
Abstract
Background.
Low-income older adult populations have increased vulnerability to occupational engagement barriers and poor health outcomes while aging in community settings.
Purpose.
The purpose of this study was to examine the relationship between community navigation and well-being for low-income older adults.
Method.
Community-dwelling older adults (N = 10) were recruited for this multimethod observational cohort study, which employed GPS data, measures of well-being, and semistructured interviews across 12 months. Grounded theory processes were followed to analyze and integrate the qualitative, quantitative, and spatial data.
Findings.
Findings were three patterns of community navigation. In particular, patterns of being chronically underoccupied were noted for this low-income population. Specific place-based challenges are explained along with strategies used to mitigate these challenges.
Implications.
Supporting community navigation, especially social interaction opportunities, can maximize well-being; and older residents’ occupational participation may be unnecessarily curtailed by geographic, economic, and social factors beyond their control. Community navigation strategies should be considered holistically by occupational therapists as part of interventions supporting aging in place.
Aspects of the community in which an older adult lives have been linked to general well-being in older age (Oswald, Jopp, Rott, & Wahl, 2011; Yang & Sanford, 2012). There is evidence that detrimental aspects of the built environment impinge on older adults’ activity within a community (Clarke & Gallagher, 2013; Rantakokko et al., 2014) and that restrictive social connections can negatively affect participation (Levasseur et al., 2015) and mental health (Fiori, Antonucci, & Cortina, 2006). The various dimensions that are thought to make a community age-friendly are the focus of significant research and grassroots attention (Lui, Everingham, Warburton, Cuthill, & Bartlett, 2009).
Community mobility is an important element of this person–place relationship, and it supports the ongoing ability to age in place and engage in meaningful and necessary occupations (American Occupational Therapy Association, 2016). Community navigation is used here as a term to include community mobility as well as the social and temporal considerations, physical abilities, personal patterns and preferences, and social and physical dimensions of out-of-home participation. Community navigation enables older adults to meet basic daily needs, to develop and maintain strong social relationships (Heatwole Shank & Cutchin, 2016), and to engage in meaningful occupations. Therefore, it follows that limited community navigation and occupational engagement are associated with diminished access to activities outside of the home (Zeitler, Buys, Aird, & Miller, 2012) and lower life satisfaction (Oswald et al., 2011). Lower activity level is also predictive of poorer long-term health outcomes (Menec, 2003). Supporting older adults’ ability to be out and about in the community therefore has the potential to mediate risks and maximize positive outcomes.
There is clear evidence within the occupational therapy literature that several types of interventions can be effective in supporting older adults’ participation in the life situations and roles that enable aging in place. Home-based interventions (e.g., Gitlin et al., 2006; Szanton et al., 2011; Zingmark & Bernspang, 2011) as well as driving assessments and interventions (e.g., Alvarez & Classen, 2018; Vrkljan, McGrath, & Letts, 2011) have long been a focus for occupational therapists. However, there is increasing attention within the field to ways that social participation is also a critical occupational concern for older adults in community settings, with direct links to health outcomes and quality of life. In a systematic review of evidence for leisure engagement and social participation interventions, Smallfield and Molitor (2018) found that there is strong evidence supporting the effectiveness of occupational therapy group interventions to support social participation and that education can increase leisure engagement for community-dwelling older adults.
Research by occupational therapists has also begun to examine the structural factors that affect community navigation and participation. For example, Jonasdottir and Polgar (2018) reviewed evidence about the services, systems, and policies that affect the mobility patterns of individuals who use assistive mobility devices. They concluded that few structure- and policy-centred studies exist, despite evidence that these factors shape how individuals participate in the community. For older adults aging in place, the ability to engage in necessary and discretionary occupations involves complex orchestration of home and community spaces, and social and temporal factors. Little research has examined the situated and place-based ways that older adults move in and through community settings as they engage in occupations.
One group that is consistently underrepresented in the literature about community mobility and age-friendly spaces is low-income older adults. However, we know that low-income older adults may be particularly vulnerable to changes in neighbourhood demographics or safety (Yen, Michael, & Perdue, 2009) and have an increased risk for social isolation (Rantakokko et al., 2014). Clarke and Gallagher (2013) examined underserved older adults in Detroit and highlighted the unique mobility concerns of older adults living in a city with significant socioeconomic decline. They argued that this group is at “greatest risk for physical decline and institutionalization” (Clarke & Gallagher, 2013, p. 1005). This is particularly the case because attempts to increase supports for older adults in community contexts rarely consider this economic variation in experiences and need for services (Lehning, Smith, & Dunkle, 2014).
