
Abstract
Introduction
Cognitive stimulation therapy (CST) is an evidence-based psychosocial intervention for individuals with mild to moderate dementia that has shown to improve and maintain cognitive health irrespective of an individual receiving drug therapies for dementia (Spector et al., 2003). Despite there being limited high-quality research on CST's effectiveness in improving everyday functioning, well-being, and quality of life, further exploration is warranted (Woods et al., 2012). Trained individuals with knowledge and experience supporting individuals with dementia can implement CST. However, occupational therapists are particularly well suited for this role, due to their clinical skill set in providing functionally oriented activities and adaptations according to individual or group needs (Spector et al., 2008; Yuill & Hollis, 2011). Implementation of CST by an occupational therapist may also strengthen implementation impact, given their ability to continuously monitor, grade, and modify client activities using a person-centered therapeutic lens (Salmon, 2006). Occupational therapy outcomes often focus on both occupational performance and occupational well-being and an individual's subjective experiences of their occupational lives are an important occupational therapy outcome (Doble & Santha, 2008). Given the limited research on CST's impact on well-being, occupational therapists who often collect self-reported measures of individuals’ subjective experiences of their occupational lives may contribute to this gap in research. The World Alzheimer's Report from 2011 identified that CST should be routinely provided to those living with early-stage dementia (Prince et al., 2011). Although many other countries have adopted and implemented CST since its conception and as the evidence for its use became available, the systematic implementation of CST by a trained occupational therapist has not been studied in Canada.
Background
Presently, there are a half-million Canadians living with dementia, with 25,000 new cases diagnosed every year. By 2031, that number is expected to rise to 937,000 people, which is a 66% increase (Chambers et al., 2016). Dementia has physical, psychological, social, and economic impacts, not only for those affected, but also for their carers and society at large (World Health Organization, 2020). Dementia is a chronic and progressive disease with both pharmacological and non-pharmacological interventions available to mitigate the progression. There is no cure for most dementias and therefore, the effectiveness of such treatments cannot be measured by complete functional recovery (Chapman et al., 2004). Self-management has become a standard for the prevention and management of chronic diseases (Mountain, 2006). According to the Canadian Alzheimer's Society research priorities, evidence-based person-centered and non-pharmacological approaches for managing symptoms of dementia are among the top 10 research priorities (Bethell et al., 2018). A study by Quinn, Toms, Anderson, et al. (2016) suggests evidence contrary to the belief that self-management is not appropriate for people with dementia due to cognitive impairments (Quinn, Toms, Jones, et al. 2016). Approaching dementia care with this therapeutic lens allows for the exploration of how psychosocial interventions may benefit self-management in this population. For example, skills in activities of daily living (ADLs) and self-efficacy for disease management, as well as having hope, are all indicators that have been associated with better outcomes and longevity in persons with chronic diseases, especially in terms of their ability to remain at home independently (Ibrahim et al., 2017).
Even though CST as a psychosocial intervention was not directly developed to improve self-management for people with dementia, it incorporates several self-management components including information provision, communication, social support, and skills training. Evidence shows that CST is particularly successful in improving the cognition of people with dementia in the everyday context, as well as improving their language skills (i.e., naming, word finding, comprehension, etc.) (Spector et al., 2010). Implementation of community-based CST programs has demonstrated benefits across both clinical (i.e., cognition, functional autonomy, mood, behavior, etc.) and psychosocial (i.e., well-being, social inclusion, quality of life, delayed institutionalization, and global costs) outcomes for individuals and communities at large (Yates et al., 2017). The aim of CST is to provide cognitive stimulation to improve general cognitive functioning through cognitive training and rehabilitation that is person-centered. Additional benefits of psychosocial treatment include a positive mindset for family, care partners, and clients through the provision of strategies to prevent and solve behavioral problems, and to cope with functional and emotional consequences of cognitive decline (Yates et al., 2017).
Although CST has been widely studied and implemented globally, little research has been done on its implementation process in Canada. The CST facilitator requires a specific skill set to effectively manage individual and group dynamics, to be flexible in person-centered care, to provide motivation and encouragement, to adapt session content and an interaction style, as well as to maintain a continued sensitivity to individual and group needs (Spector et al., 2008). This unique skill set aligns well with those of occupational therapists, who are often responsible for providing psychosocial interventions to dementia patients (Yuill & Hollis, 2011). This alignment creates an opportunity to investigate the implementation of CST by registered occupational therapists in their practice setting. As CST is commercially available, and there is nationally available training on its implementation for occupational therapists in Canada, it would be beneficial to understand the effectiveness of their involvement in the implementation and delivery of CST in the Canadian health care setting. The successful implementation of CST is relevant to occupational therapists who have the skill set to deliver the therapy in practice as it offers an opportunity to positively impact the occupational performance of persons with dementia they serve (Streater et al., 2016). The CST program was designed by incorporating theoretical concepts of reality orientation, use of multi-sensory stimulation, and focusing on implicit memory (Yates et al., 2017). Designed to be enjoyable for the participants, this person-centered approach is important to occupational therapy practice as it differs from cognitive training which has the potential to be an insensitive experience for individuals with dementia (Yuill & Hollis, 2011).
