
Abstract
Background.
As adults age with human immunodeficiency virus (HIV), the role for rehabilitation continues to emerge. Understanding how social participation is affected among women aging with HIV can inform occupational therapy assessment and treatment.
Purpose.
Our purpose was to develop a theoretical model that describes the experiences of social participation from the perspective of older women living with HIV.
Method.
A grounded theory methodological approach was utilized. We conducted interviews with 20 women living with HIV, age 50 or older, to explore various aspects of social participation, including self-care, relationships with others, and access to health and social services. Emergent themes informed the theoretical model.
Findings.
The theoretical model comprises four concepts related to social participation: social engagement, social isolation, contrasting perceptions about factors variably influencing participation, and contextual influences that may enhance or hinder social participation.
Implications.
Women aging with HIV experience social participation as a dynamic process involving social engagement and isolation. Contextual influences may promote and impede social participation.
Description.
Compte tenu du vieillissement des adultes atteints du virus de l’immunodéficience humaine (VIH), le rôle de la réadaptation est en constante évolution. Une meilleure compréhension de la façon dont la participation sociale est affectée chez des femmes vieillissantes atteintes du VIH est susceptible d’éclairer l’évaluation et l’intervention en ergothérapie.
But.
Notre but était d’élaborer un modèle théorique pour décrire les expériences de participation sociale vécues par des femmes âgées atteintes du VIH.
Méthodologie.
Une méthode de recherche fondée sur la théorie ancrée sur les données empiriques a été utilisée. Nous avons réalisé des entrevues auprès de 20 femmes âgées de 50 ans et plus qui sont atteintes du VIH, afin d’explorer différents aspects de la participation sociale, dont les soins personnels, les relations avec les autres et l’accès aux services sociaux et de santé. Des thèmes émergents ont éclairé le modèle théorique.
Résultats.
Le modèle théorique comprend quatre concepts associés à la participation sociale, soient: l’engagement social, l’isolement social, les perceptions contrastées face aux facteurs variables qui influencent la participation et les influences contextuelles qui peuvent favoriser ou faire obstacle à la participation sociale.
Conséquences.
Chez les femmes qui vieillissent avec le VIH, la participation sociale est vécue comme un processus dynamique mettant en jeu l’engagement social et la participation sociale. Les influences contextuelles peuvent favoriser ou faire obstacle à la participation sociale.
Keywords
The availability of combination anti-retroviral therapy (cART) has increased survival in people with human immunodeficiency virus (HIV) and transformed HIV from a terminal illness to a manageable and chronic condition (Grabar, Weiss, & Costagliola, 2006). According to the Centre for Communicable Diseases and Infection Control, Public Health Agency of Canada (CCDIC, PHAC, 2010, chap. 5), adults 50 years of age and older living with HIV are considered older adults. Adults 50 or older compose an increasing proportion of both incident and prevalent cases of HIV; the proportion of HIV-positive test reports among older adults rose from 10.6% in 1999 to 15.3% in 2008 (Bhavan, Kampalath, & Overton, 2008; CCDIC, PHAC, 2010, chap. 5).
The consequences of the physical, cognitive, and psychological manifestations of aging with HIV continue to emerge. Existing literature has largely focused on understanding the co-morbidities associated with aging and the interaction between HIV infection and the immune system as one ages. The persistent immune dysfunction and chronic inflammatory state evident in people with HIV can lead to “accelerated aging,” even among people with excellent virologic control with cART (Patel & Crane, 2011). This accelerated aging can manifest as cardiovascular disease, cancer, frailty, immune dysfunction, and organ damage. These conditions can emerge at earlier ages in people with HIV compared with the general aging population (Deeks, 2011).
In addition to the well-documented physical sequelae of HIV infection and its treatment (e.g., Carr & Cooper, 2000; Lee et al., 2009), people with HIV often face challenges related to their social participation. Social participation is an indicator of well-being that refers to one’s involvement in social activities, such as volunteering, recreation, work, and cultural practices (Human Resources and Skills Development Canada [HRSDC], 2012). Factors that influence social participation include the presence of social networks, a sense of belonging, and trusting relationships (HRSDC, 2012). Social isolation is one factor associated with social participation that is well documented in older adults with HIV (Bhavan et al., 2008; Emlet, 2006b; McDowell & Serovich, 2007; Shippy & Karpiak, 2005a; Simoni, Montoya, Huang, & Goodry, 2005). Older HIV-positive adults are more likely to be socially isolated than younger people with HIV (Emlet, 2006a; Siegel, Raveis, & Karus, 1998).
