
Abstract
Introduction
Home modifications are environmental interventions to support performance, safety, and engagement in everyday activities (Canadian Association of Occupational Therapists, 2016). Evidence indicates home modifications are beneficial for people and offer both individual and social benefits for people choosing to age in place. At an individual level, home modifications can reduce fall risks at home (Carnemolla & Bridge, 2020; Somerville et al., 2016; Stark et al., 2017, 2018), decrease an individual's fear of falling (Chase et al., 2012; Gitlin et al., 2006), and decrease difficulty performing everyday tasks (Carnemolla & Bridge, 2020; Petersson et al., 2009; Somerville & Stark, 2015). Since people have strong connections to their homes (Vrkljan et al., 2011), implementing home modifications that facilitate people to safely remain at home can strengthen their personal and social meaning of home (Tanner et al., 2008).
In general, the World Federation of Occupational Therapists describes sustainability as the ability of humans to live and thrive without threatening the well-being of future generations’ ability to live and thrive (World Federation of Occupational Therapist, 2018). More specifically, sustainability occurs at the intersection of three pillars: economic, social, and environmental (Hussain et al., 2018).
The economic aspect of sustainability refers to the need for adequate financial resources to meet the needs at the individual, community, and institutional level (Vergunst et al., 2020), such as the financial costs involved in purchasing adaptive equipment, modifying a home, or moving to a more accessible home. Challenges in supporting aging in place have been identified because of inadequate funding (Zhou et al., 2020), especially for older adults (Samuel et al., 2019) despite evidence that supports potential sustainability for the overall system if funding is considered. For example, an American study found home modification programs were cost-effective compared to pharmacologic and other medical therapies and facilitated older individuals to remain safely at home (Jutkowitz et al., 2011). Another study conducted in the United Kingdom found that home modifications can result in significant cost savings if completed in a way that prevent hospitalizations or expedite discharges (Curtis & Beecham, 2018).
Social sustainability is concerned with the human aspects of sustainability such as quality of life and socially driven decision making (Hussain et al., 2018). This links system-level decision makers to considerations that everyone has the opportunity to live a full life including all aspects of their health. This line of thinking also indicates social sustainability is a key objective in health care. Both, individual and systemic social barriers to social sustainability exist. The individual barriers include challenges in navigating the system (Johansson et al., 2009; Mackintosh, 2020) and that having to move homes may be stigmatizing (Shaw et al., 2018; Struckmeyer et al., 2022). Social systems issues typically surround policies that act as barriers to access to home modifications such as application procedures and acceptance criteria or a focus on providing funding for health care support vs. environmental modifications. Studies highlight the connections between social outcomes and financially related policies (Zhou et al., 2020; Slaug et al., 2017). Appropriate funding of basic home modifications can decrease the need for home services (Slaug et al., 2017). The completion of home modifications has direct implications on social aspects of health including reductions of caregiving and caregiver burden (Carnemolla & Bridge, 2019; Stark et al., 2017) and improved social and community participation (Carnemolla & Bridge, 2020; Petersson et al., 2009; Somerville & Stark, 2015). While these effects are understood, it is unclear if occupational therapists intentionally consider these concepts in their clinical process.
The environmental pillar focuses on maintaining a balance between consuming and replenishing natural resources (Vergunst et al., 2020). The built environment is highly carbon intensive (Hayles and Dean, 2015) and, while there are policy actions around reducing CO2 emissions related to the built environment, it is opined that human behaviour is key to reducing society's reliance on carbon (Pilkington et al., 2011). Additionally, construction and its waste, abandoned equipment, and a lack of existing accessible housing (i.e., requiring new builds) in general all have environmental implications.
The concepts of health and sustainability are viewed as compatible but there needs to be better collaboration and coordination between experts in sustainability and health professionals to strategically build plans that will link sustainability related actions with health outcomes (Guidotti, 2018). Specific to OT, the World Federation of Occupational Therapist (2018) outlines guiding principles for sustainability in occupational therapy practice in general. They outline a need for an in-depth discussion of what sustainability means for occupational therapy. More specific to Canadian OT, the Canadian Association of Occupational Therapists has declared that mobilizing strategic partners for equitable, sustainable, and accessible health and social systems is a strategic priority for the next three years (CAOT, 2023). The benefits of learning more about how sustainability is considered and applied in occupational therapy in Canada may help fill gaps in the system that are limiting best practices to support sustainability. Home modifications are an area of practice with clear links across and at the intersections of all three pillars of sustainability. In order to enter into prioritized, in-depth, and interdisciplinary collaborative discussions, there is a need to understand where OTs are starting from with their perceptions of sustainability in practice. This study is an exploratory study to work toward a better understanding of occupational therapists’ perceptions of sustainability in relation to their practice in home modifications.