The Ontario Dementia Strategy (2016) identified support for persons living with dementia as a top priority. To date, many successful initiatives have been implemented in Ontario that aim to support people living with dementia, such as Regional Geriatric Programs, Specialized Geriatric Services, and Behavioral Supports Ontario. These initiatives have helped to break down barriers and foster partnerships to help people live well with dementia. Implementation of CST within the context of these successful initiatives may be appropriate given the population base that is served and the opportunity for improved coordination and access to dementia care services. Aging at home or “aging in place” remains a priority of the Ontario health care system for its long-term sustainability to meet the needs of a rapidly aging population (“Aging with Confidence: Ontario's action plan for seniors,” 2017). It is therefore important that the implementation potential of CST be assessed in community-based settings to align with the province's priorities for research and routine care in the community for those with mild to moderate dementia. At a federal level, the top 10 priorities for dementia research in Canada, developed by The Canadian Dementia Priority Setting Partnership, identify three areas that this CST research addresses, including the implementation of best practices for care, nonpharmaceutical approaches to managing symptoms, and impact of early treatment (McGilton & Bethell, 2017).
Study Purpose
The objectives of the present study were to:
Deliver a community-based CST program to older adults with mild-to-moderate dementia led by a trained occupational therapist. Examine any changes in the self-reported measures of general self-efficacy and hope before and after the implementation of the CST Program. Evaluate the feasibility and satisfaction of implementing the CST Program within our health care setting.
Methods
A mixed-methods experimental pre/post design was used to address our objectives. The flow of our study design is in Appendix A. The sequential steps taken during intervention delivery are described below. Research and Ethics Board approval was obtained from North York General Hospital in Toronto, Ontario, Canada. All participants provided written informed consent to participate in the study.
Participants and Recruitment
Purposive sampling was used to recruit community-dwelling older adults (age 65 years and older) with mild-to-moderate dementia diagnosed within the last year. Inclusion criteria were the ability to speak and understand English, adequate vision, hearing and speech to participate in the conversation in a group setting, and ability to tolerate sitting for 1 hour. The recruitment process involved reviewing the study information and recruitment protocol with geriatricians at the clinic who were asked to identify patients with a diagnosis of mild-to-moderate dementia within the last year. Although CST is an appropriate intervention for any individual with mild-to-moderate dementia, study participant referrals were limited to those deemed capable of consent by the clinical judgment of referring geriatricians. Meeting with geriatricians and clinical staff members in person to review program details led to recruitment from all clinic staff.
PreCST Program: Screening and Baseline Measures
Each participant was invited for an initial study enrollment visit with the occupational therapist prior to starting the CST program. Following signed consent, the occupational therapist and occupational therapy assistant performed quantitative outcome measurements: the General Self Efficacy (GSE) Scale (Schwarzer & Jerusalem, 1995), and the Adult Hope Scale (AHS) (DiGasbarro et al., 2020).
CST Program Delivery
The program was delivered by two CST program facilitators (occupational therapist and occupational therapy assistant) both of whom have received formal training for CST implementation. They each have over 5 years of experience working with individuals with dementia and facilitating and leading seniors’ groups. The CST program facilitators incorporated the core principles of CST: mental stimulation, promoting new ideas, thoughts and associations, a focus on opinions rather than facts, maximizing the potential of people with dementia, respect, and person-centeredness (Spector et al., 2006). Participants were assigned to a program session based on their preference and availability. The delivery of the intervention mirrored the 14 sessions outlined in the CST manual “Making a Difference” (Spector et al., 2006). Group sessions were delivered twice a week for 1 hour. Upon completion of each session, participants completed a feedback survey about the session content related to their perceived level of challenge, engagement, and enjoyment. CST program facilitators completed subjective feedback on implementation and participation after each session using the monitoring progress record of the CST manual (Spector et al., 2006).
CST Program Evaluation
We performed a number of data collection activities to evaluate the implementation, delivery of, and satisfaction with the CST Program including approaches to assess the feasibility of continuing the program in the context of the coronavirus disease 2019 (COVID-19) pandemic.
Evaluations at the End of the CST Program. At the end of the 14 sessions of the CST program, participants completed the quantitative outcome measurements that were collected at baseline (the AHS and GSES), as well as a satisfaction survey (Appendix B) consisting of 10 questions using a 5-point Likert scale (where 1 is strongly disagree and 5 is strongly agree). We also evaluated the overall CST program through an end-of-session focus group, which was conducted in-person at the end of the 14 sessions for all participants. Focus group questions were related to identifying participants’ overall impressions of the CST Program, what they liked about it and suggestions for improvement (Appendix C). However, participants who were put on hold during the COVID-19 pandemic answered these focus group questions over the telephone (during the mid-point of the program after Session 7) and again in-person (at the end of the program after session 14). At the conclusion of the study, we also conducted a self-reflection focus group with CST Program facilitators (OT and OT assistant) led by an implementation scientist, to elicit their experience of the determinants (facilitators and barriers) of the CST Program implementation. The purpose of this exercise was to improve any future implementation of the CST Program.