Community navigation is an integral part of the relationship of older adults and the communities in which they age and engage. Lack of clarity about mechanisms that promote participation and well-being have stemmed in part from largely self-report and qualitative methodologies. To answer questions about complex and multidimensional experience, mixed methodologies are needed to both access and represent the complexity and underlying relationships of community-situated occupation. Therefore, the purpose of this research is to examine community navigation using qualitative and GPS methods in order to identify patterns of participation, spatial behaviour, and well-being for lower-income adults.
Method
In order to examine the relationship between community navigation and well-being for community-dwelling low-income adults, we utilized a mixed-methods observational cohort design, where data were collected over 12 months. Procedures for the concurrent collection of quantitative well-being scores, measures of community navigation via GPS, and in-depth interviews are described next, including the integrated analysis processes.
Participants
Low-income community-dwelling older adults were recruited to participate via fliers, and inclusion criteria were being 65 years old or older, living in federally subsidized senior housing, and reporting leaving home at least twice per week. Individuals were excluded from the study if they intended to move within the coming year, were hospitalized three or more times in the previous year, or demonstrated a cognitive impairment that limited functional recall. Approval for this study was granted by the authors’ university institutional review board, and all participants provided voluntary consent to participate. At the conclusion of each phase of data collection, each was given a $25 grocery gift card retention incentive. All names and locations are pseudonyms.
Setting
This study took place in a small suburban town outlying a large metropolitan area in the United States; the town is bounded by an eight-lane beltway on several sides yet within a short distance from other suburban and rural residential areas. As of the 2010 U.S. Census, the town population was 55,000, and 16.5% of the population was 65 years or older. The median income was $77,680, with a poverty rate of 12.8% (U.S. Census Bureau, 2017). This area was chosen based on the number of federally subsidized senior housing complexes, the accessibility of public transportation, and the proximity of the town’s facilities and services. Within a mile of study sites are numerous independent retailers, a large indoor shopping mall, a recently developed pedestrian square with a cinema and restaurants, and an outdoor mall with over 15 retailers. Multiple residential buildings dot the downtown, including high-end luxury apartments and townhomes. Several main roads run through downtown, intersecting at a busy traffic circle.
Data Collection
The data collection involved semistructured interviews, administration of well-being measures, and the use of GPS loggers. Data were collected twice, first during March 2017 (Time 1) and again 12 months later, in March 2018 (at Time 2). Participants were contacted regularly throughout the study to aid in retention and maintain rapport. Participants carried the GPS device for approximately 10 days at Time 1 and completed well-being measures and semistructured interviews (lasting approximately 45 min each) at Time 1 and Time 2. At Time 2, interviews involved drawing maps (tracing routes on provided municipal maps), which were also included as data for each participant.
Spatial data
Participants carried GPS loggers for approximately 10 days (range 9–12 days), which was the length of battery life of the logger. Spatial data were uploaded from the GPS loggers and were composed of a geographical point recorded every 10 s while a participant was outside of his or her apartment building. Spatial variables derived from these data were average distance traveled, number of trips per day, calculated activity space, and number and repetition of destinations. Because number of total days varied slightly among participants, analyses were done using averages by day and by trip to aid in comparisons. GPS data were also uploaded using spatial software to visualize individual maps.
Quantitative data
Well-being indicators selected for this study were a self-rated health item (SRH) and the Late-Life Function and Disability Index (LLFDI). These measures were chosen due to their ability to capture social and functional dimensions of older adults’ well-being. The SRH is a single-item questionnaire that asks, “In general, would you say your health is…” with Likert-type scaled responses ranging from excellent (5) to poor (1). SRH has been closely correlated with objective well-being outcomes (McDowell, 2010) and has high utility as a concise addition to a larger battery of assessments. The LLFDI measures level of satisfaction with functional performance and the extent of perceived limitations (Jette et al., 2013). Test-retest reliability for the functional component was high (intraclass correlation [ICC] = .91–.98; Haley et al., 2002) and was found to be moderate to high (ICC = .68–.82) for the participation component (Jette et al., 2002).