Social isolation may be partially attributed to stigma, which may stem from both HIV-positive status and age (Shippy & Karpiak, 2005a). Older adults with HIV experience increased HIV-related stigma and loneliness compared to other HIV-positive populations (Grov, Golub, Parsons, Brennan, & Karpiak, 2010). Schrimshaw and Seigal (2003) interviewed 45 men and 18 women over the age of 50 with HIV regarding their perceived barriers to social support. Ageism emerged as a major theme; participants believed that older adults were viewed with less sympathy and support than their younger counterparts. Participants were less willing to ask for support as they valued their independence and did not want to be a burden to others. In a survey, Grov and colleagues (2010) found that 39% of older adults with HIV exhibited symptoms of major depression, which was significantly related to HIV-associated stigma, loneliness, decreased cognitive functioning, and reduced energy (n = 914). Aging may add additional social and psychological challenges to the lives of individuals living with HIV. Older adults with HIV can feel unwelcome in programs offered through AIDS service organizations (ASOs), given their focus on supporting younger populations (Shippy & Karpiak, 2005b). Psychological symptoms in older adults with HIV have been correlated with decreased support from friends and reduced access to health and social services (Heckman et al., 2002).
Alternatively, some older adults with HIV fare well, and in some cases, better than younger adults with HIV. Aging can be accompanied by wisdom, patience, contentment, moderation, and a greater respect for health and life. These traits may enable older adults to cope well with their illness (Siegel et al., 1998). Aging with HIV may foster resilience, self-acceptance, and optimism (Emlet, Tozay, & Raveis, 2011). Older adults with HIV have also reported fewer depressive symptoms (Mavandadi, Zanjani, Ten Have, & Oslin, 2009; Sherr et al., 2009), greater positive affect (Mavandadi et al., 2009), and greater vigour (Sherr et al., 2009) than younger people with HIV, which may be linked to greater perceived satisfaction with social support (Sherr et al., 2009).
Gender differences in social participation are emerging in older adults living with HIV. As women 50 or older now account for 15.1% of positive HIV test reports among older adults in Canada (CCDIC, PHAC, 2010, chap. 6), it is important to understand their unique experiences. Goodkin et al. (2003) found gender differences in the sources of life stressors in older HIV-positive adults. Men’s concerns tended to be more body focused (e.g., worried about changes in physical appearance), whereas women’s concerns were more relationship focused (e.g., worried about their children). Because women are socialized to care for their families, HIV-related symptoms may reduce their ability to care for their homes, care for their children, or engage fully in their own self-care (Hudson, Kirksey, & Holzemer, 2004). A recent meta-analysis found that among women with HIV, social isolation is tied to adverse mental health outcomes (McIntosh & Rosselli, 2012). A phenomenological study examining participation among women living with HIV found that living in poverty, enduring depression and isolation, and fearing disclosure and stigma contributed to women’s social isolation. However, having children to support, balancing life with HIV, and accessing support networks appeared to enhance social participation (Solomon & Wilkins, 2008). These studies did not focus specifically on older women. Emlet, Tangenberg, and Siverson (2002) revealed that older women feel a sense of isolation, underscoring the supportive environments for this population. With increased longevity, there exists a need to understand the unique consequences of aging with HIV from a gender perspective.
Occupational therapy has a role in addressing the physical, cognitive, and psychological manifestations of HIV and specifically, challenges to social participation among older women living with HIV (Barkey, Watanabe, Solomon, & Wilkins, 2009; Solomon & Wilkins, 2008). The International Classification of Functioning Disability and Health (ICF; World Health Organization [WHO], 2001) has been used to inform rehabilitation approaches to assessment and treatment in the context of HIV (Nixon & Cott, 2000; Pettersson, Pettersson, & Frisk, 2012); however, no known theoretical models exist to specifically inform occupational therapy practice to enhance social participation in older women with HIV.
The purpose of this research was to develop a theoretical model of social participation in older women living with HIV “grounded” in theoretical analysis (Charmaz, 2006). This model will help to inform future occupational therapy practice with the aim to enhance social participation among older adults with HIV.