Methods
Study Design
This study adopted a qualitative description approach (Nowell et al., 2017) and used semistructured interviews as the primary means of data collection (Sandelowski, 2000, 2010). This study was approved by the Behavioural Research Ethics Board at the University of British Columbia and is reported here according to COREQ guidelines (Tong et al., 2007). This design was established prior to recruitment.
Participants
To be included in the study, participants needed to be licensed occupational therapists aged 19 or over, currently practicing in Canada, English speaking, consent to live audio recording and live transcript on Zoom, and have two or more years of experience in home modifications. Participants were recruited from the professional networks of the research team via word of mouth and email using convenience sampling.
Data Collection
Written and verbal consent for the study was obtained by all participants prior to data collection. Ten participants were interviewed by two Masters of Occupational Therapy student coinvestigators (second and third authors) under the supervision of a research team with extensive research experience (first and fourth authors). The first author is also a practicing OT with clinical practice in the area of home modifications. Participants completed a Qualtrics online survey prior to the interview to provide demographic information about their experience in home modifications
Data Analysis
Data collection was concurrent with ongoing analysis. Data from the first three transcripts were initially independently coded by the second and third authors/interviewers and then compiled to create a list of initial codes. The codes were reviewed by the research team to develop a preliminary consensus-based coding guide. The coding guide was updated as needed throughout the coding process in order to capture new perspectives that emerged. The research team identified the final themes based on the final coding guide (Nowell et al., 2017).
The primary trustworthiness strategies used were reflexivity and triangulation of interviewers. In terms of reflexivity, the interviewers considered their positioning and used research diaries to reflect on their activities, thoughts, and feelings throughout the research process (Bloor & Wood, 2006). The interviewers were female, Caucasian Canadian occupational therapy master's students between the ages of 25 and 35 years old. They did not have any prior experience working in home modifications, therefore, their understanding of the perspectives of the sustainability of home modifications was limited. The first author was a female Caucasian occupational therapist with 14 years of community-based practice including home modifications, and an interest in determining the personal and social value of home modifications in supporting people to live in the place they choose. The last author was a male Caucasian occupational therapist/researcher with over 30 years’ experience and a deep concern about the environmental impacts of climate change.
Prior to conducting the interviews, the interviewers documented how they believed the participants would respond to the interview questions. In terms of their preexisting assumptions, the interviewers believed that affordability would be a barrier to clients accepting home modifications and that navigating the funding system was challenging. In addition, they believed that participants would discuss how home modifications would allow their clients to remain within their own communities and maintain social connections. To mitigate these assumptions, the researchers approached the interviews from the perspective of learners and students, to encourage candid responses from participants. The second author had a preexisting professional relationship with one participant, and the third author had a preexisting professional relationship with one different participant. Since the interviewers were students, they had no actual or perceived professional power over any of the participants. The interviewers participated in all interviews and the entire research team participated in the data analysis process. The researchers do not believe they reached data saturation due to the heterogeneity of participants and the relatively small sample. Recruitment was stopped at ten participants due to time constraints; however, there was a repetition of concepts in the last few interviews; which is assumed to suggest adequate sampling for an exploratory study.