Qualitative data
Qualitative data were collected via semistructured interviews, which were audio recorded with portable digital recorders. Initial interviews at Time 1 were used to review the spatial patterns seen in the GPS-generated maps. Additional semistructured questions addressed the participant’s daily activities, barriers to participation, and neighbourhood features. Interviews during Time 2 took place a year later, and additional questions were asked about new activities clients engaged in and more detailed questions about the neighbourhood context, such as the presence of or change in destinations. Interviews were conducted in the participants’ homes.
Data management
After collection, the data were uploaded from portable devices to a password-protected computer and saved without any identifying information. Participants had the option to exclude specific locations or routes recorded by the GPS loggers; however, none made this request. Identities were protected by assigning pseudonyms to participants and their residences. Names, home addresses, and phone numbers were maintained separately.
Analysis
Analysis of the multiple types of data occurred iteratively, beginning with Time 1 data and continuing into the final stages of writing. Following Charmaz’s (2014) grounded theory procedures, interviews were transcribed and all members of the research team performed sequential rounds of open coding to achieve code saturation. Researchers discussed and sorted all codes and identified patterns and discrepancies among the experiences of participants. Focused codes were developed and defined and were reapplied to the transcripts. Simultaneously, spatial data from each GPS logger were stored in the form of a map for each participant, a log with listed times and destinations, and a data file. ArcMap spatial software was used to calculate basic summary statistics of each participant’s community navigation and to derive measures of distance and activity space. A matrix was created to juxtapose and integrate the various types of data (O’Cathain, Murphy, & Nicholl, 2010), including focused codes, example quotes from participants, spatial data, and well-being scores. Again adopting a grounded theory approach, the team made constant comparisons across and among participants, which served to highlight topics for memo writing; then topics were developed into emergent concepts. Data integration also occurred during the final step of analysis, where patterns and discrepancies across all data types were further developed in memos; this interpretive writing, done by all members of the research team, served as the foundation for representation and for honing the findings presented here.