Evaluation Throughout the CST Program. At the end of each of the 14 sessions, we administered a short evaluation survey to assess participants’ level of enjoyment, engagement as well as how challenging or stimulating they found each session. Appendix F shows the details for all session activities. The three dimensions were assessed using a 3-point scale (1 = not enjoyable, engaging, challenging or stimulating to 3 = very enjoyable, engaging, challenging or stimulating). These scores were monitored across these factors, and iteratively changing aspects of the session activities if mean scores < 3. Given the uncertainty of resuming the CST program under the COVID-19 public health restrictions, we also asked participants in the two initial CST groups who completed 7 of the 14 program sessions (n = 8) to provide feedback about the feasibility of delivering the CST program virtually (Appendix D). Data from these evaluations were used to identify potential program delivery changes to optimize the implementation of the CST program for subsequent groups.
Implementation Considerations
Implementation of the CST program was facilitated using the Reach, Effectiveness, Adoption, Implementation, Maintenance (RE-AIM) framework (Glasgow & Estabrooks, 2018). RE-AIM is an implementation science tool that can be used to plan for the evaluation of programs and can be used to encourage the consideration of essential program elements that can improve the sustainable adoption and implementation of effective, generalizable, and evidence-based interventions (Glasgow et al., 1999). Although well established, application of the RE-AIM framework in its entirety to complex interventions can be challenging in real-world community and clinical settings, particularly with the often-limited resources available for implementation (e.g., staff) (Glasgow & Estabrooks, 2018). To address this challenge, the RE-AIM developers recently provided a pragmatic approach to use RE-AIM in these settings, which involves the use of a familiar set of “who, what, when, where, how, and why” questions (Glasgow & Estabrooks, 2018). We applied the pragmatic RE-AIM questions (Appendix E) throughout the planning and implementation phases of the CST program to use it as a method to iteratively identify areas where adjustments may be necessary to achieve the desired outcomes (Glasgow et al., 1999; Glasgow & Estabrooks, 2018).
Outcomes and Measures
Outcomes were assessed across patient, process and implementation factors. Patient-reported outcome measures (PROMs) included self-efficacy (measured by GSE Scale [Schwarzer & Jerusalem, 1995]), and hope (measured by AHS [Snyder et al., 1991]).The AHS is a 12-item measure of a person's level of hope. The scale is divided into two subscales that comprise Snyder's cognitive model of hope (Snyder et al., 1991): (i) Agency (i.e., goal-directed energy) and (ii) pathways (i.e., planning to accomplish goals). Each item is measured using an four point Likert-type scale ranging from “Definitely False” [0] to “Definitely True” [4] (Snyder et al., 1991). The AHS has demonstrated reliability and validity as a tool for older adults with and without cognitive impairment (DiGasbarro et al., 2020). The GSE Scale is a self-reported measure of self-efficacy and uses a 4-point Likert-type scale ranging from “Not True at All” [0] to “Exactly True” [4]. Possible scores range from 10 to 40, with higher scores indicating greater self-efficacy (Schwarzer & Jerusalem, 1995). The GSE Scale measures a person's sense of competence for dealing effectively with a variety of stressful situations. The GSE Scale has good internal consistency with a Cronbach alpha ranging from 0.79 to 0.86 (Luszczynska et al., 2005) and has been used in studies exploring self-management in dementia (Quinn, Toms, Jones, et al., 2016). Patient-reported experience outcome measures were collected via our post-intervention survey to assess participant satisfaction (Appendix C) and feasibility to deliver the program virtually (Appendix D).
Data Analysis
Analysis of quantitative data (including analysis of the patient experience survey) involved descriptive statistics (frequencies, means, proportions) to compare patient-reported outcomes and pre-post measurements. However, limited program participation due to the COVID-19 pandemic led to a smaller than planned sample size. As such, overall trends of pre and post scores are reported descriptively only. For qualitative data, facilitators transcribed verbatim transcripts from focus groups and telephone interviews and analyzed data using content analysis (Braun & Clarke, 2012).
