health challenges estimated to cost approximately US$5 trillion annually (Arias et al., 2022). In Australia, mental health challenges and suicide are estimated to cost the economy around AU$220 billion each year (Productivity Commission, 2020). In this paper, we use the term ‘mental health challenges’ as a preferred descriptor, reflecting guidance from lived-experience advisers; where datasets or references use other terms, such as ‘mental disorder’, we report them as presented.
The term ‘severe mental illness’ has long been used to describe mental health challenges associated with enduring and significant functional impairment. It is defined in the literature as a mental disorder lasting 2 years or more and causing significant functional impairment, indicated by a Global Assessment of Functioning (GAF) score of 50 or below (Ruggeri et al., 2000). While closely related to a severe mental illness, ‘psychosocial disability’ is conceptually distinct because of the emphasis on the disabling impact of the illness; however, in practice, the boundaries between the two are often blurred (Hamilton et al., 2020), and the distinction remains ambiguous across policy and service contexts (Australian Institute of Health and Welfare, 2022; Choi et al., 2025; National Mental Health Consumer & Carer Forum, 2011; Shelby-James et al., 2023).
Over the past decade, the concept of psychosocial disability has gained increasing prominence in Australian mental health and disability policy, particularly in the context of the National Disability Insurance Scheme (NDIS; Shelby-James and Rattray, 2025; Smith-Merry et al., 2018). This terminology builds on earlier Australian practice rooted in psychosocial rehabilitation approaches. For example, in Victoria, during the 1990s, Psychiatric Disability Rehabilitation and Support Services operated within the mental health system, integrating psychiatric services within a disability framework and psychosocial rehabilitation approaches (Victorian Department of Human Services, 2004). ‘Psychosocial’ elements of mental health supports have been delivered through community-based rehabilitation, recovery support, housing assistance and social participation programmes funded by state and territory mental health systems (Rosenberg and Harvey, 2021).
Despite being long-standing frames for targeting policy and services, terminology related to psychosocial disability and severe mental illness has been inconsistently defined and applied across service systems. As a result, data collections often fail to distinguish between clinical diagnoses and the disabling impacts of mental health challenges (Threlfall et al., 2025). This lack of clarity affects how individuals are identified, coded and represented in national datasets – leading to gaps, overlaps and misclassification. As a result, the data system struggles to accurately capture the distinct experiences and support needs of people with psychosocial disability, limiting its usefulness for planning, evaluation and policy development (Williams and Smith, 2021).
These data limitations also constrain the design and delivery of effective responses. Preventing the disabling impacts of mental health challenges requires coordinated, evidence-based interventions that are responsive to individuals’ evolving needs (England et al., 2015). However, Australia’s current mental health data systems face well-documented challenges related to fragmented definitions, inconsistent measurement approaches and limited integration across services and jurisdictions (Health Policy Analysis, 2014; Pagliaro et al., 2024). Therefore, the development and implementation of effective, targeted policy strategies to prevent and manage psychosocial disability must be grounded in a more coherent and harmonised national data landscape. This study aims to contribute to addressing these challenges by systematically examining how mental health challenges and psychosocial disability are defined and measured across major Australian national surveys and the NDIS administrative dataset.
Methods
Data sources
We drew on five national data sources: the Census of Population and Housing (Census) 2021, the Survey of Disability, Ageing and Carers (SDAC) 2022, the National Health Survey (NHS) 2022, the National Study of Mental Health and Wellbeing (NSMHW) 2020–2022 and the NDIS participant dataset.
The Census and the three surveys are conducted by the Australian Bureau of Statistics (ABS) and largely use standardised instruments to ensure comparability of data across time periods. The NDIS dataset is an administrative database derived from the government’s disability insurance scheme. We extracted its operational definition of psychosocial disability and related eligibility criteria as a key indicator of how mental health conditions are included within a programme that uses psychosocial disability as a designated eligibility category.
Sampling and design
The Census aims for complete population coverage. For the SDAC, NHS and NSMHW, the ABS uses stratified multistage sampling of households to ensure national representativeness across states and territories (excluding very remote areas) (ABS). For the SDAC, the sample includes two components: private dwellings and cared-accommodation facilities. Demographic information was collected for all usual residents, along with details about the dwelling. In the NHS, all usual residents of private dwellings in Australia were eligible. Households were randomly selected, with one adult aged 18 years or over and one child aged 0–17 years selected to complete individual questionnaires. For children aged 0–14 years, a parent or guardian answered the questions on their behalf. For the NSMHW, one person aged 16–85 years was randomly selected in each household to complete the survey questionnaire. Parental consent was sought for participants aged 16–17 years.
The NDIS dataset captures all psychosocial disability applicants, both eligible and ineligible. The dataset includes information on a range of socioeconomic and demographic characteristics, as well as the disorder type recorded using International Classification of Diseases (ICD) classification for each applicant. The NDIS was the first to utilise the term ‘psychosocial disability’ and continues to play a central role in shaping its definitions. Including the NDIS dataset therefore provides a benchmark for identifying the population in other data sources. Further details on the purpose and methods of data collection are provided in Table 1.
Overview of datasets’ objectives, data-collection methods and frequency.