Findings
Data collected through GPS mapping data, well-being measures, and in-depth interviews offer insights into the place-based occupational experiences of low-income older adults. We describe participation patterns related to community navigation, challenges that arose, and related problem-solving strategies participants used to negotiate these challenges. Findings are presented using data from multiple sources to provide a holistic understanding of participants’ experiences.
Sample
Participants were 10 older adults ranging from 67 to 96 years old, with a mean age of 77.1 years. The sample consisted of eight females and two males; six of the participants were Caucasian, and four were African American. Although it was not part of inclusion criteria, all participants lived alone. Six were able to drive; however, only four owned a vehicle and drove themselves as primary transportation. Four of the 10 used public transportation, and another third relied exclusively on rides from others for any community navigation. Many used some combination of methods for transportation (see Table 1). In terms of well-being, participants’ SRH scores ranged from 2 to 5 (fair to excellent), and most participants’ LLFDI scores for functional limitation and participation restriction fell within one standard deviation from the mean. All participants left home during the course of the study but varied from rarely to daily. The number and type of occupation destinations also varied significantly (see Table 2).
Sample Demographics and Transportation Mode
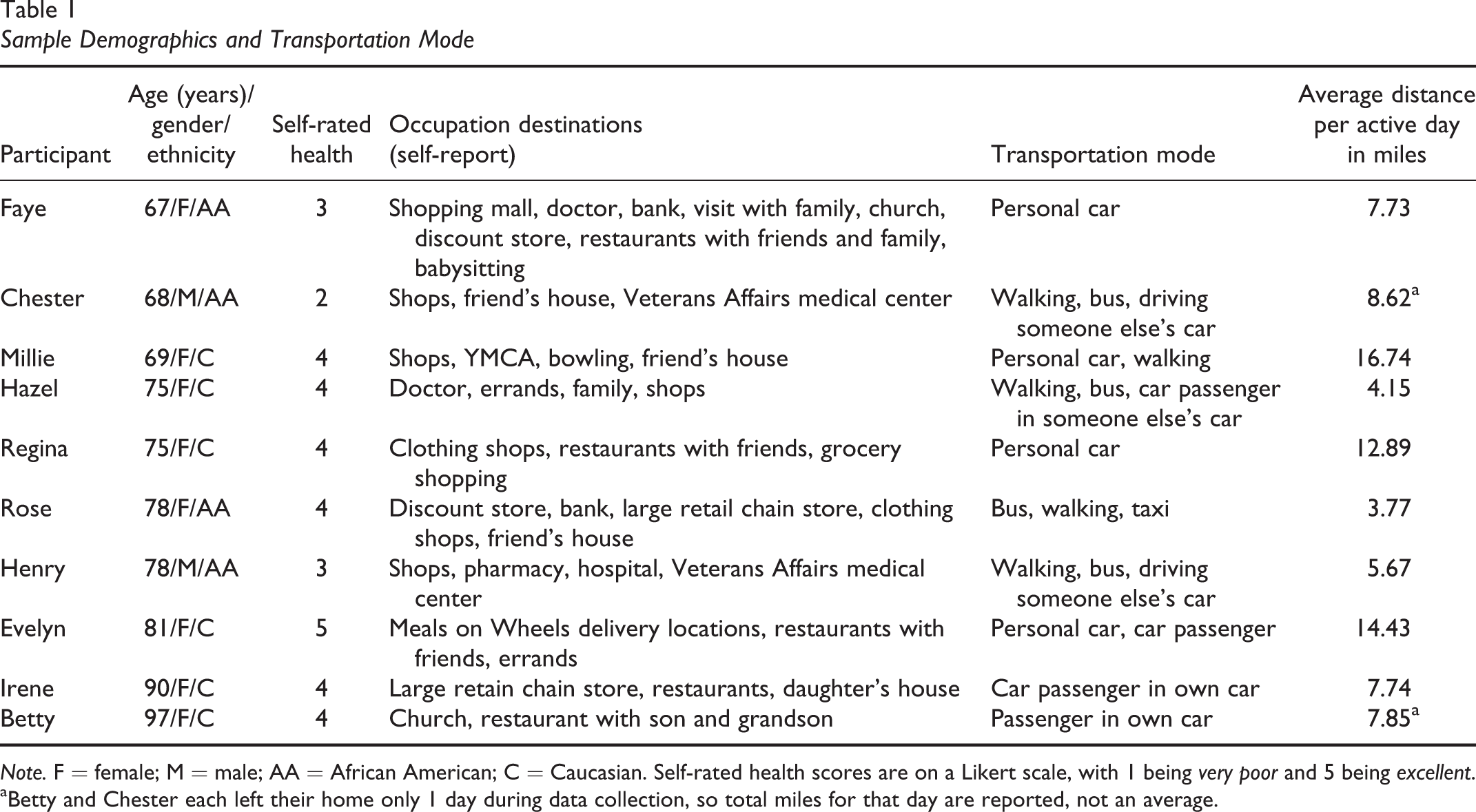
Note. F = female; M = male; AA = African American; C = Caucasian. Self-rated health scores are on a Likert scale, with 1 being very poor and 5 being excellent.
aBetty and Chester each left their home only 1 day during data collection, so total miles for that day are reported, not an average.
Well-Being and Community Navigation (N = 10)
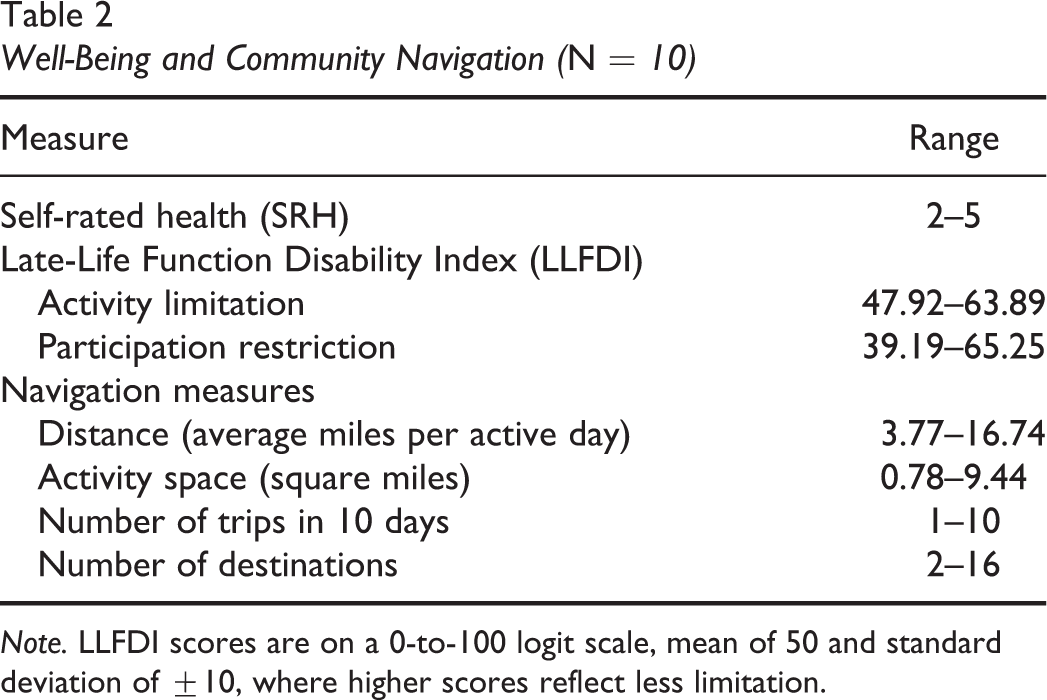
Note. LLFDI scores are on a 0-to-100 logit scale, mean of 50 and standard deviation of ±10, where higher scores reflect less limitation.