Results
Participant Characteristics
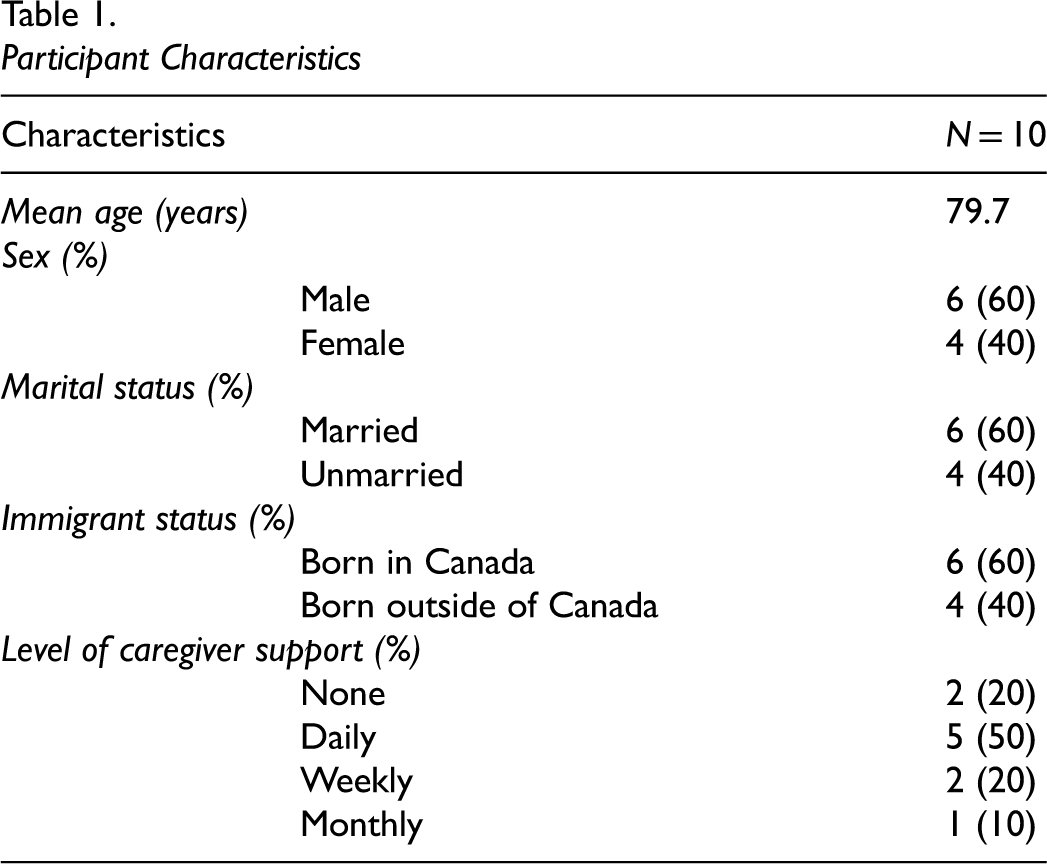
Of the 23 eligible older adults with mild-to-moderate dementia who were recruited, 20 individuals consented to participate in the study (launched in January 2020). Due to the COVID-19 pandemic, the study was placed on hold between March 2020 and August 2020. Upon study resumption, one individual died, one no longer had access to transportation, and eight withdrew consent and no longer wished to participate in-person or virtually due to personal or health related reasons related to COVID-19. Table 1 shows the characteristics of the 10 participants who took part in the CST Program intervention (mean age 79.7 years; 60% male). The majority of participants (60%) were married and born in Canada and, all were English speaking, and 50% needed daily caregiver support to manage some aspect of their ADLs.
Participant Characteristics
CST Program Participation
The 10 participants attended on average 11 of the 14 CST program sessions. Participants in Group A (n = 5) and Group B (n = 3) attended twice weekly for the initial seven sessions and then were placed on hold for 5 months due to the COVID-19 pandemic. There were two individuals from Group A (n = 5) who did not return following the COVID-19 study hold due to illness and therefore attended less than seven sessions. Upon return to complete the remaining seven sessions, the remaining participants from Group A and B combined to form Group D (n = 6) and attended twice weekly. Participants in Group C (n = 2) attended all 14 sessions without absences attending twice weekly for 7 consecutive weeks.
Quantitative Outcome Measures
Results from the GSE Scale indicated that self-efficacy increased in five participants (63%) following completion of the CST program. GSE Scale scores can range from 10–40 with higher scores indicating more self-efficacy. GSE Scale scores ranged from 21–37 preintervention and 24–40 postintervention. Pre intervention AHS scores ranged from 27–63 and 41–62 postintervention. Results from the AHS at postevaluation show that all participants reported being hopeful, (AHS score ≥40) and two participants (20%) reported having high hope (AHS score > 56).
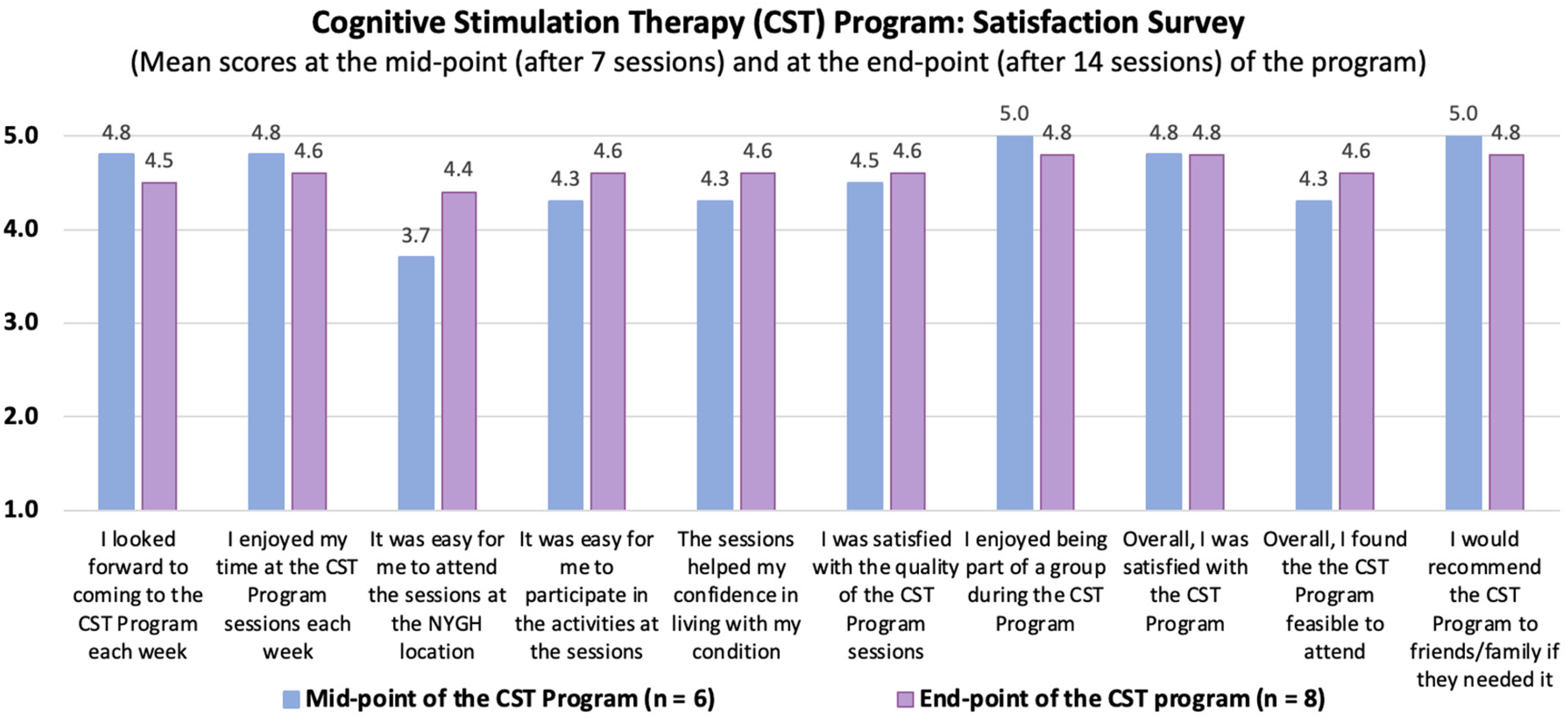
CST Satisfaction and Feasibility Survey. Figure 1 shows the mean scores for the satisfaction survey that was completed by participants at the mid-point of the CST Program (after 7 sessions) and at the end of the Program (after 14 sessions). There was an increase in scores from the mid-point (mean score range across questions 3.7–5.0) to end-point of the program (4.4–5.0) for six of the 10 questions. The highest mean scores that were consistent across the program were enjoyment of being part of a group (mean score 5.0 at mid-point; 4.8 at end-point), enjoying the program sessions (mean score 4.8 at mid-point; 4.6 at end-point) and overall satisfaction with the program (mean score 4.8 at mid- and end-points). At both evaluation points, participants only somewhat agreed that the program location was easy to attend (mean score 3.7) due to parking and construction challenges.
Satisfaction survey results.
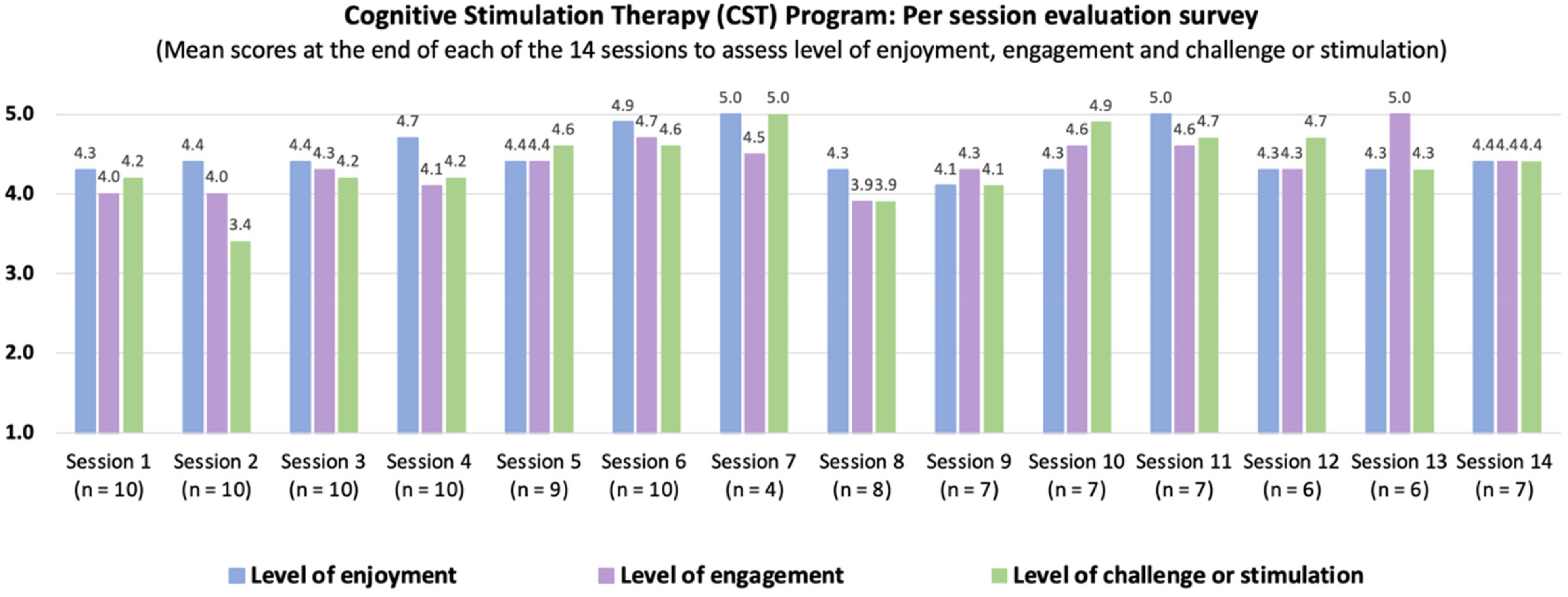
CST Program Per Session Evaluation. Figure 2 shows the mean scores for the per session evaluation survey to assess participants’ perceived level of enjoyment and engagement during the sessions and whether they perceived them to be challenging or stimulating. None of the mean scores for these three dimensions fell below the threshold to modify subsequent session activities: range of mean scores from sessions 1 to 14 for level of enjoyment (4.1–5.0), engagement (3.9–5.0) and challenge or stimulation (3.4–5.0). Overall, the highest rated program sessions across all dimensions (enjoyment, engagement, and challenging) were Session 6, which involved a “Faces and Places” activity (mean score 4.9,.4.7, 4.6, respectively); Session 7, which involved a word association exercise (mean score 5.0, 4.5, 5.0, respectively); and Session 11, which involved a “Price is Right” virtual game (mean scores 5.0, 4.6, 4.7, respectively). Lowest rated program sessions were Session 8, which involved a virtual museum tour (mean scores 4.3, 3.9, 3.9, respectively) and Session 9 involving the categorization of objects (mean scores 4.1, 4.3, 4.1, respectively).