Method
We conducted a grounded theory study to examine social participation from the perspective of older women with HIV. Constructivist grounded theory (Charmaz, 2006) provided us with the ways in which to consider meanings, processes, and contexts of social participation among older women with HIV while understanding knowledge as socially constructed. This approach acknowledges the multiple perspectives of the women aging with HIV and of ourselves as researchers and reflexively considers our positions and privileges as researchers relative to our participants (Charmaz, 2009, pp. 129–130). We completed a literature review to place our research in the context of a greater body of knowledge rather than to guide the development of our theory. Ethical approval for the study was obtained from the University Research Ethics Board.
Participants
We used maximum variation sampling in which we recruited participants with variable characteristics to be able to document differences across the aging experience (e.g., ethnicity, employment status, time since diagnosis). We recruited women by posting advertisements and brochures on websites and in waiting rooms at HIV clinics and ASOs. We received written consent from all participants prior to initiating the interviews. To be eligible for the study, women had to be HIV positive, 50 years or older, and able to communicate orally in English. Our definition of older adult as 50 or older is consistent with the current definition used by the CCDIC of the PHAC (2010, chap. 5).
Data Collection
We conducted semi-structured face-to-face or telephone interviews with older women living with HIV. Face-to-face interviews occurred at locations chosen by participants, including ASOs, coffee shops, and libraries. All of the participants lived in southern Ontario with the exception of one woman who lived in Nova Scotia. We asked participants about various aspects of their social participation, including self-care and household management; relationships with family, friends, and romantic partners; work; and access to health care and social support services. Examples of interview questions were “Describe the challenges that you experience with living your everyday life and interacting with others as you age with HIV,” “Have you ever accessed specific services and supports for older adults with HIV?” and “What types of things in your day-to-day surroundings affect your challenges aging with HIV?” Interview questions were modified as part of our constant comparative method (Charmaz, 2006) as we collected and analyzed interview transcripts throughout the study. Interviews ranged in length from 15 to 90 min. The interviews were audio recorded and transcribed verbatim. Participants received a small honorarium.
Data Analysis and Rigour
The data were analyzed using a constructivist grounded theory approach (Charmaz, 2006). NVivo 8 software (Version 8) was used to manage and organize the data. We began by noting our pre-conceptions before reading any transcripts. Our pre-conceptions included that HIV-positive status penetrates all areas of life and dictates personal choice and engagement; HIV-positive status is accompanied by feelings of shame, guilt, and loss; and individuals with HIV have little hope for the future. The first and second author then read all transcribed interviews to obtain an overall sense of the content and meaning of the participants’ experiences. Three transcripts were then independently coded by the same two authors using Charmaz’s (2006) analysis strategies. During this initial coding, we remained open to emergent ideas expressed by participants. We subsequently met to establish a coding scheme that was grounded in the data, after which the remaining transcripts were coded independently. Thirty-four initial codes emerged; these initial codes were then reviewed to reduce the data through focused coding into categories. During this stage, we compared actions, experiences, and interpretations between and across participants as part of constant comparison methods (Charmaz, 2006). We wrote memos throughout the analysis to facilitate ongoing comparison of codes, categories, and emergent concepts and to appreciate the connections among these elements. The comparison allowed us to realize that there was a range of responses to social participation that could be represented in contrasting concepts of social engagement and social isolation that subsumed the categories. The concepts, in turn, informed the development of a theoretical model that outlined processes related to social participation for older women living with HIV (Figure 1).