Findings
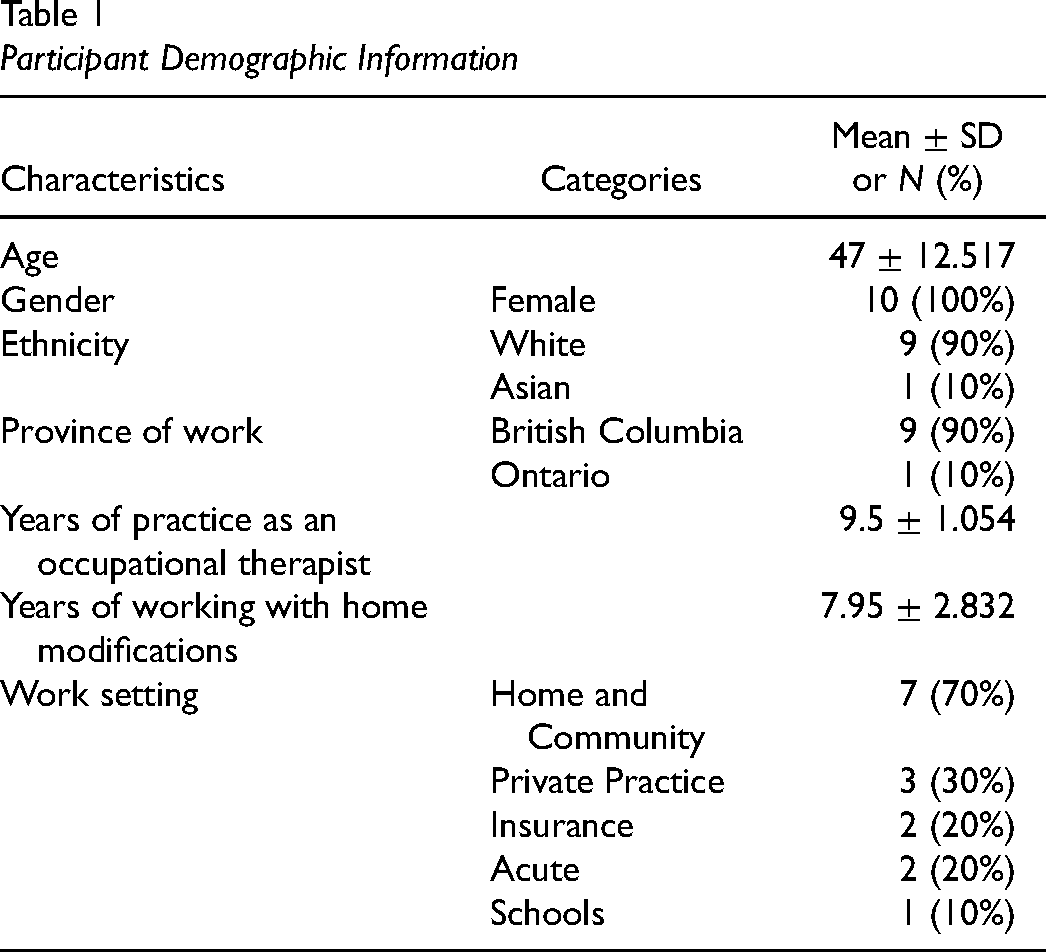
Demographic information for the sample is summarized in Table 1. Through our data analysis, we developed three themes. The first, “It's not easy being green: environmental sustainability” described the uncertainty and lack of direction occupational therapists experienced regarding the environmental considerations of home modifications. The second theme, “Stretching a dollar: financial inequities,” described inequities that exist within the funding system, and the third theme, “Barriers and
Participant Demographic Information
Theme 1: It's Not Easy Being Green: Environmental Sustainability
This theme revealed therapists’ perceptions of balance between consuming and replenishing resources when working with home modifications. Participants indicated they were aware of environmental considerations, but felt it was not something they were able to implement in practice. Leanne, who was between the ages of 46–55, said, “I think it's an area where we can really work on,” and expanded by saying, “There's awareness, but I think the problem is, it's […] general society today, not looking at how we could be more sustainable.”
A few participants indicated that function and safety were key considerations when prescribing home modifications and the principles of reducing, reusing, and recycling were not prioritized. They reported they were aware of informal options for clients to sell their equipment through online platforms, which would allow for it to be reused. When recommending these platforms, participants emphasized the need for clients to be aware of potential safety issues. Hannah, who was between the ages of 46 and 55, expressed her frustration regarding a lack of recycling programs available through her employer, saying “I’m more frustrated with the amount of plastic and the amount of metal that we're producing to provide these aids.” Many participants indicated that the health authorities within which they worked did not have a suitable program for recycling equipment that was no longer being used by clients. Oftentimes, a client would only need the equipment for a short duration, and it was in good working order at the end of its use. Hannah identified challenges that people had when donating used equipment: [When the] Ministry pays for it, [if] client dies […] two months later, like it's perfectly useful. And I got to find a home [for the equipment]. The other option for the building is to put it in the lane and someone will take it for scrap metal, but the building shouldn't be reinstalling it themselves because they don't have the training to reinstall something.