Per session evaluation results.
Implementation Disruptions Due to the COVID-19 Pandemic
The program was implemented and delivered as per the CST manual (Spector et al., 2006). Individual session content and accompanying CST core principles are summarized in Appendix F. During the seventh session for Groups A and B, CST program implementation had to stop due to mandated public health restrictions of the COVID-19 pandemic. Given the uncertainty of when/if implementation could be resumed, we obtained telephone feedback using focus group questions (Appendix C) as well as the feasibility of implementing CST virtually (Appendix D) from six of the eight (75%) participants in Group A and B. Of the two participants who did not provide feedback, one was lost to follow up and the other was too ill to provide feedback. Results showed that five of the seven participants (71%) had access to Wi-Fi and a tablet device, but four (57%) did not feel confident in their skills to use the device. Most participants (57%) believed that delivering CST virtually could still provide some benefits, however they felt technology training would be required for success of future program participants to participate virtually if COVID-19 restrictions continued.
Results of the Qualitative Analysis
Qualitative data were collected from nine of ten participants. One participant's feedback was provided using a caregiver proxy due to illness and one participant was lost during follow up. Participants provided recommendations for future CST program participants. Overall, four general themes emerged from telephone interviews with participants and focus groups with both participants and CST program facilitators.
Theme 1: Social connectedness. Being part of a group that allowed social connection with others was a key message expressed by the program participants: Great group support, motivation, engagement, great involvement. (Person with Dementia)
These social connections provided additional psychosocial benefits that CST can offer by bringing together a group of individuals with a shared experience. Participants began to engage in communication outside of the group setting and, on several occasions, spent time after the session to socialize with their peers. One participant, who made strong bonds with other participants, strongly emphasized the importance of a return to in-person CST for the social benefits stating: It got me out of the house, people to socialize and associate with. (Person with Dementia)
Social connections were made not just between participants but also between the program facilitators and participants. The safe environment created by the facilitators to promote communication and connections between participants was noted to enhance participant experience and encourage engagement to get the full benefits of the program: Felt warm, pleasant atmosphere, comforting and valuable. (Person with Dementia)
These social bonds were clearly observed by facilitators who noted that as the participants became more comfortable with each other, their conversations and communication were enhanced across the span of the course: Clients were more talkative, opinionated, and supportive of each other towards the end of program. (Facilitator)
Participants who resumed study participation following the COVID-19 hold strongly emphasized the social benefits they received with the in-person group and their preference for an in-person over virtual delivery of the program when it was safe to do so. One participant who had experienced virtual and telephone medical care during the pandemic provided a strong statement about the possibility of participating in the CST program virtually rather than in-person: Human touch and in-person contact are essential and removing that is harmful. (Person with Dementia)