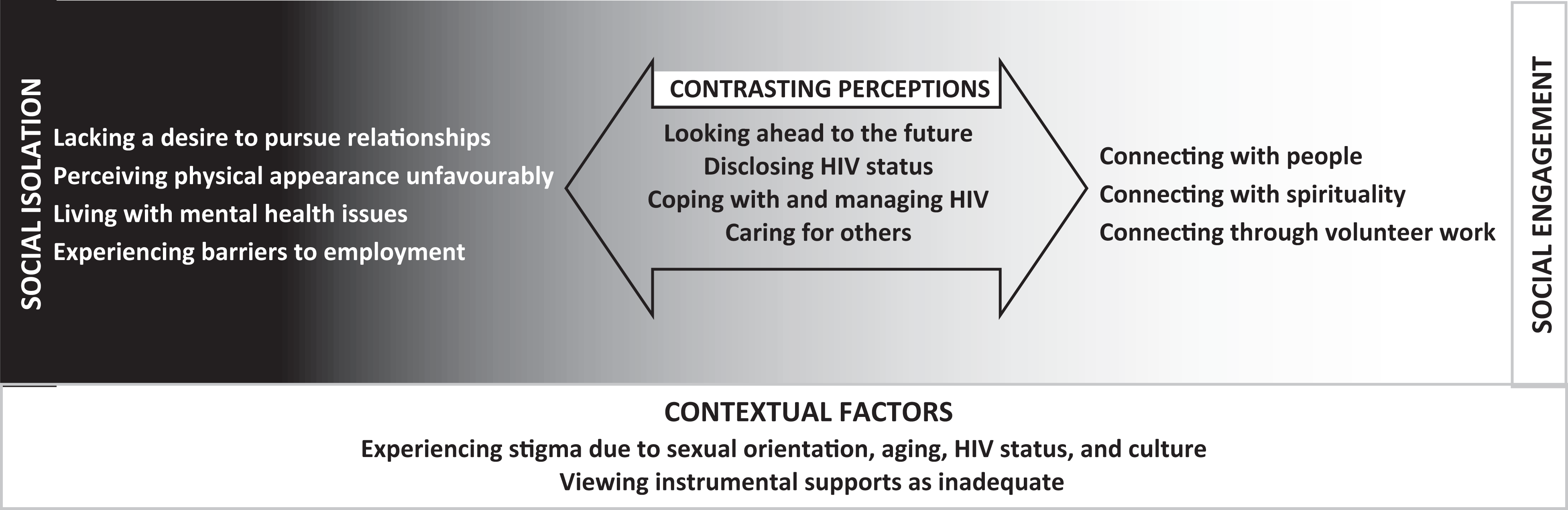
This figure presents a model of social participation in older women living with HIV. Social participation exists as a continuum with social isolation at one end and social engagement at the other, and contrasting perceptions having the potential to fall to either side. Factors described by the women associated with social isolation are listed to the left of the model. Factors experienced positively by the women composing the theme of social engagement are listed to the right. Contrasting perceptions describe elements of social participation associated with social engagement by some women and with social isolation by others. Contextual factors depict the parts of the environment that form the context that may influence the entire spectrum of social participation.
Rigour was ensured through a decision trail used to track the development of codes, categories, and concepts. Research team meetings provided an opportunity for peer discussions among novice and experienced team members.
Findings
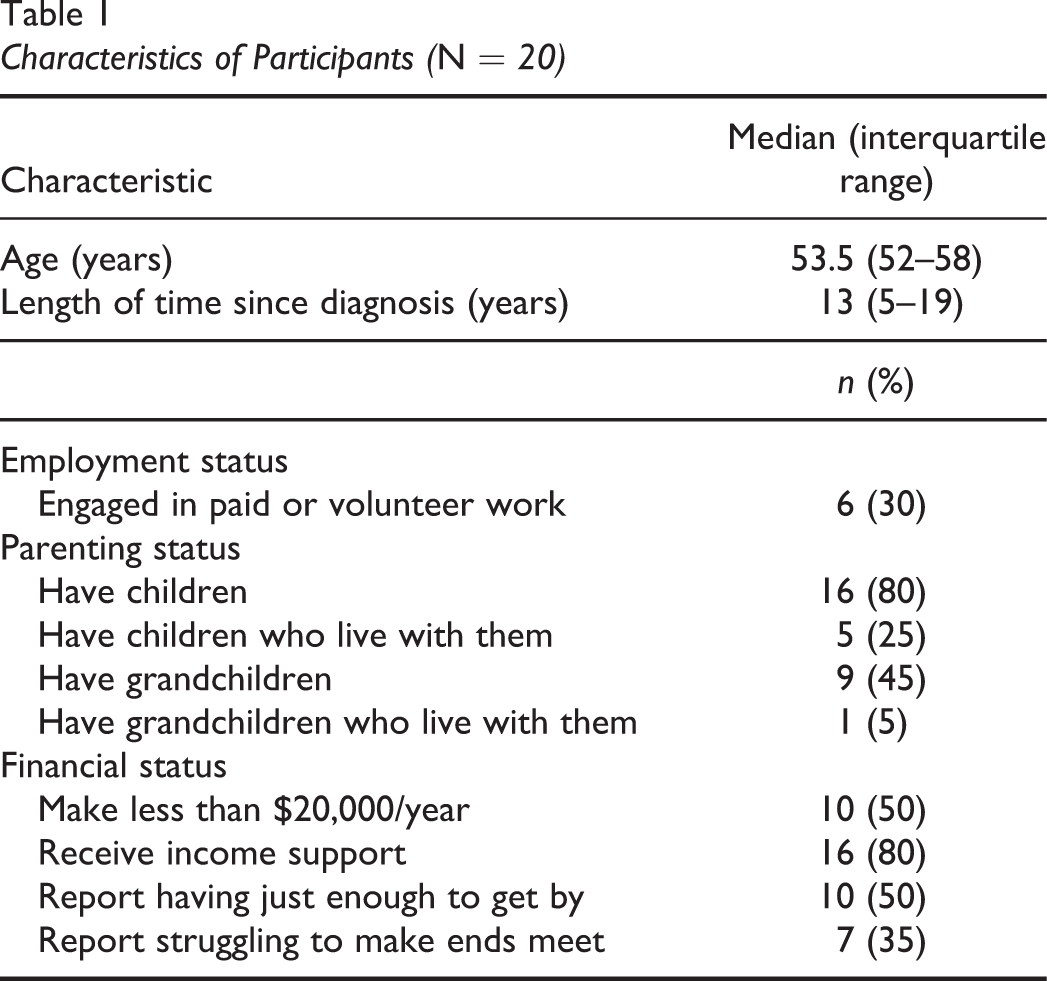
Twenty older women with HIV (19 born female, 1 male-to-female transgendered) participated in the interviews between December 2009 and June 2011 (see Table 1).
Characteristics of Participants (N = 20)
The theoretical model of social participation of older women living with HIV comprises four overarching concepts that emerged from the data and describe social processes that are related to social participation: social engagement, social isolation, contrasting perceptions about aspects that variably influence participation, and contextual influences that may affect social participation. Each concept comprises a series of categories that represent the processes that influence social participation for older women living with HIV. Categories of social participation that composed the concept of social engagement were connecting with people, with spirituality, and through volunteer work. Aspects of social participation that were experienced negatively by older women with HIV represented social isolation; its categories were lacking a desire to pursue relationships, perceiving physical appearance unfavourably, living with mental health issues, and experiencing barriers to employment. The concept of contrasting perceptions comprised categories of social participation that were framed positively by some women but unfavourably by others: looking ahead to the future, disclosing HIV status, coping with and managing HIV, and caring for others. Contextual influences emerged as parts of the environment that affected participants’ social participation and comprised categories of experiencing stigma related to sexual orientation, aging, HIV status, and culture, and viewing instrumental supports as inadequate. The concepts and their categories are described below with representative quotations. This model depicts how social participation varies on a continuum from social isolation to social engagement and how women report contrasting perceptions that variably influence their participation.