A couple of participants explained how their clients’ preferences for new or used equipment were a factor in how the environmental component played out in their everyday practice. Monica, who was between the ages of 36 and 45, and Kristina, who was 66 or over, indicated that some of their clients had an aversion to using secondhand equipment, and would prefer to purchase new equipment instead.
The Red Cross and local loan cupboards were identified as possible means of having a sustainable practice. Through these programs equipment could reenter the healthcare system after the original owner no longer required the item. However, access to these programs varied based on location and type of home modification. Paula, who was between the ages of 46–55, mentioned that clients often came to her stating that they no longer required the equipment they had purchased. She then would refer them back to the Red Cross and inform them that it may be able to be recirculated through the program if it were in relatively new condition and was deemed safe.
Theme 2: Stretching a Dollar: Financial Inequities
The second theme, “Stretching a dollar: financial inequities,” revealed the funding inequities that existed with home modifications. Participants described different experiences clients with and without personal funds had. Affluent clients could afford most home modifications they needed and could make home modification choices based on aesthetics without an apparent regard for basic concepts related to sustainability. Morgan, who was between the ages of 56 and 65, stated, “I have people who are phenomenally wealthy who can create a home […] I have students [as clients] who have beautiful elevators in their home with wood panelling, […] out of a magazine kind of level.” Leanne echoed this experience when she was sourcing a lift recline chair for a client, but the client did not like how it looked. Leanne explained, “So he ended up making a $2000 donation to the ALS program and said, ‘Thank you very much. I don’t need your equipment.’ And then bought himself a leather [lift recline chair].”
In contrast, funding and navigating the funding system was the biggest barrier to home modifications for clients with limited financial means. Paula illustrated this when she said, “economic factors could be insurmountable for many people.” The participants described how clients did not know all the available funding options, and that helping them navigate and piece together sufficient funding took a lot of time and energy. The participants felt this was part of their role, but as Leanne described, “there's only so much you can do and I have 40, 50 other clients that I need to see.”
Sometimes, the funding still did not cover everything. Hannah described how there is no funding for installing grab bars and explained that “we have to approach our managers to pay for [it] […] for people who really need it.” Theresa described feeling “constrained” when seeking funding for her clients, and attributed this to her belief that the public funding system was only interested in providing safety-related accessibility. This was exemplified by Leanne's story of a 40-year-old client who was denied funding to add railings and widen the stairs leading into her house, which would have allowed her to independently engage in the community. Without the funding that would have allowed this client to be mobile and active, Leanne explained: She ended up […] having a pressure wound that was quite significant and she ended up […] in a care facility. And then they worked really hard to get her out of the care facility because she shouldn't be there, but […] she just couldn't manage [her wound].
The participants described how home modifications were delayed both by the time it took to find funding, as well as the time it took to receive them. Long wait times for home modifications often meant people were unable to participate in basic self-care activities, which could also result in a loss of dignity. This was illustrated by Charlotte's example of a client who was using a hose in the backyard to shower because he was unable to access his bathroom. Making do with alternative solutions to occupational therapy recommended home modifications, whether due to a lack of funding or waiting for the funding to be approved, was often perceived as unsafe. For example, due to financial limitations, one of Morgan's clients used a piece of plywood as a ramp. She described feeling concerned about the safety of the family and others using it, as well as the liability risk it brought for the family.
A few participants believed that paying more for future-proofed home modifications could save both the healthcare system and clients’ money long term. Morgan shared a story that illustrated both the benefits and financial savings that a well thought out home modification provided for a family involving aging parents and a son with a physical disability. With a combination of personal funds and grants, the family built a fully accessible home with a suite attached so the son could have his independence as he got older, and the parents could age in place as long as possible. Morgan recounted what happened later when the husband moved into a care facility: The family struggled financially and what they were able to do was rent out the suite. And [the son] moved into […] the other part of the home with his mother, but because they built it already fully accessible he could make that transition very smoothly. And, they generated some income from having this suite […] as an accessible solution. […] And […] if that hadn’t happened, […] when the dad moved into a care home and the cost of keeping him there was so expensive. He could have almost bankrupted them, paying for his fees. So, it kept that family together […] because the built environment allows them to do that.