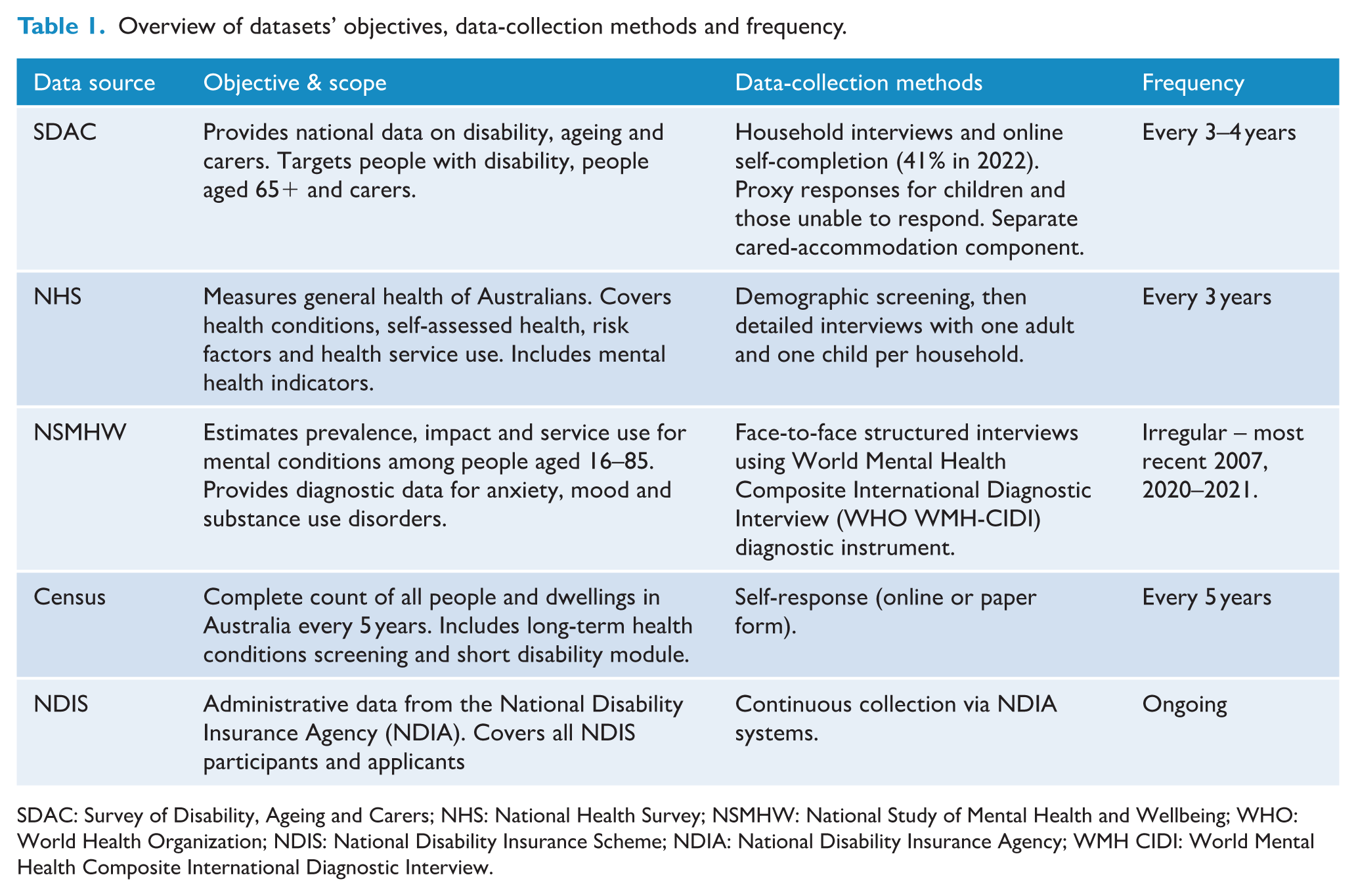
SDAC: Survey of Disability, Ageing and Carers; NHS: National Health Survey; NSMHW: National Study of Mental Health and Wellbeing; WHO: World Health Organization; NDIS: National Disability Insurance Scheme; NDIA: National Disability Insurance Agency; WMH CIDI: World Mental Health Composite International Diagnostic Interview.
Measurements
We evaluated definitions and measurements in two stages. First, we reviewed each survey’s data items to determine how psychosocial disability and/or mental health challenges were defined and measured. To do this, we systematically examined four key elements: diagnostic criteria, temporal scope, functional impact and severity grading. These elements represent common elements of definitions of severe mental illnesses described in the literature (Ruggeri et al., 2000). Ruggeri et al. (2000) highlight diagnosis, functioning and duration in their three-dimensional definition of severe mental illnesses. In comparison to this definition, we split functioning into both impact and severity in our analysis to better capture these different elements where this was possible. For diagnostic criteria, we identified disorders included in each dataset and the instruments used to ascertain them. The temporal scope assessment considered a timeframe where this was used within a dataset as part of the identification of disability or long-term health condition. Finally, where the definitions included a ‘severity’ grading, we evaluated the way severity was framed, e.g., the extent to which each data source quantified intensity or impairment.
In the second stage, we analysed the prevalence of psychosocial disability and mental health challenges using the respective definitions and measures within each data source. We also examined the components of each measure to highlight key elements supporting the operationalisation of psychosocial disability and mental health challenges across surveys.
Statistical analysis
The analysis was conducted within the ABS DataLab environment using the Person Level Integrated Data Asset (PLIDA) platform. For the SDAC, NHS and NSMHW datasets, we applied the person-level survey weights provided by the ABS to produce nationally representative prevalence estimates. Replicate weights were used to estimate standard errors and confidence intervals, ensuring accurate variance estimation under each survey’s complex design (ABS). The analysis took a descriptive approach to estimate point prevalence, stratified by age group and gender. We used the age groups (0–14, 15–24, 25–44, 45–64, 65 and above) and gender to disaggregate prevalence estimates. See the Supplementary File 1 for prevalence estimates by age group and gender. All analyses were done using Stata (version 18).