Social Engagement
This concept focused on the positive aspects of social participation and highlights the importance of making connections with others by connecting with people, with spirituality, and through volunteer work.
Connecting with people
Participants emphasized the importance of support from friends and family members. Loved ones provided emotional support and comfort as well as practical assistance, such as health care advice and help purchasing items. “I have this sort of little inner sanctum of good people that I trust. And I would ask them…if I had something that I required their help with.” Meaningful connections with friends and family members brought a sense of closeness and joy. Technology was a facilitator of connecting with others. Some used e-mail and Facebook to stay in touch with family members and friends and to access information about social events.
Connecting with spirituality
Having spiritual or faith-based connections was perceived to be an enabler of social engagement that helped older women with HIV cope with the challenges in their lives. Participants identified gaining strength, coping strategies, and spiritual connection from worship at churches and other spiritual institutions: “I feel [church is] where I have gotten a lot of my emotional strength to cope with the family and…to make peace with myself.” This connection with spirituality was more of an individual one between each woman and her spiritual beliefs than a collective one shared with others. This connection was nonetheless highly valued by some participants.
Connecting through volunteer work
Participants discussed how, through their volunteer work, they related to others with similar experiences and felt personally fulfilled. Women also discussed the reciprocal nature of volunteer work and the benefits that they received while helping others: “I think [peer case management] strengthens me because I’m able to share with…others, and others share with me their experiences.” Volunteering provided a meaningful and enjoyable activity for older women with HIV who were not engaged in paid employment and enabled them to contribute to their communities.
Social Isolation
This concept encompassed women’s descriptions of situations that accompanied decreased engagement with others and their community. Categories illustrated concerns regarding relationships, physical appearance, mental health, and employment.