Participation Patterns
Participants’ community navigation was directly linked to the ways they participated in their out-of-home occupations. Predominant occupations included doing errands, spending time with friends and family, medical appointments, shopping or leisure activities, and religious services. Patterns that shaped the doing of these occupations were the social dimension of participation, the significance of familiarity, and the experience of being chronically underoccupied.
The social dimension of participation
All participants left home in order to engage in occupations that they described as having a strong social component. Going to restaurants with friends, attending church with a family member, or visiting someone in his or her home were frequently seen on participants’ maps and described during interviews as meaningful. In some cases, the timing of errands was intricately linked to social time with family, such as Betty’s reliance on her sons, who “take [her] anywhere.” Others went out frequently and seemed to do so primarily to be around other people. Evelyn said, “I like people; I like to go out and be social”; and Faye echoed, “I try to get out of here every day.” Both of these participants’ maps showed almost daily trips away from home, although often these trips to “be social” were also described as “doing errands” at locations like the grocery store or pharmacy. For all participants, the desire to connect with others often precipitated travel out of their homes, no matter how (in)frequent.
The social influence on participation patterns was also indirect. Some participants had relationships with family and friends who were not within close proximity of the building or even the same town but instead were located in another city suburb or in a more rural part of the county. These relationships influenced the distances traveled and selection of destinations by participants. For instance, Millie explained, “I do organize my errands—if I’m in a certain area, if I’m near my sister’s, I do my laundry, then I go to [the grocery store], the one close to her, I go there because I’m going right by it.” Millie’s comments were consistent with her map, which showed clusters of destinations in her sister’s neighbourhood but very few within her own. Similarly, Henry was able to drive but did not have a car of his own. His map showed walking trips from his building to nearby shops, but his driving originated from a friend’s home in a nearby neighbourhood, where he would act as informal chauffeur for several women once a week. These trips reflected the joint nature and scheduling of their community navigation.
Significance of familiarity
Related to this social dimension of participation, participants espoused a strong preference for locations that were familiar. Participation patterns that reflected this affinity for the familiar included using repeated routes, avoiding certain areas, and travelling farther distances to ensure familiarity. These patterns were identified through visual analysis of the maps generated by the GPS data. Most noticeably, participants typically traveled down repeated roadways. In some instances, this travel was toward a habitual destination; in others, it was a path of avoidance (several spoke of avoiding driving through the traffic circle downtown). Faye shrugged and said, “I do the same thing. I stick to a routine.” For most, however, the repetition of familiar roads was an unreflected aspect of community navigation.
Participants tended to be more cognizant of the fact that they avoided certain areas. Evelyn said, “I don’t really care for driving in the city. I really don’t need anything down there; it’s busy busy busy. I could take you cross-country but I couldn’t take you downtown and show you nothing.” Evelyn’s map showed regular trips away from home, which encircled the perimeter of a nearby metropolitan area but never broached downtown. Others spoke of avoiding major highways and of the back roads they used as alternatives. Patterns of mobility were thus shaped by both destinations and roadways that felt familiar and usable—places that felt safe.
Finally, the significance of familiarity showed up in several participants’ patterns of travelling farther than necessary to go to a destination—often an errand location—that was well known. For example, Millie travelled to a Walmart store in a different town, driving four miles farther than necessary since there was also a Walmart within several blocks of her building. Millie explained that she “knows the store”; she later alluded to the fact that the one farther from her was in a middle-class neighbourhood, compared to the one nearby, whose clientele were more socioeconomically and racially diverse. Familiarity of both route and place was appealing and influential as these older adults organized their trips away from home.