Theme Three: Barriers and Benefits in the Process of Home Modifications
The third theme, barriers and benefits in the process of home modifications, described the disparities in the process of home modifications. It is divided into three subthemes: barriers to completing home modifications, creativity in rural communities, and aging in place. The first subtheme, barriers to completing home modifications discusses challenges that participants encountered during the process. Participants reported that navigating home modifications was complex due to system constraints and differing regional policies. For example, the need to obtain permission from landlords could prevent home modifications from going ahead. Morgan spoke to this challenge: “if people are living in rented accommodation that adds a whole other layer of complexity because you need a landlord's approval and often it can't be anything that's permanent.” Charlotte further explained the process of getting a landlord's permission in the context of social housing: If it's a rental, you’ll need to get landlord permission, so usually I would seek that before we even make recommendations for the modification because if we can get equipment it's usually preferred by landlords. And if it's social housing, […] You have to get the permission from the social housing corporation to do any modifications.
Participants reported that the resale value of the home and the general cost was considerations for clients. Monica spoke to this with regard to aging in place: “[Clients] want to spend as little as possible. They don't want to modify their home because […] what's it going to do to resale?.” Other participants brought up concerns regarding the home being structurally sound enough to complete home modifications. Courtney stated concerns about a client living in inadequate conditions on a reserve, which was complicated by his social circumstances. She shared what she found during her home assessment: the floor was coming through on the shower into the basement and I couldn’t go into the basement because they had infestations of rats and other things down there so basically I just left really not making any recommendations. And that was a struggle because I couldn’t justify having to put in a new bathroom in a house that for one, the [owner]was partially responsible for and […] they didn’t have the money to fix it […] So it was a challenging one in which I kind of left saying [he] continues to live at his own risk and I don't think that I can recommend anything specific. He needs a new shower, but he needs a new floor, and he needs a new house.
The second subtheme, creativity in rural communities, explored the unique complexities that therapists who worked in a rural setting encountered. Alex described how having limited options in rural areas necessitated clients to find workarounds when home modifications were not easily accessible due to their geographical location. She stated that low-tech home modifications were often preferred in rural communities and described the sense of community that existed: …people who live in these rural areas […] have this great sense of community, […] everyone comes together and comes up with a solution like it's not very often [one would] go to a community like that and their favourite coffee store has […] already made a ramp for them to get in and out. […] they just kind of come together and take that on as a community which is really cool.
Alex spoke about the positive qualities that she viewed rural communities to possess: “A lot of rural areas [are] very resilient and creative.” She wanted to incorporate these qualities into her urban practice as well.
The third subtheme, aging in place, described the meaning of being able to stay at home with advancing years, or after a significant injury/illness, and how home modifications allowed clients to stay involved in their daily routines and in their communities. Many participants emphasized that when prescribed successfully, home modifications allowed clients to remain at home by increasing accessibility, improving safety, reducing caregiver burden, and allowing clients to reengage with their activities of daily living. Monica stated: One of the arguments, […] that I make for a well-designed environment, including a modified home, is that I say that it's a silent care partner who never gets sick who […] you don’t have to pay them overtime, because your home works for you, rather than against you.[…] And it allows you to maintain your sense of self and to be interdependent on caregivers, should that be necessary, rather than totally dependent.
Discussion
The findings of this study provide an initial understanding of occupational therapists’ perspectives on the sustainability of home modifications in primarily British Columbia. Three themes illustrate the ways in which the economic, social, and environmental pillars of sustainability interact with each other in home modifications practice. Constraints and uncertainties around environmental considerations, financial inequities in funding systems, and the numerous challenges limiting effective home modifications are highlighted.
