
Abstract
The Australian and New Zealand Journal of Psychiatry GRADE Evidence Guidelines for Schizophrenia highlight the importance of considering psychiatric comorbidities, including autism spectrum disorder. These guidelines acknowledge that there is limited empirical research to guide the management of individuals with schizophrenia who also have these comorbid conditions. This lack of evidence poses challenges for clinicians, especially those working in early psychosis services, where the possibility of a missed diagnosis of autism spectrum disorder is increasingly being examined, and pre-existing diagnoses of autism spectrum disorder are not uncommon. This commentary explores the complex overlaps among shared histories, risk factors and symptomatology, as well as the difficulties stemming from the absence of validated assessment tools to aid in diagnostic clarification. Psychotic symptoms may complicate the recognition and differentiation of underlying neurodevelopmental characteristics of autism spectrum disorder. Considering the limited available evidence, practical guidance is offered to assist clinicians in their decision-making when a strong evidence base is lacking. In the context of early psychosis, diagnostic formulation should be considered provisional, with assessment of a possible a missed ASD diagnosis occurring after the stabilisation of psychotic symptoms wherever possible.
The ANZJP GRADE Evidence Guidelines for Schizophrenia acknowledge the importance of considering comorbidities, including autism spectrum disorder (ASD) (Suetani et al., 2026). These guidelines also emphasise that there is ‘. . . very little empirical research to guide us on the management of people with schizophrenia who have such comorbid conditions . . .’ (p. 30). This lack of evidence is problematic for clinicians, particularly those working in early psychosis services, where the question of a missed diagnosis of ASD is being increasingly considered (Treise et al., 2021), and a pre-existing diagnosis of ASD is not uncommon (Zheng et al., 2018). This commentary explores the complex overlap among shared history, risk factors and symptomatology, as well as the challenge posed by the lack of validated assessment tools to support diagnostic clarification. Based on limited available evidence, pragmatic guidance is provided to support clinician decision-making in the absence of a strong evidence base in the context of early psychosis.
ASD is a neurodevelopmental disorder where difficulties with social communication and restrictive/repetitive behaviours, interests or activities are evident from early childhood. In recent decades, there has been an increase in the proportion of people where the diagnosis is first made in youth and adulthood (i.e. ‘late diagnoses’) (Aggarwal and Angus, 2015; Carroll et al., 2025; Russell et al., 2025; Russell et al., 2022). This trend has coincided with increased public awareness of the disorder and the broadening of the diagnostic criteria following the shift from ‘autistic disorder’ in DSM-IV to ASD in DSM-5 (Harris, 2023; Murphy et al., 2016). Accompanying this broadening of the diagnostic boundaries is an increasing number of adults seeking assessment for ASD and a willingness for clinicians to assess adults for an ASD diagnosis (Carroll et al., 2025). It has been suggested that undiagnosed ASD is common in the general population and in those with mental illness (Fusar-Poli et al., 2020). However, diagnosing ASD in youth and adults is challenging, given the heterogeneous nature of the characteristics associated with this disorder (Carroll et al., 2025), and particular challenges arise in early psychosis services where ASD and psychosis have features in common (Russell et al., 2025; Treise et al., 2021).
Understanding the similarities and overlaps between ASD and psychosis
It is unsurprising that there is significant overlap between the phenotypes of ASD and psychotic disorders such as schizophrenia (see Figure 1) (Trevisan et al., 2020; Zheng et al., 2018). The term ‘autism’ formed one of the pillars of Bleuler’s conceptualisation of schizophrenia, based on the observations of a preoccupation with one’s ‘inner life’ and social withdrawal (Evans, 2013). The apparent overlap is most often observed in domains that resemble ‘negative symptoms’ of psychosis, reflected in the absence of typical social and communicative behaviours (Trevisan et al., 2020). Negative symptoms in schizophrenia are characterised by affective blunting (e.g. reduced affective sharing, eye contact, facial expressivity and gestural communication), alogia (impoverished speech output) and anhedonia (reduced motivation for social and recreational engagement) (APA, 2022). Similarly, ASD is defined by persistent deficits in social–emotional reciprocity, including reduced emotional sharing or initiation of social interaction, as well as impairments in nonverbal communicative behaviours (e.g. eye contact, gesture use and facial expression) and reduced spontaneity in communication and conversational reciprocity (Kincaid et al., 2017; Marder and Umbricht, 2023; Mosolov and Yaltonskaya, 2021).