Being underoccupied
The previous descriptions of patterns of participation should not overshadow the final pattern noted in our data, which was a pervasive and seemingly chronic experience of being underoccupied. Although all participants were quick to respond to questions about their daily occupations, questions in which they were asked to explain or reflect on aspects of their map offered different insights. For most participants, their daily occupations—and out-of-home participation in particular—felt unnecessarily curtailed. “They’re just closing up everything… There are not too many activities around here,” Rose said. Similarly, Irene lamented that “a lot of activities are no more, so I spend more time in my room, which isn’t good.” Sometimes their perception of having few “activities” and places to go were phrased through concern for others: “They need something to do to make them feel good, and they don’t have it,” Regina said of her neighbours. The nearby high-end restaurants and developments were rarely mentioned and never appeared as destinations on the GPS logs; however, a local grocery store had relocated between Time 1 and Time 2, and a nearby convenience store also closed; these losses were acutely felt and mentioned by multiple participants in the follow-up interviews.
Expressing a desire for more things to do was often related to concerns about health and safety. Chester said, “I have to walk. I’m not able to go far without…having pain,” and therefore he was limited to options that were available in a small geographic radius. Betty reported, “I’ve been told not to walk around here far because you get in trouble…so I don’t go anywhere by myself except for right around this block.” She was aware that she could use public transportation, but she said she did not “have to use it.” Betty left her building only once during the 10 days that she carried the GPS logger, driven to church by her son. Chester and Betty both scored below the mean, and lowest among the sample, on the LLFDI measure of functional limitation.
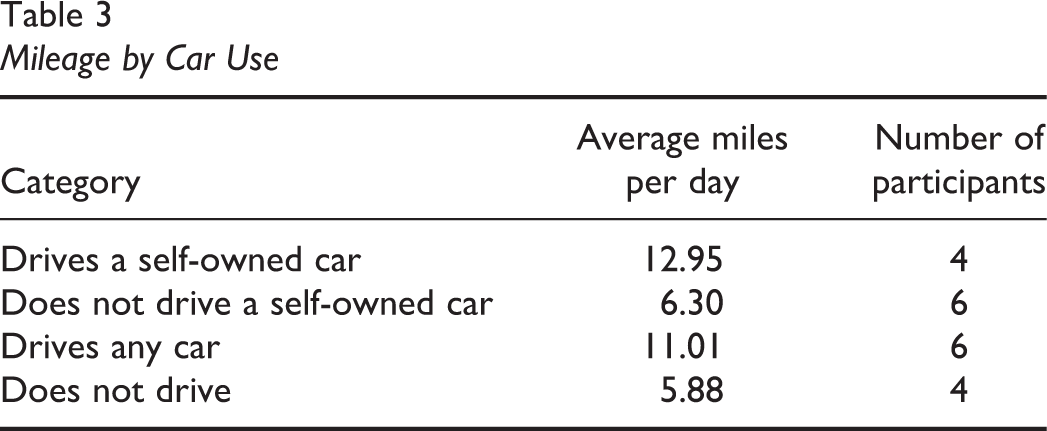
Not surprisingly, access to a vehicle and an ability to drive had a significant impact on the extent of community navigation by participants. In this sample, four out of the 10 participants had a car and were able to drive themselves; others used public transportation, walking, rides with others, or taxis as their modes of transportation. These four “auto-mobile” participants—Millie, Faye, Evelyn, and Regina—left home more frequently, had among the highest scores on the LLFDI measures of function and participation and on SRH, and did not report this same sense of being underoccupied. Additionally, participants who drove any car, including using their own car or borrowing someone else’s, travelled almost twice as far as those who were not able to drive (see Table 3), which opened up significantly more possibilities for participation in occupation.
Mileage by Car Use
Challenges and Strategies of Participation
In addition to the transportation challenges described above, participants had challenging health conditions, aspects of the built and natural environment, and the indirectly discussed limitations of finances. These limitations to going out and doing occupations in the community, particularly when it came to health challenges, were congruent with both well-being measures and spatial data. For example, Evelyn, the participant with the highest SRH score, travelled about twice as far as Chester, the participant with the lowest SRH score. Despite participants’ relatively high self-ratings, health conditions still emerged as a significant barrier for many participants. Participants with more severe chronic health conditions reported that it affected their participation, such as Chester’s pain, Millie’s shortness of breath, and Irene’s low vision. Many explicitly linked their health and occupational engagement during interviews, concisely summed by Henry’s comment that “if you are not growing, moving, or doing anything, then they may as well throw the dirt on you.” Participants repeatedly reported limitations in their occupations, often speaking about restrictions to their daily choices and the extent to which they were able to participate in the community.