Findings from this study suggest that occupational therapists are less certain about the environmental sustainability aspect of implementing home modifications than they are in equipment provision. In fact, their application of the concepts of sustainability focuses primarily on environmental aspects related to equipment (e.g., equipment loan programs). This shows participants consider the importance of potential environmental outcomes of their recommendations but not as much how their broader home modifications practice is impacted and can influence sustainability. This focus could be related to how the system, specifically the financial pillar, imposes barriers on access to higher level sustainable practices such as home modifications. This can limit OTs to the provision of equipment in this area of practice which can limit their consideration of broader sustainability concepts in their practice.
In relation to the pillar of economic sustainability, the findings in this study suggest a public system priority on safety which implies a focus on preventing additional health spending (i.e., avoiding use of the high-cost acute care system). Participants in this study demonstrate a sense of awareness of this pressure in their practice. They also highlight the differences in the degree of home modifications that can be provided depending on the funding source and / or policies behind the funding. Spending appropriately based on health professional recommendations appears to demonstrate financial benefits and sustainability according to the study by Curtis and Beecham (2018). Further detailed cost analysis research is warranted to support sustainable public health funding policy. Specifically, the safety issues not addressed with appropriate modifications or adaptations (including adaptive equipment) or lack of access in general can have negative health outcomes as outlined by Charlotte's and Linda's examples.
It is difficult to comment on the implications of the social pillar on its own without considering the interplay with the financial pillar. Without access to funds, individuals must rely on a fragmented system that places them in a further disadvantage and sometimes fails them by denying them appropriate home modifications. This negative feedback loop is especially evident among those living on reserves, where 43 per cent of homes are in need of major repairs (Statistics Canada, 2017) without considering home modifications for accessibility. These intersectional effects between the social and financial pillars of sustainability illustrate the need for equity focused funding support for home modifications. With adequate funding, home modifications can reduce individual and societal costs (Slaug et al., 2017; Jutkowitz et al., 2011).
More specifically related to the social pillar of sustainability, participants identified contextual challenges that can limit clinical reasoning. For example, obtaining permissions from landlords and strata may act as a deterrent to completing a home modification in a sustainable manner. Challenges in rural communities were previously identified in research pertaining to community access, even when home modifications were installed (Thordardottir et al., 2020). Participants in this study outlined similar challenges but highlighted the unique sense of community and resilience that comes when clients from rural areas are forced to be creative when home modifications are not readily available.
This study is limited by having a small sample size that is fairly homogeneous. The focus for this exploratory study was within Canada and ultimately ended up primarily a study of perceptions of British Columbian occupational therapists because of sampling. All of the participants identified as female, and all but one participant identified as white. Many participants had more experience completing home modifications involving equipment rather than renovations, thus the results may speak better to the sustainability of the former.
Conclusion
This study explored occupational therapists’ perspectives on home modifications pertaining to the three pillars of sustainability: economic, social, and environmental. Building an understanding of sustainability in practice is important to enable occupational therapy to join the action needed to support planetary health. While there is research on the economic and social pillars of sustainability, little exists on the environmental pillar. This study contributed toward filling this gap by confirming the uncertainty and lack of awareness occupational therapists experience regarding sustainability as a broad concept in home modifications. We found occupational therapists are interested in taking environmentally friendly approaches in their home modification practice but currently find it challenging due to system constraints.
This study suggests the importance of improved policies and guidelines regarding sustainable home modification practices, including more equitable access to funding sources. The findings could be used to inform guidelines to foster occupational therapists’ clinical reasoning to consider the interplay of all three sustainability pillars in home modification practice. Future studies to further understand the views and practice of Canadian Occupational Therapists are warranted based on the initial themes found in this study. Preliminary findings of unique considerations regarding perceptions of sustainability in rural settings justify the need for further research in this specific aspect of home modification practice. Cost analysis studies that review the hidden costs and set benchmark values of providing home adaptations such as the study completed by Curtis and Beecham (2018) would also be a valuable addition to the Canadian literature.
Key Messages
Occupational therapists would like to implement more environmentally friendly and overall sustainable approaches when it comes to home modifications but may be limited by the social and financial systems.
The funding system for home modifications in Canada needs to be improved to become more equitable for the public.
Further research in understanding sustainability in OT practice is needed.
Footnotes
Acknowledgements
The authors would like to acknowledge the time and expertise provided to our team and this study by each of the participants.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.