Results
Survey of Disability, Ageing and Carers
Measurement approaches
Psychosocial disability is defined operationally within the SDAC as a condition that includes experiencing a nervous or emotional condition that restricts everyday activities; having a mental illness or condition that requires help or supervision; memory problems or periods of confusion that limit daily functioning or social or behavioural difficulties that interfere with participation (Supplementary File 2).
In terms of disability positioning, the SDAC adopts a functional, International Classification of Functioning, Disability and Health – World Health Organisation (ICF)-aligned approach, identifying disability through limitations, restrictions or impairments that affect everyday activities and are expected to last, or have already lasted, 6 months or more (Table 2). Using this functional approach, disability is assessed primarily through limitations in activities and participation rather than diagnosis alone. In the context of psychosocial disability, this means that the underlying condition may not always be a mental health condition; any condition that leads to a nervous or emotional condition, a mental illness, memory problems or periods of confusion or social and behavioural difficulties can result in classification as a psychosocial disability. Severity of disability was measured across six categories related to limitations in core activities: profound limitations, severe limitations, moderate limitations, mild limitations and no limitations.
Summary of mental health conditions and/or disability: definitions and measurement approaches, temporal scope, functional impact, severity grading and disability positioning and definition within each dataset.
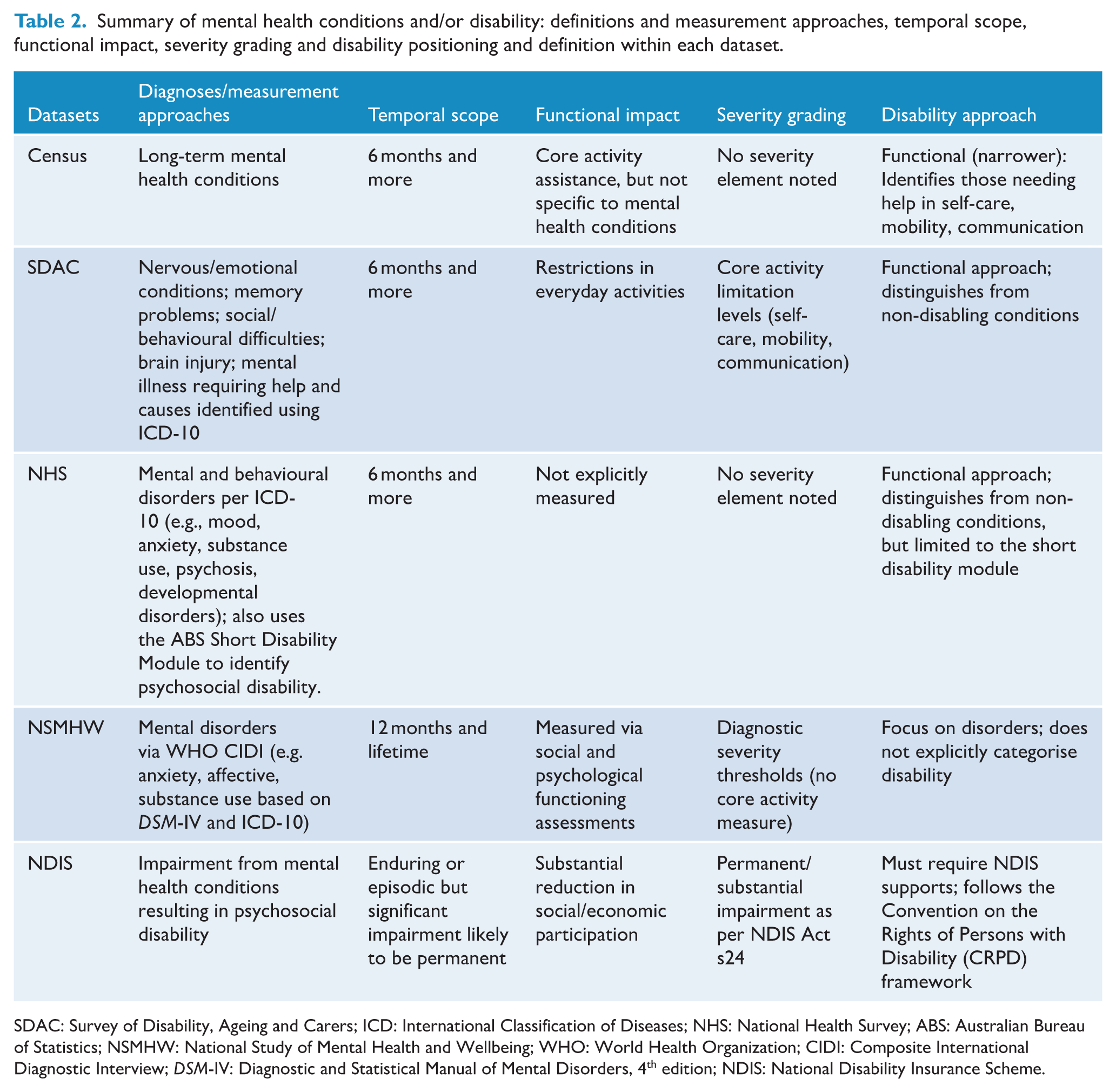
SDAC: Survey of Disability, Ageing and Carers; ICD: International Classification of Diseases; NHS: National Health Survey; ABS: Australian Bureau of Statistics; NSMHW: National Study of Mental Health and Wellbeing; WHO: World Health Organization; CIDI: Composite International Diagnostic Interview; DSM-IV: Diagnostic and Statistical Manual of Mental Disorders, 4th edition; NDIS: National Disability Insurance Scheme.