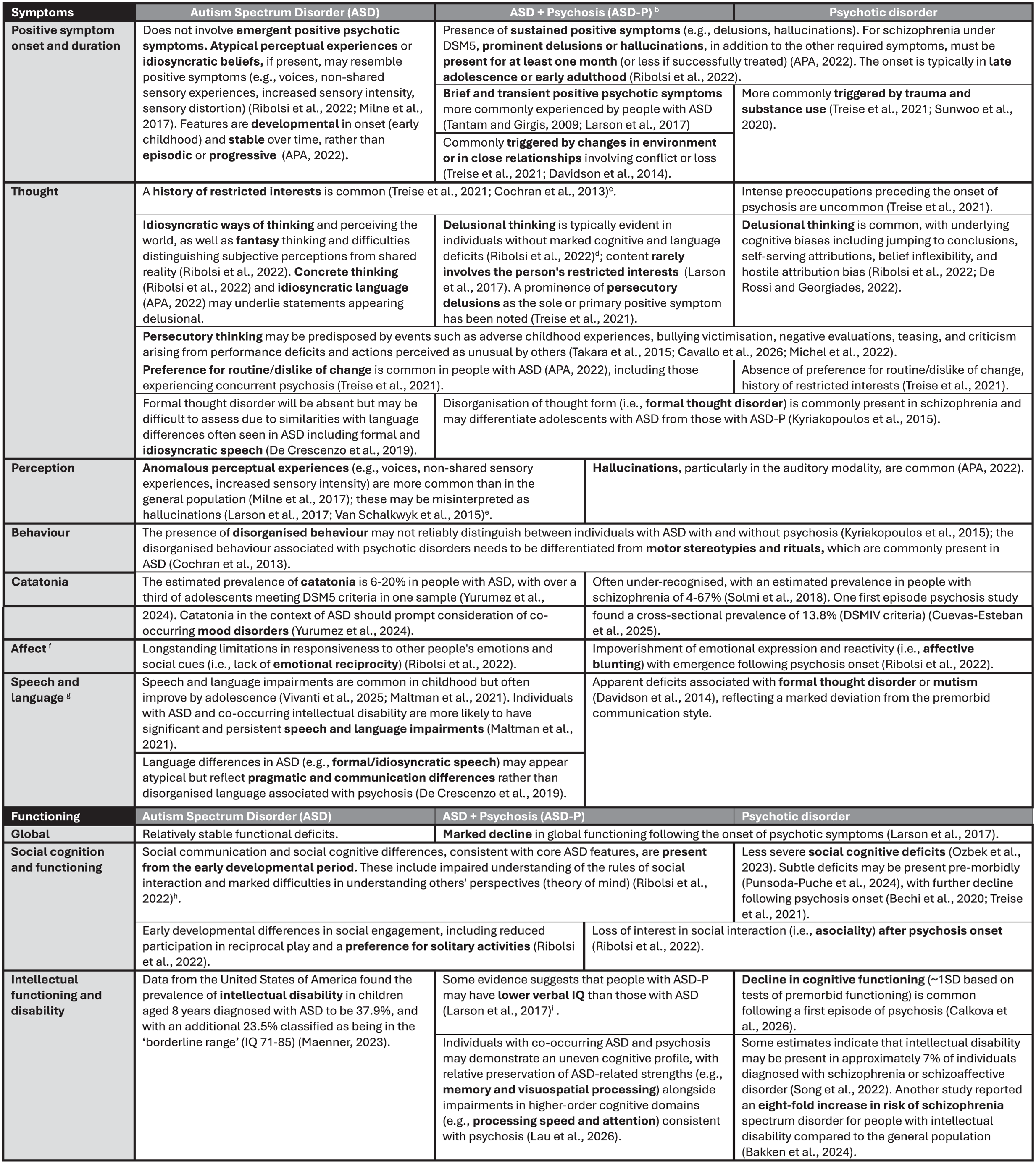
Matrix of heuristics guidance for differentiating of autism spectrum disorder (ASD), autism spectrum disorder and psychosis (ASD-P) and psychotic disorders based on the limited available evidencea.