Theme 2: Knowledge Gained and Shared. Participants reported benefits to the knowledge gained about their health condition (mild-to-moderate dementia) and described strategies for self-management. In particular, participants felt that the information they received from participating in the CST program was valuable and contributed to new knowledge they had not previously had: In the group we can learn some things because everybody has different opinions. Because what you’re thinking and I’m thinking could be different. We learn something from the group, like a challenge and we learn from new people. (Person with Dementia)
Participants were also willing to share their own experiences with other participants that allowed for further translation of knowledge about dementia self-management. This supplemented educational materials provided by the facilitators. Participants were able to learn from each other, allowing them to increase their own self-confidence by sharing a tip or trick they have used with their peers. Their connection of all having lived with dementia but with different experiences allowed for ample group discussion throughout the study, which uplifted participants’ spirits and hope: Gave me ideas to improve my attitude and thinking. Also gave incentive to continue to live life, not let sickness overcome us. (Person with Dementia)
Theme 3: Tailored Implementation Adjustments. Given that individuals participating were all within the first year of dementia diagnosis, it was important for facilitators to tailor the program activities accordingly. Participants provided feedback following each session and facilitators used their clinical skills to adjust activities in real time. Using these strategies, the activities were overall well received. One participant provided the following feedback: At the beginning, it doesn't look difficult, but you try to learn counting to 10 in 5 different languages and then remembering that. If you really want to learn, you got to go back and review it and learn it for homework. Now I never really did it before although I ask that question to myself, why didn't I ever do that …. (Person with Dementia)
Participants throughout the program sessions noted a resounding positivity of activity enjoyment. One individual felt they were: One of the luckiest people to get to come and learn this stuff. (Person with Dementia)
Using the CST manual allowed a semistructured group intervention to be provided but also allowed facilitators some implementation control based on clinical expertise: It allowed us to stick to the theme and structure of the manual but the activities were tailored for the individuals we had. (Facilitator)
Facilitators having clinical skills and experience working with persons with dementia was a large success to ensure the just right challenge was achieved but also so that communication was encouraged and supported in an organic way. The facilitators felt that: Our professional expertise makes the hard moments a little easier … reacting to the changes that happen along the way and how we model the activities … facilitators have different ways of phrasing or expressing certain points to maximize engagement. (Facilitators)
Theme 4: Long-term Programing. Upon completion of the program, participants shared sentiments of enjoying the variety of activities in the CST program and wanted to see CST offered for a longer period. Participants were inquisitive about next steps and what they could do to ensure that programing is offered in the future. Many participants were eager to learn more and wanted to know future groups they could be a part of: Is it possible to have something like this more often like for the person themselves? Is it possible to have more groups that are like us? (Person with Dementia)
Discussion