Psychosocial disability SDAC estimates
The overall prevalence of psychosocial disability was estimated at 5.97% (95% CI: 5.58–6.39) (Table 3). Among the different components of psychosocial disability, a nervous or emotional condition that restricted everyday activities was most commonly reported (3.78%, 95% CI: 3.40–4.19) (Table 3).
Prevalence estimates of mental health conditions and/or disability SDAC, NHS, NSMHW and the census.
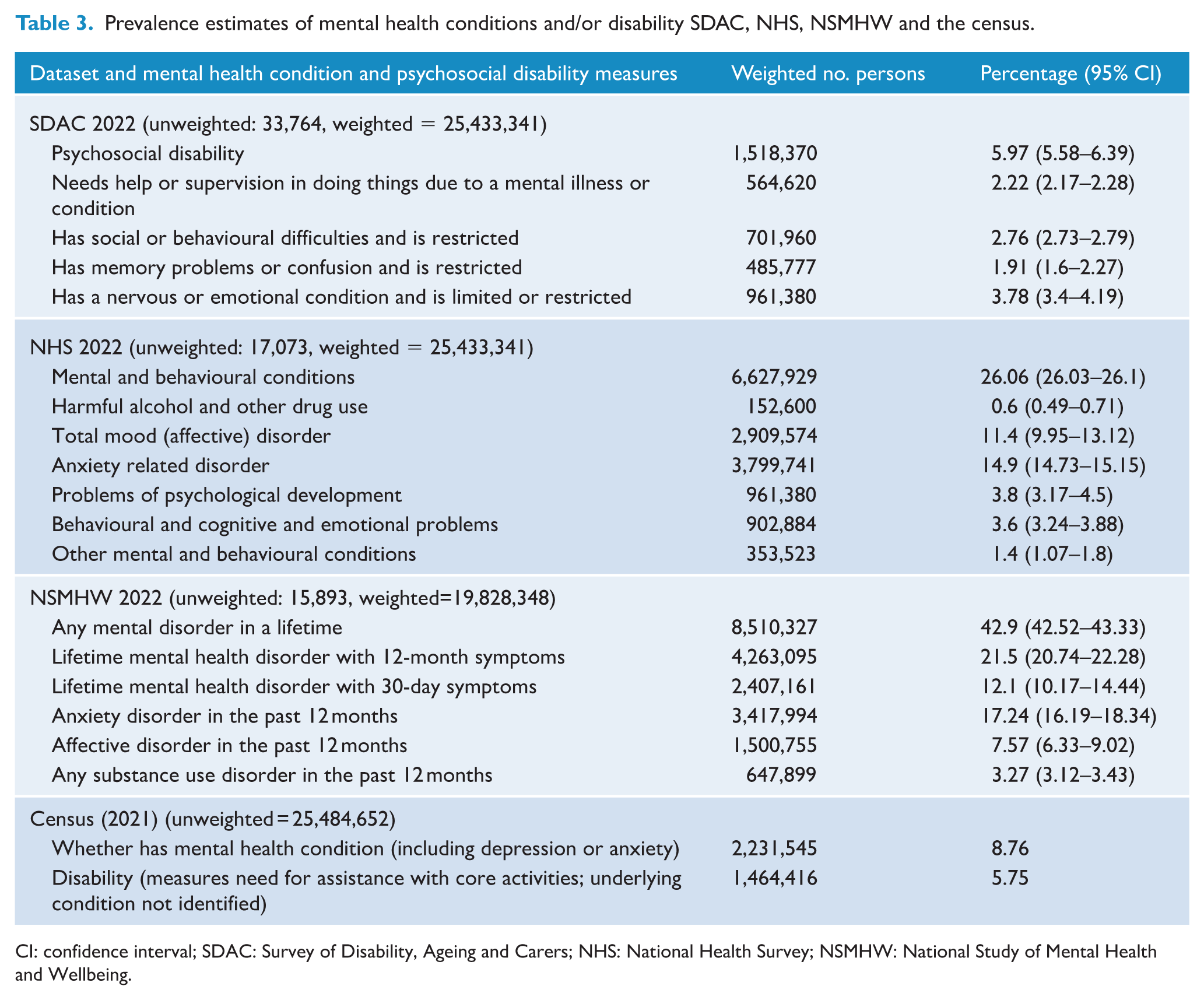
CI: confidence interval; SDAC: Survey of Disability, Ageing and Carers; NHS: National Health Survey; NSMHW: National Study of Mental Health and Wellbeing.
People with psychosocial disability experience one or more psychosocial impairments that limit or restrict their everyday activities. Among the 1.5 million people identified with psychosocial disability, the most commonly reported condition was a nervous or emotional condition that restricted daily functioning (63%) (Figure 1).
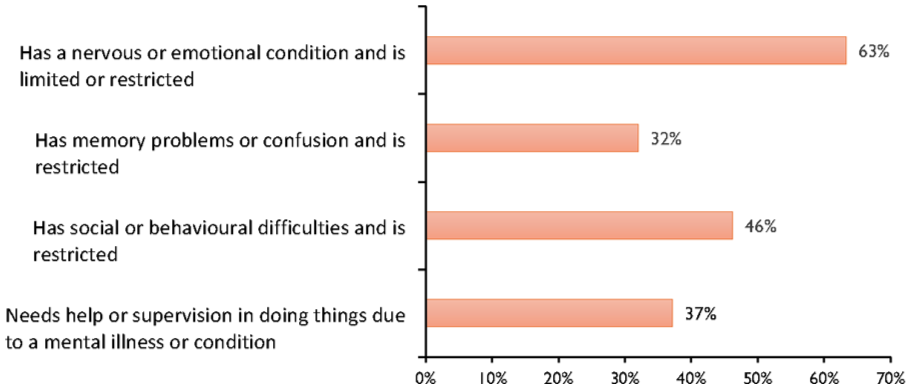
Conditions contributing to psychosocial disability.