However, participants’ accounts and maps reflected strategies relative to these challenges. For example, in response to questions about her timing of trips, Faye explained, I try to do everything after the traffic dies down in the morning and before it picks up in the afternoon. I only go out once and do all of my errands for the day. The more people out on the street, the more chances of something happening.
A second participant expressed a similar sentiment, explaining, “There is plenty of traffic here at certain hours of the day, but you know how to avoid that” (Hazel). Participants also utilized specific route strategies to navigate in their communities. Faye described avoiding driving through the traffic circle located just a short distance from her home. Hazel, Regina, and Chester primarily utilized smaller roads and avoided using the beltway. Many of the participants discussed their choice of walking routes, including routes with flat surfaces and shorter distances. Whether driving or walking, participants were aware of this aspect of their community navigation and actively chose routes that minimized features that were more challenging.
In contrast, one strategy for dealing with challenges that seemed to be unreflected, yet consistent across multiple participants, was a cognitive shift in expectations about how they participated in out-of-home occupations. For some, this cognitive strategy took the form of minimizing the significance of leaving home. Henry said, “I only go out depending on the business I have to take care of.” Rose explained, “I just go out when I need something,” and Faye said, “I do the things I need to, do my business.” The sense of “necessary business”—which was never extensive—as being the main reason to leave home was also echoed by Chester, who commented (while inspecting his map that showed one trip away from home in the span of 10 days), “I really don’t have any places where I have to go, as far as activitywise.” This reframing process, where out-of-home trips entailed only “business,” meant that participants were not focusing on the leisure or discretionary trips that were absent from their routines.
Although they did express a feeling of being underoccupied and wishing for more to do, there was also an emphasis on accomplishing what was necessary and not dwelling on anything else. The use of these cognitive reframing strategies allowed the older adults with significant health concerns and mobility restrictions to report relatively high levels of well-being and few barriers to community participation.
Discussion
These patterns and strategies offer important insights into the community navigation of low-income older adults and suggest ways that well-being is related to and sustained by participation. Several dimensions of participation presented here are consistent with existing literature. For example, the cognitive strategies relate to findings from Goins et al. (2015), who identified older adults’ problem-solving strategies, such as positive attitude, and from Heatwole Shank and Cutchin (2010), who described cognitive reframing processes that help older adults negotiate change. In addition, our findings confirm previous descriptions of older adults’ route strategies (Zhao, Yamamoto, & Morikawa, 2018) and further identified situations that older adults may avoid, such as traffic circles. Our study extends this body of research by connecting these strategies and patterns of participation, previously identified in isolation, to observed spatial behaviour and occupational engagement for a community-dwelling population.
One of the gaps in this literature is the dearth of evidence relating specifically to the low-income population. Although directly asked about things that made their participation challenging, none of the participants answered this question with reference to financial constraint. When finances did come up, it was in reference to limited gas money or not having change to ride the bus. In comparison to more affluent and urban community-dwelling populations (Yen et al., 2016), this sample had a notably restricted range (distance) and quantity of destinations.
For many participants in our sample, the options for out-of-home activities were few. Despite substantial new retail and leisure development within several blocks, these venues were described as cost prohibitive for the older adults living nearby. Even other walkable destinations, such as a convenience store, a gas station, and several smaller restaurants, entailed making a purchase. Although the location of the senior housing buildings in this town may have been located near amenities, the effect of being inside this ring of costly options, which were not perceived as occupational possibilities (Laliberte Rudman, 2006) by this population, created an occupational desert. As Robinson, Rickenback, and Lachman (2015) suggested, older adults with diminished resources may particularly rely on a process of “compensation”—part of the selection, optimization, and compensation model of dealing with change in function over time—as they participate via contexts with limited possibilities for engaging in occupation beyond their home. In fact, for the low-income older adults in this study, compensation for declining ability to navigate in the community largely meant staying at home most days of the week despite the expressed value of getting out and being socially engaged.