In addition, several common features observed in ASD can mimic the ‘positive symptoms’ of psychotic disorders. Restricted interests, a rich fantasy life and concerns about persecution arising from recurrent negative evaluations by others, may resemble delusional thinking (Guerrera et al., 2024; Takara et al., 2015). Atypical perceptual and information processing in the auditory, visual and tactile domains may be misinterpreted as hallucinations (e.g. non-shared sensory experiences, increased sensory intensity, sensory distortion) (Milne et al., 2017). Furthermore, stereotypies and repetitive motor movements can resemble disorganised behaviour (Guerrera et al., 2024; Ribolsi et al., 2022).
The overlap in clinical features between ASD and schizophrenia may result from shared genetic and epidemiological risks (Cheung et al., 2010; Chisholm et al., 2015; Park et al., 2018) and neuroanatomical structural abnormalities (Diaz-Caneja et al., 2019). People diagnosed with ASD are at a greater risk of developing schizophrenia (odds ratio [OR] = 3.5, 95% confidence interval [CI] = [2.08, 6.05]) (Zheng et al., 2018), and rates of diagnosable ASD in people experiencing psychotic disorders are considerably higher than in the general population (Kincaid et al., 2017). The increasing recognition of the overlap between these conditions has contributed to conflicting concerns about ‘missed diagnoses’ and ‘misdiagnoses’ in people being supported for the first episode of psychosis (Bell et al., 2025; Treise et al., 2021; Zheng et al., 2018). Misattributing characteristics of ASD to a psychotic disorder risks iatrogenic harm (e.g. unnecessary exposure to antipsychotic medications), while misattributing psychotic symptoms to ASD (i.e. diagnostic overshadowing) delays appropriate care. Missing a comorbid diagnosis of ASD in a person experiencing psychosis reflects a missed opportunity to provide relevant scaffolding to support optimal functional outcomes (Fusar-Poli et al., 2022; Kentrou et al., 2024). However, a misdiagnosis of comorbid ASD in a person with schizophrenia can result in the provision of potentially inappropriate supports.
Overlapping and distinguishing characteristics of ASD, co-occurring ASD and psychosis (ASD-P), and primary psychotic disorders based on the limited available evidence are summarised in Figure 1. Taken together, these findings suggest that differentiation depends less on signs and symptoms observable in the current mental state examination, than on whether observed features represent continuity or discontinuity with prior functioning. In ASD, restricted interests and preoccupations, differences in social communication and atypical perceptual and information processing, by definition, reflect long-standing neurodevelopmental characteristics which are evident from childhood (APA, 2022). In primary psychotic disorders, delusions and hallucinations are sustained, represent new phenomena and are accompanied by a discernible shift in functioning (APA, 2022). In people who have ASD and later develop psychosis, a careful history along with detailed attention to phenomenology will enable identification in a change in an individual’s mental state and functioning from baseline with emergence of psychotic symptoms.
Screening and assessment for autistic and psychotic features
The differentiation described above highlights a central limitation of current assessment approaches. Validated screening and diagnostic tools for ASD and schizophrenia are designed to detect syndrome-specific symptom clusters rather than to determine whether observed features reflect pre-existing developmental characteristics or a change associated with emerging psychotic illness. Used in isolation, they cannot determine whether observed features reflect long-standing characteristics or recent change.
The Autism Diagnostic Observation Schedule (ADOS-2) and Autism Diagnostic Interview-Revised (ADI-R) are validated, commonly used tools for supporting the assessment and diagnosis of ASD in youth and adults in the general population (Frigaux et al., 2019; Mammarella et al., 2024). However, these tools have been found to have high false-positive rates in schizophrenia (Maddox, 2020; Nakamura et al., 2024). Similarly, tools like the Positive and Negative Syndrome Scale (PANSS) are well validated for assessing the presence and severity of symptoms in people experiencing psychotic disorders (Geck et al., 2025). However, these tools may have limited validity in assessment in the context of potential comorbidity (Zheng et al., 2018).