Among people reporting a mental illness or condition requiring help or supervision, the most common causes were autism spectrum disorder (25.4%), depression (15.7%) and anxiety disorders (14.3%). Less frequent but notable causes included post-traumatic stress disorder (PTSD) (5.9%), schizophrenia (5.3%), dementia (5.2%), bipolar disorder (4.7%) and intellectual impairment (4.7%), with smaller proportions linked to attention-deficit/hyperactivity disorder (ADHD), Alzheimer’s disease, head injuries and other mental or behavioural problems. Other physical conditions also contributed (7.4%).
For those reporting a nervous or emotional condition restricting daily activities, depression (5%), anxiety (4.3%) and PTSD (4.3%) were most common. Among people with memory problems or confusion, head injuries (11.3%), dementia (10.4%) and stroke (10%) were leading causes. In cases of social or behavioural difficulties, autism spectrum disorder (24.1%) and anxiety (21.9%) were most frequent.
National Health Survey
Measurement approaches
The NHS collects information on long-term health conditions (table 2). Conditions are classified according to the International Classification of Diseases, 10th Revision (ICD-10). In the NHS, mental and behavioural conditions were defined as long-term conditions that have lasted, or are expected to last, 6 months or more (Supplementary File 3).
In terms of disability measurement, the NHS uses the ABS Short Disability Module, which adopts a functional, screening-based approach (Australian Bureau of Statistics, 2022b). The module identifies limitations or restrictions in everyday activities, allowing the survey to capture functional information without conducting a full disability survey. Its design makes it easy to embed within broader health surveys, but it is less reliable for estimating prevalence, particularly for milder forms of disability, and may tend to overestimate functional limitations compared with more comprehensive tools like the ICF used in the SDAC (Australian Bureau of Statistics, 2022b).
Prevalence estimates in NHS
The 2022 NHS included 17,073 participants, with population weights applied to produce national estimates. The overall prevalence of mental and behavioural conditions was estimated at 26.06% (95% CI: 26.03–26.10). Among these categories, the most commonly reported subgroups were anxiety-related disorders (14.9%, 95% CI: 14.73–15.15) and mood (affective) disorders (11.4%, 95% CI: 9.95–13.12). Smaller proportions were reported for problems of psychological development (3.8%, 95% CI: 3.17–4.5) and behavioural, cognitive and emotional problems (3.6%, 95% CI: 3.24–3.88). Other mental and behavioural disorders, including schizophrenia and other low-prevalence conditions, accounted for 1.4% (95% CI: 1.07–1.8), while harmful alcohol or other drug use affected around 152,600 people (0.6%, 95% CI: 0.49–0.71) (Table 3).
Among people with mental and behavioural conditions, 1,782,877 individuals (7.01%, 95% CI: 6.02–8.14) were identified as experiencing psychosocial disability. Severity of disability was measured across the six categories of limitations relating to core activities, as described earlier.
People with mental and behavioural conditions often experience psychosocial impairments that limit or restrict their everyday activities. Among the 6.6 million people identified with such conditions, anxiety-related disorders were the most commonly reported ones, accounting for 57% (Figure 2).
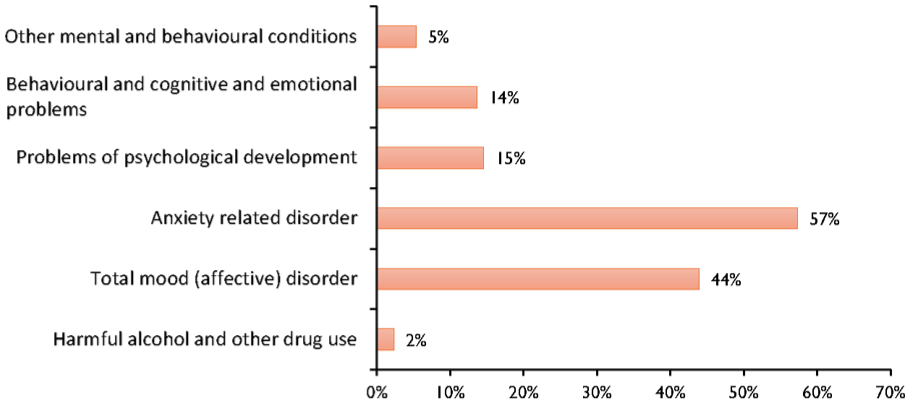
Proportion of conditions contributing to mental and behavioural conditions.
National Study of Mental Health and Wellbeing
Measurement approaches
The NSMHW captures information on the onset, recency and duration of mental health condition symptoms; examines their impact on key areas of daily life such as home management, work, relationships and social functioning and explores treatment-seeking behaviours, including access to and effectiveness of the care received. The survey used the Composite International Diagnostic Interview (CIDI 3.0) to assess a broad range of mental health conditions. These include high-prevalence, high-burden conditions: mood disorders such as major depression, dysthymia and bipolar disorder; anxiety disorders including generalised anxiety disorder, panic disorder, social phobia and PTSD; substance use disorders and eating disorders. However, the survey fails to capture lower-prevalence mental health conditions such as psychosis.