The delivery of the CST program as intended was interrupted by the COVID-19 pandemic, which also significantly affected our sample size for the duration of the study. However, of those who completed the full 14-session program, attrition was minimal with attendance remaining high. In particular, participants who were put “on hold” for several months due to the COVID-19 pandemic, came back once public health restrictions and lockdowns were lifted. This was particularly encouraging, and the strong bonds that were formed among participants as well as the familiarity with the environment in which the program was delivered may explain their return to the in-person program. This is an interesting finding in comparison to the attrition of those who consented to participate but had not yet started their CST program prior to the COVID-19 pandemic. These individuals had no experience with the CST program and many of them withdrew consent for a variety of personal health reasons and concerns related to the COVID-19 pandemic (e.g., health comorbidities, vaccination status, and being uncomfortable returning to an in-person group setting or using technology to tune in from home). Despite this challenge, the pair of participants who did not withdraw consent and began their CST programing following the COVID-19 restrictions had perfect attendance completing all 14 sessions in succession.
Participants were overall satisfied with the program and the results from satisfaction and feasibility surveys supported the findings obtained from the qualitative interviews. Participants were not only satisfied with the program and would recommend it to others, but they also expressed an interest and need for ongoing programing for themselves. The social connectedness and strong bonds formed through their participation also led to another unintended consequence, exchanging personal information among participants to maintain relationships after the program. Although this was not investigated formally, participants placed high value on their social bonds formed during their CST participation, which may have been influenced by the social isolation they experienced during the COVID-19 pandemic.
At the end of the project, both CST program facilitators reported that their clinical expertise contributed to their confidence in implementation including client centered practice, activity analysis and grading of activities that have been identified as foundational skills for occupational therapy (Townsend & Polatajko, 2007). The use of client feedback forms to assess program enjoyment, engagement and whether participants find the sessions challenging also allowed the facilitators to iteratively make adjustments to session content. This ensured that the program remained client centered, included relevant and meaningful activities, and had activities graded based on participant feedback as well as clinical skills and observations. As noted by Spector et al. (2008), a CST group facilitator needs to effectively manage individual and group dynamics, provide motivation and encouragement, adapt session content and interaction style, as well as maintain sensitivity to individual and group needs. Feedback from participants indicated that facilitators demonstrated these skills and were valued as key components to the success of the CST groups in our study. All these learnings will be adapted for any future delivery of the CST Program by our group.
An unintended consequence of CST being offered within our setting was the potential for care coordination to be discussed by the occupational therapist and referring physicians. Although external study personnel had to discuss findings with referring physicians (to eliminate a conflict of interest of the occupational therapist being the CST program facilitator and researcher), knowledge of participants’ health status during the CST program facilitated a dialogue with the referring physicians, which triggered the scheduling of earlier follow ups to address critical concerns. This highlights an additional benefit to embedding a CST program within geriatric services to allow for monitoring of patient status and being able to respond in a timely manner through care coordination should critical issues arise.