Lacking a desire to pursue relationships
Some participants expressed that it was easier to be alone because they did not have the desire or energy to engage socially with others. Social withdrawal or isolation was often attributed to aging, having HIV, or both. Women also described how their reluctance to engage socially influenced their engagement in valued occupations: “I don’t really think I have the energy to play…the social game as well as I did when I was younger. So I avoid doing things that I would love to do.” While some women seemed to accept social isolation, others wished they had more social connections, and others felt ambivalent about their situation.
Perceiving physical appearance unfavourably
Women expressed unhappiness with their physical appearance and described how this affected their self-concept. One participant clearly described how her perception of her appearance was a barrier to her social participation: “I didn’t want to go out; I didn’t want to associate with anyone. I didn’t want to go to a family dinner because my face was so haggard.” Some women were concerned about how they may be regarded by others because of their physical appearance, which had been affected by the accelerated aging process associated with HIV.
Living with mental health issues
Some women spoke of living with mental health issues and of feeling marginalized by society: “I think living with HIV and aging with it, I think it could make older people feel very unloved…which can lead to depression and sadness in your life.” Living with mental health challenges added a further layer to the women’s perceived stigma, in addition to feeling discriminated against due to age and HIV status.
Experiencing barriers to employment
Many of the women described how their HIV-positive status and older age negatively affected their participation in work. Some described how the structure of provincial financial support systems for people with disabilities created a disincentive to work: “The jobs that you can get, you can make as much on disability [support funding] so it’s gonna cost you to go to work.” The relationship between work and one’s sense of meaning and purpose was emphasized by some women: “I probably never feel good about myself until I work. Everybody has to work, you know.” Receiving disability supports seemed to be a frustrating reality for many women who expressed longing for more typical aspects of getting older, such as enjoying stable work or retirement.
Contrasting Perceptions
Contrasting perceptions comprised several categories associated with social participation that the women experienced differently. Some women’s experiences with social participation were associated with social engagement, while others were connected to social isolation. Categories highlighted looking ahead to the future, disclosing HIV status, coping with and managing HIV, and caring for others.
Looking ahead to the future
Some of the women described feeling hopeful about the future, while others expressed that they felt “stuck” and lived day by day. Women looking forward to the future spoke of the positive aspects of aging, such as growing old with their families and being involved in the lives of their children and grandchildren. They looked forward to retirement and travel. One participant portrayed a sense of determination and resilience: “I don’t plan on having any disease beat me. I want to beat the disease. I wanna die of something natural like old age.” Conversely, other women spoke negatively of the future with regard to their deteriorating health and feelings of burdening others: “I don’t think I’m looking forward to anything. Yeah, because what does it mean? It means I can’t walk anymore, I cannot work anymore. No, I don’t look forward to that.” Some expressed a general uncertainty and apprehension for the future; they had few concrete plans and lived one day at a time: “To look into the future is kinda scary for me…what do I have to look forward to now? What is it that I want to do?” Others expressed uncertainty regarding their capacity to accomplish goals, and described how HIV was a constant consideration in their life:
Whatever I want to do…it’s still there that I’m living with HIV. So, whatever I want to accomplish it’s like, can I accomplish this? I have to still think of that. So, [HIV] is always number one whatever I do.
Disclosing HIV status
Some women described being very deliberate about when, how, and to whom they disclosed their HIV status:
In my life there are two groups of people. There are people that are aware of my status…so I discuss stuff with them and they’re usually long-term friends. Then there are people that don’t know my status and I don’t discuss anything about HIV with them.
Coping with and managing HIV
Some women indicated that they felt well in spite of their health challenges: “The aging with HIV at this point is pretty good compared to everything else. You know…it’s not bothering me at all.” Health challenges affected participation, but they chose to accept their limitations and be “kinder” to themselves:
I try to live my life to make it as good as it can be and deal with…the tiredness and the lethargy and things like that, so I have to balance. So I sometimes have to make decisions to not do some things that I’d like to do.
Caring for others
Some women specifically expressed how they perceived that the caregiving role in their families affected their lives differently than those of men living with HIV without children. In a positive sense, having children gave women more reasons to keep themselves healthy and gave hope and meaning to the future. Others indicated that having children complicates living with HIV in terms of having others to care for beyond themselves:
I think women have too many things to worry about, especially if we are women and a mother at the same time. You are always not first…in many things, you know? You put someone first if you have a child like me, so you’re mom, you put the child first.