There has been increasing interest in screening for ASD in early psychosis populations (Treise et al., 2021) as well as for psychosis screening in children and adolescents diagnosed with ASD (Mammarella et al., 2024). This has coincided with efforts to develop tools for assessing autistic characteristics in the context of psychosis (Nibbio et al., 2022; Treise et al., 2021). However, given the engagement demands associated with structured diagnostic assessment tools for ASD, it is important to consider whether their use provides benefit in identifying people with ASD in the context of psychosis (Frigaux et al., 2019; Nibbio et al., 2022).
The PANSS Autism Severity Score (PAUSS) had been proposed as a brief measure derived from PANSS items and suggested as suitable for this purpose (Kastner et al., 2015). However, emerging evidence raises concerns about its validity, with findings indicating that PAUSS scores are more strongly associated with psychotic symptom severity than autistic traits (Chisholm et al., 2024; Pelizza et al., 2026; Zheng et al., 2021). Critically, studies have observed a lack of long-term stability in the PAUSS scores of people with first episode psychosis and established schizophrenia, suggesting it may reflect state-related features rather than underlying autism (Chisholm et al., 2024; Pelizza et al., 2026).
How should we be assessing for ASD in people with psychotic disorders?
There is a substantial risk of misdiagnosis when evaluating individuals for a potential ‘missed diagnosis’ of ASD in the context of the first episode of psychosis or an established psychotic disorder. Current evidence indicates that features resembling autism during acute psychosis may be transient and linked to the acute state (Pelizza et al., 2026). Furthermore, the persistence of these features is associated with the severity and treatment resistance of the psychotic disorder (Chisholm et al., 2019; Jeong et al., 2024). This complexity does not diminish the understanding of shared vulnerabilities and risk factors between ASD and psychosis; rather, it highlights the limitations of utilising present state and assessments conducted following the onset of psychosis as a basis for identifying a comorbid diagnosis of ASD.
ASD and other neurodevelopmental disorders (e.g. attention-deficit/hyperactivity disorder, specific learning disorders, intellectual disability) should be routinely considered in the assessment of an individual with psychosis. The absence of validated screening and diagnostic tools to assist in the identification of ASD in the context of psychosis poses a substantial challenge for clinicians. There is limited validation data supporting the use of measures such as the ADOS-2 and ADI-R in people diagnosed with psychotic disorders (Maddox, 2020; Trevisan et al., 2020). However, these standardised assessments are preferable to the PAUSS, for which there is growing evidence of a lack of validity in this context (Pelizza et al., 2026). Collateral information from caregivers to inform the developmental history, complemented by school reports and standardised assessments from childhood (if available) are informative for diagnosing ASD.
At present, there is no adequate substitute for a detailed developmental history, which includes screening for early features of ASD. The diagnostic value of the developmental history rests on the fact that features of ASD are, by definition, present from the early developmental period. Historically this was specified as before 36 months of age (DSM-IV-TR) (Wiggins et al., 2019); although no strict age cut-off is stipulated in DSM-5, it is acknowledged that features are typically evident within the first years of life (APA, 2022). As this precedes the prodrome of psychotic disorders by several years, documented continuity of social–communicative and restricted/repetitive features from early childhood provides evidence supporting ASD that is not confounded by emerging psychotic illness. For example, if a person consistently demonstrated age-appropriate social communication, flexibility, and imaginative and reciprocal play throughout early childhood, then ASD is unlikely. However, one of the challenges faced by clinicians in obtaining such a history in the context of concerns about a missed diagnosis of ASD beyond adolescence is the availability and reliability of collateral information about the early developmental years.