The NSMHW evaluates the level of impairment rather than measuring disability, focusing on how mental health conditions affect daily activities and role functioning. Functional impairment was assessed using the GAF score. In the survey, the predicted GAF score was calculated based on two components: the maximum number of days out of role and the scores from the Sheehan Disability Scale (SDS) domains. The SDS assessed the level of interference in four life domains during the worst period of symptoms in the 12 months prior to interview: home management, ability to work, ability to form and maintain close relationships and social life.
Prevalence estimates in NSMHW
In our analysis, an estimated 42.9% of Australians aged 16–85 years (95% CI: 42.52–43.33) reported experiencing a lifetime mental health disorder. Of those, 21.5% (95% CI: 20.74–22.28) reported symptoms within the past 12 months, while 12.1% (95% CI: 10.17–14.44) had experienced symptoms in the past 30 days (Table 3). The prevalence of mental disorder decreased with age across all time frames. The highest rates of both 30-day (24.3%) and 12-month (24.8%) symptoms were reported among those aged 16–24 years.
High rates of anxiety, mood and substance use disorders were reported. In the 12 months preceding the survey, the prevalence of anxiety disorders was 17.24% (95% CI: 16.19–18.34), with 24.9% classified as severe. The prevalence of mood (affective) disorders was 7.57% (95% CI: 6.33–9.02), with 45.1% being severe. For substance use disorders, the prevalence was 3.27% (95% CI: 3.12–3.43), and 24.2% were considered severe. Overall, 23.7% of individuals with any mental health disorder experienced severe symptoms.
Census of population and housing
The Australian Census screens the entire population for long-term health conditions by asking, ‘Has a doctor or nurse ever told you that you have any of these long-term health conditions?’ One response option is ‘Mental health condition (including depression or anxiety)’. Disability status and severity were defined by asking every respondent whether they required help from another person, or needed supervision, in three essential domains of daily living – self-care, mobility and communication – due to a long-term health condition, disability or old age lasting 6 months or more. The Census did not collect data on specific types of disability. The estimated prevalence of long-term mental health conditions in the population was 8.76% (95% CI: 8.75–8.77).
The NDIS
Measurement approaches
When assessing eligibility as an applicant with a primary psychosocial disability under the NDIS, key criteria related to diagnosis, functioning and permanence are considered. First, the disability must originate from a mental health condition. This includes conditions such as schizophrenia, bipolar disorder, severe depression, PTSD and other enduring mental health issues. Second, assessment considers the condition’s functional impact. The NDIS focuses on how the mental health condition reduces a person’s functional capacity in one or more key areas of life. These include communication, social interaction, learning, mobility, self-care and self-management. Third, except for a small number of people entering through an ‘early intervention’ pathway, a psychosocial disability must be considered permanent or likely to be permanent, even if symptoms fluctuate or vary in intensity. In this context, ‘permanent’ is understood to mean lifelong. Finally, there must be evidence of a need for ongoing support. This includes support required to carry out daily activities and to actively participate in the community and economy.
NDIS coverage
At the time of this analysis, there were 64,564 participants with psychosocial disability in the NDIS. Figure 3 shows variation in eligibility rates across psychosocial disability conditions, with schizophrenia having the highest eligibility (79%) and anxiety disorders the lowest (25%). Among NDIS participants, schizophrenia accounted for the largest proportion of conditions (56%), followed by bipolar affective disorder (10%) and major depressive illness (9%).
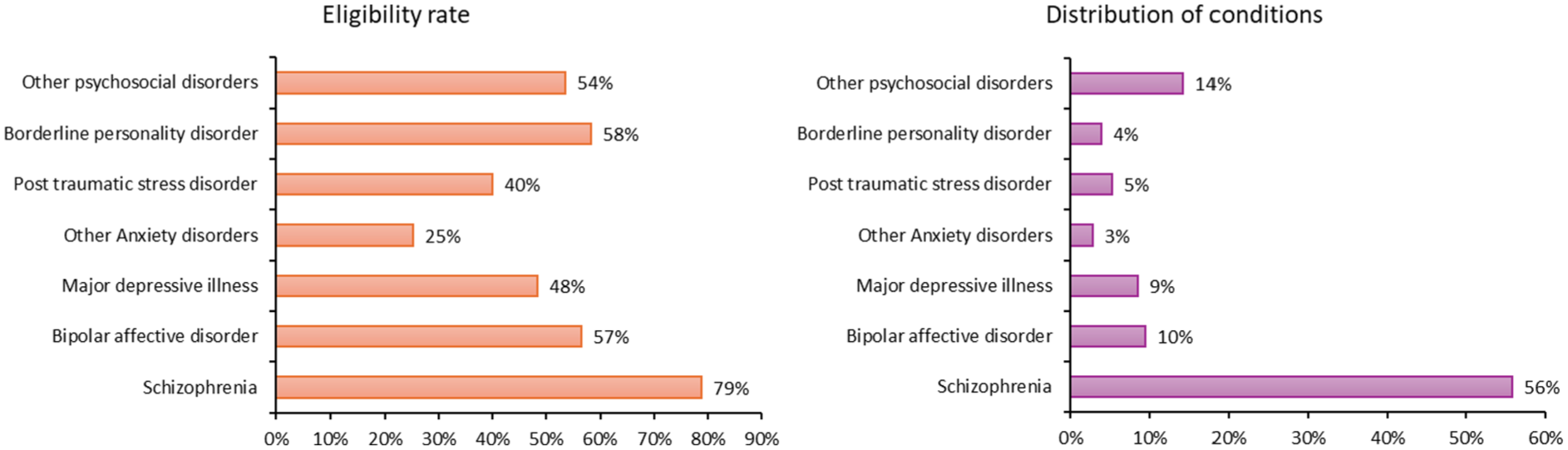
Eligibility for NDIS support and distribution of psychosocial disability conditions among participants by ICD classifications.