Implications for Occupational Therapy
There are several significant implications for the practice of occupational therapy. Our research found that older adults have a strong desire for social interactions, specifically through participation in occupations involving family or friends. This is a powerful source of motivation and an occupation through which strategies for community mobility, social interaction skills, cognitive habit training, and endurance can be applied. It should be noted that a trip to the grocery store could also fulfil this social need for some individuals, and identifying the social dimension of even “necessary” occupations may be a useful starting place instead of assuming that social occupations are leisure oriented. Further, the “social” occupations (such as seasonal parties, game nights, and birthday celebrations) facilitated by building staff at each of the three apartment complexes were rarely mentioned by participants, suggesting that this type of programming may play less of a role in supporting well-being and perceptions of meaningful participation in a community context than occupations that are often considered “instrumental.”
Second, this research underscores the importance of considering the living environment in all aging-in-place interventions, extending from the home (e.g., Liu, Change, & Change, 2018) to community-situated occupations. Cognitive strategies, such as the ones employed by these individuals, will be most successful when they reflect nuances of specific communities, such as the potential benefit of travelling father to maintain familiarity or centralizing errands near a friend or family member. Although cognitive strategies and route planning may be highly individualized, occupational therapists should also advocate for community spaces and routes that facilitate moving through community—not just the accessibility of a specific building, for example—and that allow people who are aging in place to have places to go and things to do that are not contingent upon “necessity” or consumer activity.
A final implication for occupational therapy is the utility of using mapping to understand participation. This innovative approach to visualizing patterns, habits, and routines—often that the individual did not realize and could not have verbalized in an interview or assessment—was a valuable tool to shed light on real participation in real environments. This method can be replicated with other populations to understand patterns of participation in real-world settings. It may also be used as an outcome or indicator of effectiveness for interventions or programs targeting community navigation in both practice and research capacities.
Limitations
The primary limitation of our study is that the data were collected from 10 participants from three buildings within one town. Factors influencing the experience of these low-income older adults may be situationally unique given the layout and amenities of this place. Additionally, our semistructured interview template was based on a larger protocol about community navigation and contained no questions specific to being low income. Such questions may have yielded more specific information about how finances affected their occupations and should be included in future research with this population. Finally, the GPS data were collected only at a single point in time. Although assessing change over time was not the intent of this research, additional points would have provided more confidence beyond self-report that the collected data were typical for the participants and not outliers in terms of navigation extent or type. Future research about community navigation, particularly employing GPS methods, should include a longitudinal component to increase the reliability of measures.
Conclusion
Our findings demonstrate how social interaction shapes occupational participation patterns and represent several problem-solving strategies used by older adults to negotiate changes while aging in a community context. We also describe the experience of being underoccupied, which is influenced by multiple factors, such as community features and personal auto-mobility. The use of mixed methods (qualitative semistructured interviews, mapping, GPS data, and SRH measures) allows for interpretation of a complex issue and presents a holistic understanding of how low-income older adults navigate their environment in order to satisfactorily participate in their occupations.
The experiences and patterns of being underoccupied particularly serve to highlight the geographical, social, and financial constraints of going out and doing the occupations of daily life while aging in place. Although individual well-being is certainly linked to these patterns, issues of access transcend individual-level outcomes. Occupational therapists can address this aspect of aging in place through identifying and further developing strategies to support social interaction through community participation. Further, occupational therapists can play a role in advocating for inclusive participation practices and policies by service providers, city program developers, and city planners. Participation in community contexts via community navigation can support and extend well-being for older adults aging in place and must be addressed through multiple holistic and place-based solutions.
Key Messages
The social aspect of instrumental occupations is highly motivating and shapes community participation patterns. Low-income older adults are vulnerable to being underoccupied in both necessary and discretionary occupations. Strategies to support community navigation while aging in place include route planning, identifying destinations, and cognitive reframing. Occupational therapists should consider ways that occupations satisfy both social and instrumental needs for those aging in place and can advocate for participation-supporting mobility options, housing locations, and public spaces.
Footnotes
Acknowledgements
The authors gratefully acknowledge Christina Costill, Karena Foreman, Erica Good, Emily Grap, Lauren Hoover, Jessica Lloyd, Tasie Nwachukwu, Brittney Pettewey, Eileen Teunis, and Karen Van Orden for assistance with data collection and early stages of analysis. This project was funded by a grant from the Towson University Academy of Scholars.
Funding
This project was funded by a grant to the first author from the Towson University Academy of Scholars.