Where used, structured screening and diagnostic tools should be embedded within a comprehensive clinical assessment and interpreted in context, not as a diagnostic assessment in isolation. These tools complement a comprehensive assessment which includes current symptoms and developmental history, ideally provided by a parent or caregiver who has known the individual from childhood. These assessments should be deferred until the primary psychotic condition has been optimally managed (Treise et al., 2021), which may occur months or years after initial presentation. Determining a ‘missed diagnosis’ of ASD necessitates a focus on pre-morbid functioning and the developmental history, as corroborated by collateral sources (Ferrara et al., 2024). While standardised tools can assist in organising clinical observations, they should complement, rather than replace, longitudinal history-taking, multi-informant data and formulation-based clinical judgement. Guidance from subspecialist services (e.g. child/adolescent psychiatry and intellectual disability services) may be relevant to increasing confidence in the adequacy of the diagnostic assessment.
How should we be assessing for psychosis in people with autism?
People with ASD are at significantly higher risk of psychotic disorders than the general population (Davidson et al., 2014; Sunwoo et al., 2020). While there has been recent calls claiming ‘a priori screening of psychotic risk in neurodiverse populations is fundamental to prevent more serious conditions . . .’ (p. 16) (Mammarella et al., 2024), the implementation of such approaches is currently limited by the absence of validated screening tools for use in ASD populations. For screening to be appropriate, tools with strong validation data supporting its use in children, adolescents and adults diagnosed with ASD are needed.
The complexities of ASD mean that careful assessment is required when diagnosing a first episode of psychosis in this context. Common features of ASD can mimic positive psychotic symptoms, and the core features of ASD can overlap with, and at times resemble, some negative symptoms of psychosis. Individuals with ASD may demonstrate atypical perceptual experiences and idiosyncratic or unusual patterns of thinking, which can be misinterpreted as psychotic symptoms in some contexts (Takara et al., 2015). For example, atypical perceptual and information processing in the auditory, visual and tactile domains may be misinterpreted as perceptual disturbance (Milne et al., 2017). However, for a diagnosis of a psychotic disorder to be made, a comprehensive assessment to establish the presence of delusional thinking and/or hallucinations is needed, and where present, these symptoms must meet disorder-specific duration criteria (APA, 2022). Information from collateral sources will be important in establishing whether there has been a marked decline in functioning following the onset of psychotic symptoms, which is typical in psychotic disorders like schizophrenia. In undertaking these assessments, clinicians lacking familiarity with working with individuals with neurodevelopmental disorders should seek guidance from relevant subspecialist services.
Conclusion
The overlap between ASD and psychotic disorders presents a genuine diagnostic challenge, particularly in early intervention settings. Existing screening and diagnostic tools were not developed to resolve questions of comorbidity. Measures that quantify negative symptoms or autistic traits in isolation cannot establish whether observed features reflect long-standing characteristics or emerging psychotic illness. In the absence of validated instruments for comorbid presentations, structured tools should complement and be interpreted in the context of a comprehensive clinical and developmental assessment.
The risks of misclassification are substantial and bidirectional. Over-diagnosing psychosis in autistic individuals may result in unnecessary pharmacological treatment and reinforce stigma. Conversely, under-recognising psychosis in individuals with ASD may prolong the duration of untreated psychosis, delay access to evidence-based early intervention and contribute to poorer symptomatic and functional outcomes. Failing to identify co-occurring ASD in people with psychotic disorders may limit access to appropriate supports and adjustments. In presentations where autism and psychosis may be co-occurring, diagnostic certainty is rarely achievable in the acute phase. Symptoms may mask or mimic underlying neurodevelopmental characteristics. Diagnostic formulation should therefore remain provisional, and consideration of a missed ASD diagnosis should, where possible, follow stabilisation of psychotic symptoms.
Footnotes
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship and/or publication of this article: S.P. is supported by a Metro North Clinician Research Fellowship (2024-2027) and has received honoraria in the past 5 years from CSL Seqirus, Lundbeck/Otsuka, Johnson & Johnson, RANZCP, Queensland Psychotherapy Training, and Tasmania Health. The employers of JGS (University of Queensland and QIMR Berghofer Medical Research Institute) have received funds to support research from Janssen Cilag, Otsuka and Lundbeck in return for JGS delivering lectures at educational events and participating on advisory boards. S.S. was an author of the ANZJP GRADE Guidelines. All other authors have no additional conflicts of interest to declare. No specific funding was received for this project.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.