Discussion
There is an expectation that decisions about policy direction are based on evidence, and that policy is evaluated based on outcomes to the population in question (Davies, 2012). In Australia, mental health policy formulation is complicated by a lack of national data and well-documented inconsistencies in administrative data between states and territories (Grace et al., 2017). Recent analyses have further highlighted that Australia’s mental health information architecture is not fit for purpose, with substantial fragmentation and structural gaps limiting its ability to support coherent national planning (Rosenberg et al., 2022).
Our analysis highlights variations across existing national datasets, both in how mental health challenges and psychosocial disability are defined and in the nature of information collected. These definitional differences may contribute to shaping the visibility of particular population groups and, in turn, influence how need is understood and addressed (Saloniki et al., 2025). For example, the SDAC’s functional approach, which aligns with the ICF, captures a broader range of conditions – including neurodevelopmental and neurodegenerative disorders – than the diagnostic frameworks used in the NHS or NSMHW. In contrast, the NDIS focuses narrowly on enduring mental health conditions that meet service eligibility criteria. These findings show that the way psychosocial disability or severe mental illness is defined determines who is captured in the data. In practice, each dataset may represent a different segment of the population living with a mental health challenge.
Whiteford et al. (2017), in their estimation of mental health treatment rates, noted the necessity of assumptions being made within modelling of policy impact due to the incomplete nature of survey and administrative datasets. They further noted that differences in measurement, timing and wording between the NSMHW and the Survey of High Impact Psychosis (SHIP) complicate comparisons and service planning (Whiteford et al., 2017). Our findings show that such concerns remain. The inconsistencies we found highlight how definitional and measurement choices may drive differences in how the distribution of mental health challenges is perceived across population groups. In other words, the variations we see may reflect methodological differences rather than true differences in the underlying risk or prevalence. This also demonstrates the limits of using any single dataset to represent psychosocial disability nationally. Understanding these dynamics is essential for interpreting prevalence estimates and for designing data systems that more accurately reflect the complexity and diversity of mental health challenges in Australia.
We also note that comparisons across datasets must account for differences in how mental health conditions are identified. The Census and SDAC rely on self-reported long-term conditions and functional limitations without clinical verification, while the NHS captures self-reported conditions reported as diagnosed by a health professional. In contrast, the NSMHW derives diagnoses using structured diagnostic interviews, and the NDIS requires clinical documentation and evidence of substantial functional impairment for eligibility. These approaches measure related but distinct constructs, meaning prevalence estimates across sources are not directly comparable and largely reflect methodological differences in measurement. Consequently, ‘mental health conditions’ do not represent a single standardised construct across Australian data sources. In this study, the term encompasses dataset-specific operationalisations ranging from self-reported experiences of distress to formally diagnosed disorders with documented functional impairment. Clarifying this variation is essential for interpreting prevalence estimates and understanding what each dataset is designed to capture.
A further challenge relates to the inconsistent application of concepts and terminology related to psychosocial disability across national datasets. The SDAC and NHS adopt broader definitions that encompass a wide range of conditions – such as nervous or emotional problems, memory loss and behavioural difficulties – that may or may not be related to a diagnosed mental illness. In contrast, the NDIS uses a much narrower definition, limited to mental health conditions while explicitly excluding developmental and neurodegenerative disorders. These inconsistencies may also create a disconnect between how psychosocial disability is identified in population surveys and how it is operationalised in service systems such as the NDIS. As a result, the same individual could be classified as having a psychosocial disability in one dataset but not in another, making it difficult to compare estimates or align policy and service responses. This confusion arises in part because the introduction of the NDIS created a new category of ‘disability’ in order to encompass people with disability related to mental illness within the scheme (Carers Australia, 2011; Williams and Smith, 2014). Broader usage reflects an earlier definition focused on the disabling, psychosocial impacts of illnesses or conditions, such as physical illnesses, or social stigma (Labi et al., 1980).
There is also a question about whether current data-system terminology adequately captures the perspectives of people who have mental health challenges or are identified as having psychosocial disability. While our analysis highlights substantial variation in how datasets define and operationalise psychosocial disability, there is limited empirical research on how people with lived experience believe disability and mental health challenges should be identified and captured in national data systems. Qualitative studies suggest that consumers often emphasise the episodic, fluctuating and context-dependent nature of psychosocial disability and express concern that administrative definitions – particularly those linked to eligibility processes – can narrow or misrepresent their experiences (Choi et al., 2025). Future research should therefore prioritise co-designed approaches with people experiencing mental health challenges or identified as having psychosocial disability to develop data definitions and measurement frameworks that better reflect lived experience, including how functional impact, episodic and fluctuating nature and environmental barriers are understood and captured.
The variation in how psychosocial disability and mental health challenges are defined across data infrastructures has direct implications for policy and research. Streamlining these definitions is essential to ensure that national data sources reflect comparable populations and can be used coherently for planning and evaluation. It would be useful for each dataset to clearly indicate how psychosocial and mental health concepts are framed – e.g., distinguishing the broader functional framing in the SDAC and NHS from the narrower, eligibility-based definition used in the NDIS. These definitional inconsistencies are not unique to national datasets; recent ecosystem-based analyses similarly highlight the difficulty of establishing consistent and context-appropriate mental health definitions across complex service systems (Furst and Salvador-Carulla, 2024).