Contextual Influences
Contextual influences consisted of components of the environment that shaped the continuum of social participation. The first contextual influence, stigma, was multifaceted and related to gender and sexual orientation, aging, HIV status, and culture. The second contextual influence was instrumental supports, which some participants viewed as inadequate and hindering their social participation.
Experiencing stigma due to gender and sexual orientation
The assumption that HIV mainly affects men limited women’s ability to obtain support and access services: “There isn’t much support for women. Aging or not aging. There’s not a lot for women. Not as much as for the guys.” Some participants also reported stigma in relation to sexual orientation, which was evident in the belief that HIV affects gay men: “You sit there and it feels like it’s just…a gay disease, but it’s not.” Prevailing beliefs that HIV primarily affects gay men meant that they were not “in with the in crowd,” and felt alienated from resources intended to serve people with HIV.
Experiencing stigma due to aging
Participants also experienced age-related stigma. “I don’t look like an HIV-positive person, you know, I’m too old, too grey, whatever. I don’t fit into anybody’s idea of what [an HIV-positive person] is.” One woman described how her older age did not fit with societal expectations regarding the typical profile of someone with HIV: “A lot of people think that just a certain type of person, just young people or just Brand X people or this type of people get HIV. Well, it’s not true. Every, anyone can get HIV.” This stigma was evident not only in societal beliefs but also in the groups to which HIV/AIDS-specific services were tailored. Specifically, few services were available for older women aging with HIV: “My challenge to you is to say, what supports are there for older adults living with HIV? Because I don’t think there are that many of them.”
Experiencing stigma due to HIV status
Many women described being the target of stigmatizing, discriminatory actions that they attributed to their HIV-positive status. The source of this discrimination was sometimes health care providers:
I was coming out of the room into the waiting area and it was full of people and everything else and [the dentist] bluntly told me that the only way he would work on me is if I was the last patient of the day because of my HIV.
Experiencing stigma due to culture
A few of the women described being the target of stigma or discrimination based on their cultural background or a location in which they had previously lived: “As soon as they [health care providers] found out that I had been living in Africa they treated me like a leper…they just…treated me differently because of my life experience.” This category was brought forth only by a small number of participants. Some of the women experienced stigma while living in Canada, while others felt it while living in other countries.
Viewing instrumental supports as inadequate
Many women indicated that their social participation was limited by the inability of instrumental supports, such as government-run housing subsidies and income support programs, to meet their needs. Regarding her housing, one woman said, “I hate where I’m staying, it’s not…the kind of place I’d like to live in. It’s dirty, it’s got elevators that don’t work. The only area where I’m feeling totally discriminated against is housing.” Others felt dissatisfied with government-administered disability support programs, namely, the Ontario Disability Support Program (ODSP). “I hate the way…you get treated by ODSP…in the very inconsiderate way funds are given out.” The process of obtaining financial support could be laborious: “We have to fight. And we fight and we fight and we fight to get [support payments].” Limited financial resources restricted some women’s ability to be mobile in the community, access programs and services, participate in leisure activities, and maintain a sense of freedom.
Discussion
The findings from this study present a model of social participation for older women living with HIV that describes the elements associated with social engagement and social isolation. Previous research examined social participation and isolation in people with HIV (Bhavan et al., 2008; Shippy & Karpiak, 2005a), aging with HIV (Emlet et al., 2011; Heckman et al., 2002; Siegel et al., 1998), and experiences of women with HIV (Hudson et al., 2004; McIntosh & Rosselli, 2012; Solomon & Wilkins, 2008). This is the first study to develop a model that encompasses all of these elements to illustrate social participation among older women living with HIV.
Our theoretical model is novel in that it conveys how social participation varies on a continuum from social isolation to social engagement and how women report contrasting perceptions that variably influence their participation. Similar to the ICF (WHO, 2001), this model highlights the important role of environmental factors in influencing health and participation. This facet of the model correlates with previous research highlighting the relationship between the social environment—including the presence of stigma—and an individual’s social engagement and mental health (Grov et al., 2010; McIntosh & Rosselli, 2012). This finding points to the need for policy and societal changes to address stigma, issues with financial support and other systems, and other elements of the environmental context. Occupational therapists are skilled in considering environmental factors and their influence upon occupational performance and engagement. Thus, occupational therapy has an important role in promoting social participation in older women living with HIV. Additionally, traditional HIV management tends to target the impairments that accompany the disorder, while our findings indicate a need to also address participation restrictions. Providing holistic support is an important addition to traditional HIV management, which is mainly focused on addressing medical issues and maintaining physical wellness.