Limitations
Our study had some limitations. First, many recruited participants were unable to take part in the program due to the COVID-19 pandemic. In particular, our funding for the study was only extended 3 months despite research activities being suspended for 5 months due to public health restrictions that significantly impacted study timelines. In addition, the pandemic compromised individuals' feelings of safety in terms of participating in-person due to various personal health safety considerations. Second, our study ended up with a smaller sample size than intended with a substantial lag between the first and second half of intervention delivery for a large portion of the participants. Future research should include a larger sample size of participants receiving the intervention in its intended 7 consecutive-week succession to determine if our findings can be replicated in practice. Third, we were not able to apply the Kohlman Evaluation of Living Skills (KELS) instrument as an outcome measure as intended due to the COVID-19 pandemic. Lastly, data collected on the impact of CST on self-efficacy and hope cannot be conclusive given the small sample size and the inability to account for external factors (i.e., social isolation and public health restrictions) that may have contributed to participants’ circumstances during the unprecedented times of the COVID-19 pandemic.
Future Research
Results from this report highlight a need for future research to test the CST Program rigorously and explore its applicability across a range of settings. As the population of those living with dementia continues to grow in Ontario, the government has prioritized for those with dementia to live well and be supported by appropriate services where and when they need them (Ontario Dementia Strategy Consultation, 2016). Further research into the implementation, scaling, and economic feasibility of delivering CST would provide the Ontario Ministry of Health with the necessary data to incorporate such a program into the Dementia Strategy. Although the COVID-19 pandemic study interruption impacted the collection of pre- and postfunctional outcome measures in this study, prior studies have demonstrated a positive impact of CST on quality of life, relationships with significant others, energy levels, and ability to perform chores (Chapman et al., 2004). Functional outcome measures including ADLs and instrumental ADLs (IADLs) should be a future research priority with respect to occupational therapist-led CST implementation since their foundational skills position them well to have an impact on the physical and cognitive functioning of people living with dementia (Launhardt et al., 2010; Yuill & Hollis, 2011). Possible outcome measures for use in a future trial should include the KELS instrument (Thompson & Robnett, 2016) to provide a functional outcome measure of ADL/IADL performance; along with the Amsterdam IADL Questionnaire to provide a caregiver insight into functional abilities (Sikkes et al., 2013). In addition, given the shift of health care delivery during the pandemic to virtual care, policymakers may see a need for future research to explore virtual CST implementation to determine if it provides the same benefits as in-person. The implementation of virtual CST may eliminate physical barriers to accessing in-person care; however, it may not be feasible or appropriate for this population given the skills required for use of technology, access to technology, and caregiver involvement.
Conclusion
Prior research has demonstrated an evidence base for the use of CST for individuals with mild to moderate dementia to maintain cognitive functioning irrespective of drug therapies. Occupational therapists are a well-positioned regulated health profession to implement CST programs and may be useful in supporting the dissemination and scaling of these programs within health care settings. Despite recognition globally and local training opportunities for Canadian occupational therapists, CST has not previously been formally implemented within the Ontario health care setting. The results of our qualitative findings suggest that both participants and CST Program facilitators found the program to be feasible despite implementation challenges due to the COVID-19 pandemic and valued by older adults with mild-to-moderate dementia. In particular, our OT-led CST Program was successfully delivered for individuals with varying levels of cognitive abilities, and our iterative evaluation of the program also facilitated program engagement, enjoyment, and social connections. This was reflected in both our quantitative and qualitative data. Despite our positive findings, due to the challenges related to the COVID-19 pandemic and our study limitations, further research is needed to rigorously examine CST as a feasible option for implementation by an occupational therapist in the Ontario health care system.
Key Messages
An occupational therapist-led CST Program was feasible to implement in a specialized geriatric clinic setting for community-dwelling seniors with mild-to-moderate dementia.
Ontario's dementia strategy focuses on providing evidence-based support and services to individuals aging at home, of which CST may be an appropriate intervention to support this population.
Future research is needed with larger sample size, to more rigorously test the potential of an occupational therapist-led implementation of the CST Program including its applicability in a range of settings.
Supplemental Material
sj-docx-1-cjo-10.1177_00084174221115284 - Supplemental material for Occupational Therapist Led Cognitive Stimulation Therapy: Feasibility of Implementation
Supplemental material, sj-docx-1-cjo-10.1177_00084174221115284 for Occupational Therapist Led Cognitive Stimulation Therapy: Feasibility of Implementation by Kristin Collins, Madona Hanna, Julie Makarski, and Monika Kastner in Canadian Journal of Occupational Therapy
Footnotes
Acknowledgments
The primary author wishes to acknowledge the participants of the study and thank them for their time and commitment. The facilitator and primary author's experience of program implementation has previously been shared at the Centre for Aging and Brain Health Innovation Summit in March 2021.
Declaration of Conflicting Interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and or publication of this article. This work was supported by the Centre for Aging and Brain Health Innovation SPARK Grant [|SPARK-4-00262, 2019] and the North York General Hospital Exploration Fund [2019].
Ethical Approval
Research and Ethics Board approval was obtained from North York General Hospital in Toronto, Ontario, Canada.
Informed Consent
All participants provided written informed consent to participate in the study.
Supplemental material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.