Current monitoring of the implementation of the Australian mental health policy often uses different datasets, even within the same evaluation, but without clarification of the different data that is collected within the surveys. For example, the 2021 Progress Report monitoring the Fifth National Mental Health and Suicide Prevention Plan uses both the NHS and the NSMHW at different points in the document without clarification. The National Mental Health Commission’s Annual Report Card (2024) also uses estimates from both the NHS and the NSMHW. However, that Report Card does provide a detailed, comparative explanation of the two datasets, including purpose, sampling, measurement and limitations.
Another important gap is the limited visibility of ‘low-prevalence’ but highly disabling mental conditions, such as schizophrenia, bipolar disorder and PTSD. These conditions are often combined into broad ‘mental and behavioural disorder’ categories in surveys, which dilutes the ability of policymakers to understand the population burden of these conditions and to plan appropriate service and resource allocation (Labi et al., 1980). This reflects the challenge of generating reliable estimates for comparatively rarer conditions in general-population surveys, where sample sizes are often insufficient for reliable measurement. While specialised epidemiological studies – such as the SHIP (Morgan et al., 2012) – can reliably capture low-prevalence disorders through targeted sampling, general-population surveys like SDAC, NHS and NSMHW are not designed for this purpose. As a result, low-prevalence disorders are difficult to map consistently across national datasets and are often underestimated in population data despite accounting for a large share of need for long-term, intensive supports – something captured more clearly in administrative datasets such as the NDIS.
For researchers and policymakers, our analysis highlights the importance of selecting data sources that are appropriate for the specific question or policy purpose. Each national dataset serves a distinct function and has inherent limitations that shape interpretation. Based on our analysis, the SDAC is most useful for understanding the functional impact of mental health challenges, patterns of support needs and the role of carers. It provides rich information for disability policy and planning, particularly in assessing unmet support needs. However, its broad definition of psychosocial disability – covering neurodevelopmental and neurodegenerative conditions – means it is not fully aligned with how the NDIS and support systems define or fund support for severe mental illnesses.
The NHS offers a wide view of the prevalence of mental and behavioural conditions and their relationship with physical health and health behaviours. It is well suited to monitoring national trends in mental health and general wellbeing, though its simplified disability measure limits its usefulness for analysing complex functional impairments. The NSMHW remains the most reliable source of diagnostic information, allowing detailed examination of disorder-specific prevalence, severity and service use. It is therefore particularly valuable for mental health service planning and prevention strategies. However, because it focuses on diagnosis rather than functioning, it does not explicitly capture psychosocial disability as a distinct construct and also lacks data on low-prevalence conditions, which have significant implications for planning and resource allocation. In addition, the survey is conducted infrequently, limiting its utility for monitoring trends over time, meaning that policymakers must rely on outdated diagnostic data when planning services or evaluating system performance. The Census, while containing only a single question on mental health conditions, provides complete population coverage and small-area detail. It is particularly valuable for mapping geographic patterns and linking mental health indicators with social and economic characteristics to inform local and regional service planning. Its simplicity, however, means it underestimates the complexity and severity of disability.
Conclusions
National data infrastructure differs in the way it captures data on mental health challenges, largely driven by its purpose. Variations in concepts and terminology also have direct consequences for how need is estimated, how services are planned and how resources are distributed across the health and disability sectors. With current demand for psychosocial supports continuing to outpace availability, an aligned and harmonised data landscape is critical for effective and equitable service planning and for accountability. Addressing definitional fragmentation will help identify who is affected, where needs are greatest and how systems can better respond to the realities of disabling mental health challenges.
Supplemental Material
sj-pdf-1-anp-10.1177_00048674261450886 – Supplemental material for Defining and measuring psychosocial disability in Australia: Assessment of national surveys and administrative datasets
Supplemental material, sj-pdf-1-anp-10.1177_00048674261450886 for Defining and measuring psychosocial disability in Australia: Assessment of national surveys and administrative datasets by Firew Tekle Bobo, Joel Hollier, Kuo-Yi Jade Chang, George Disney, Bernie Mullin and Jennifer Smith-Merry in Australian & New Zealand Journal of Psychiatry
Supplemental Material
sj-pdf-2-anp-10.1177_00048674261450886 – Supplemental material for Defining and measuring psychosocial disability in Australia: Assessment of national surveys and administrative datasets
Supplemental material, sj-pdf-2-anp-10.1177_00048674261450886 for Defining and measuring psychosocial disability in Australia: Assessment of national surveys and administrative datasets by Firew Tekle Bobo, Joel Hollier, Kuo-Yi Jade Chang, George Disney, Bernie Mullin and Jennifer Smith-Merry in Australian & New Zealand Journal of Psychiatry
Supplemental Material
sj-pdf-3-anp-10.1177_00048674261450886 – Supplemental material for Defining and measuring psychosocial disability in Australia: Assessment of national surveys and administrative datasets
Supplemental material, sj-pdf-3-anp-10.1177_00048674261450886 for Defining and measuring psychosocial disability in Australia: Assessment of national surveys and administrative datasets by Firew Tekle Bobo, Joel Hollier, Kuo-Yi Jade Chang, George Disney, Bernie Mullin and Jennifer Smith-Merry in Australian & New Zealand Journal of Psychiatry
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by an Australian Research Council Industry Laureate Fellowship (IL230100154) held by Professor Jennifer Smith-Merry (2024–2029). The National Disability Insurance Agency (NDIA) is a partner organisation on the grant but had no role in this study.
Author contributions
Data availability statement
The detailed microdata used in this study can be obtained by seeking approval from the Australian Bureau of Statistics.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.