The findings suggest that some older adults grow more resilient and adapt to their health challenges as they age, a finding that is consistent with the literature that describes adults thriving despite challenges related to HIV, aging, and other life circumstances (Emlet et al., 2011; Mavandadi et al., 2009). This finding reinforces that occupational therapists working with this client population should consider clients’ strengths and resources when collaboratively devising therapeutic goals. Some women expressed that they were living well in spite of their HIV and age and were in fact looking forward to many aspects of the future, such as spending time with their families. Our model assists in identifying variable factors that may be targets for interventions to decrease social isolation and move the client to the right of the continuum toward social engagement.
Many of the challenges identified by participants were not exclusive to older women but have been widely reported by those individuals living with HIV. Solomon and Wilkins (2008) found that experiencing barriers to work was associated with decreased participation. Although this study focused on older women with HIV, barriers to employment also functioned as barriers to social participation. Stigma experienced by people living with HIV has been reported across all ages and genders (Mahajan et al., 2008). Solomon and Wilkins noted that fearing disclosure and stigma was associated with decreased participation in women with HIV. As noted above, our findings highlight the complexity and multidimensional nature of stigma experienced by older women. Women perceived stigma stemming from their culture, gender, sexual orientation, HIV status, and age. This finding goes beyond the double or triple jeopardy reported in the literature and points to the need for widespread intervention and education to reduce stigma experienced by older women living with HIV. Indeed, programs and policies geared toward healthy aging, HIV, and rehabilitation ought to include elements aimed at reducing stigma and discrimination (Gahagan, Ross, Hill-Mann, & Lewellen, 2012). Given occupational therapists’ unique expertise in advocacy, the profession is well suited to advocate for women aging with HIV (Dhillon, Wilkins, Law, Stewart, & Tremblay, 2010).
Study Limitations
A limitation of this study is that we did not do theoretical sampling due to time constraints on the project. Theoretical sampling would have allowed us to explicate our categories and concepts more fully (Charmaz, 2006). This study is limited in that participants were recruited through HIV clinics and ASOs; therefore, it is possible that the perceptions of women who were less involved in their communities or less mobile were underrepresented. Additionally, while some participants speculated about the unique challenges of women living with HIV, such as balancing HIV management with fulfilling a caregiver role and accessing HIV services that were primarily geared toward gay men, it was difficult to uncover the factors that were uniquely experienced by older women aging with HIV. Future research should focus on elucidating how older women’s experiences aging with HIV differ from those of others living with HIV (i.e., younger women, younger men, and older men).
Overall Implications for Practice
These findings reinforce the role of occupational therapists in identifying areas of clients’ lives in which participation restrictions are present and facilitating the collaborative development of client-centred goals (Canadian Working Group on HIV and Rehabilitation, 2012). Using these findings to inform assessment and goal setting may be particularly beneficial for individuals who experience similar challenges to the women in this study, such as feeling “stuck” and not knowing how to devise or work toward goals for their future.
Conclusion
Older women aging with HIV experience social participation along a continuum that varies from social isolation to social engagement. Where an individual lies along this continuum is dependent on individual perceptions and contextual influences that may facilitate or hinder participation. Occupational therapists, with a focus on enabling participation and facilitating client-centred change, are well equipped to support older women living with HIV to optimize their social participation.
Footnotes
Funding:
This research was supported by a grant from the Canadian Institutes for Health Research (CIHR) to Dr. Solomon (Grant No. 206873). Dr. O’Brien is supported by a CIHR New Investigator Award.
Key Messages
Older women aging with HIV experience social participation along a continuum that varies from social isolation to social engagement. Where an individual lies along this continuum is dependent on individual perceptions and contextual influences that may facilitate or hinder participation. Occupational therapists’ knowledge, skills, values, and professional vision provide a useful lens through which to view the social participation of women aging with HIV and shape both individual interventions and broader advocacy efforts.
Acknowledgements
The authors would like to thank the women for their participation in the study as well as Nicole Gervais for her assistance with data collection and her administrative support.