
Abstract
Background.
Lifestyle Redesign® occupational therapy (LR-OT) originated in the Well Elderly studies as a preventive intervention for older adults, demonstrating positive health and cost outcomes. Although LR-OT later expanded to chronic condition management and inspired numerous programme adaptations for different contexts and populations, systematic reporting of intervention modifications remains scarce. This gap extends beyond OT, reflecting a broader movement in implementation science.
Purpose.
This study applies the Framework for Reporting Adaptations and Modifications-Expanded (FRAME) to systematically document adaptations across four LR-OT programmes. Additionally, we examine fidelity-consistency by mapping programme components to the Well Elderly programme and core LR-OT elements.
Introduction
Adaptation of Evidence-Based Programmes and Practices
Research documents a growing interest in the science and methods of adapting evidence-based programmes and practices (EBPs) for implementation in new contexts (Escoffery et al., 2019; Stirman et al., 2019). Adaptation is the process of making changes, planned or unplanned, to an intervention or programme design (e.g., content, dosage, procedure) to fit the needs of a population or context (Stirman et al., 2013). Modifying interventions can improve acceptability and outcomes for a target population and address healthcare inequities that limit accessibility and effectiveness of interventions in underresourced communities (Chambers et al., 2013). In contrast, failing to adapt interventions ignores the critical influence that context has on the success and sustainability of intervention implementation.
Although adaptation is foundational to the translation of EBPs, ensuring that adapted interventions simultaneously remain true to the core components of the original intervention framework is vital (Stirman et al., 2019), as altering essential elements of an EBP may compromise its effectiveness and ability to meet population needs (Pérez et al., 2016). Mejia et al. (2017) note that a “both-and” approach is possible, such that one can both adapt an intervention to ensure cultural relevance and maintain fidelity to its original framework. Thus, although adaptation is critical to ensure contextual relevance and equity, fidelity to an intervention's core elements anchors its effectiveness. This dynamic interplay between fidelity and adaptation frames the present analysis of Lifestyle Redesign® Occupational Therapy (LR-OT).
There is a dearth of systematic documentation of adaptations made to EBPs. This leads to difficulties in determining the effectiveness of adaptations, replicating resultant modifications, and anticipating the impact of future adaptations based on new contexts, populations, and resources (Mejia et al., 2017). Clearly specifying and evaluating adaptations enhances an intervention's external validity across contexts and facilitates its potential for routine implementation (Baumann et al., 2017).
To address these issues, the Framework for Reporting Adaptations and Modifications-Enhanced (FRAME) offers a structured, comprehensive approach to systematically documenting modifications to EBPs (Stirman et al., 2019). Unfortunately, systematic reporting of intervention adaptations is scarce in the occupational therapy (OT) literature. Only one OT team to-date has used FRAME to report adaptations to an evidence-based OT intervention (Piller et al., 2021). Piller's group posits that this gap in reporting stems from the client-centred, individualized nature of OT interventions, which rarely follow scripted, step-by-step processes, thereby hindering documentation of concrete adaptations.
Lifestyle Redesign® Occupational Therapy
LR-OT, an empirically supported approach to OT intervention, presents an opportune case to explore adaptations of client-centred OT EBPs. LR-OT has been continuously adapted to meet the evolving needs of diverse target populations and contexts (Pyatak et al., 2022). Originally developed at the University of Southern California through the Well Elderly (WE) studies, LR-OT was initially designed as a preventive intervention for well older adults 1 (Clark et al., 1997). The effectiveness and cost-effectiveness of LR-OT in improving the health and well-being of older people was established in two large-scale randomized controlled trials (Clark et al., 1997, 2012). The programmatic structure of WE LR-OT has been described elsewhere (Clark et al., 2015; Jackson et al., 1998), but is summarized in Table 1 and expanded upon in Supplemental Table 1.
Comparison of Adapted Lifestyle Redesign® Programmes to the Original Well Elderly Programme Structure.

Note: AOTA = American Occupational Therapy Association; DFU(s) = diabetic foot ulcer(s); HIPAA = Health Insurance Portability and Accountability Act; LR = Lifestyle Redesign; OT = occupational therapy/ist; WE = Well Elderly.
Refer to Supplemental Table 1 for expanded details on the Well Elderly programme structure.
The foundation of LR-OT lies in its core elements, illustrated in Figure 1, which provide a framework for fidelity while supporting flexible adaptation. Core characteristics (i.e., focusing on daily activity orchestration, applicability to lifestyle challenges, collaborative therapist–client process with individualization, health-relevant outcomes, and delivery by trained OT practitioners) distinguish LR-OT from other approaches (Pyatak et al., 2022). These characteristics are operationalized through core domains (i.e., meaningful occupations, habits, and routines; chronic condition management; psychological well-being; environment and context; and advocacy and healthcare access) that guide intervention content. Practitioners employ core techniques (i.e., patient education, occupational self-analysis, narrative reasoning, problem solving, and autonomy-enhancing communication) that shape therapeutic processes. Together, these characteristics, domains, and techniques form an integrated fidelity framework that both grounds adaptation and supports individualized implementation.
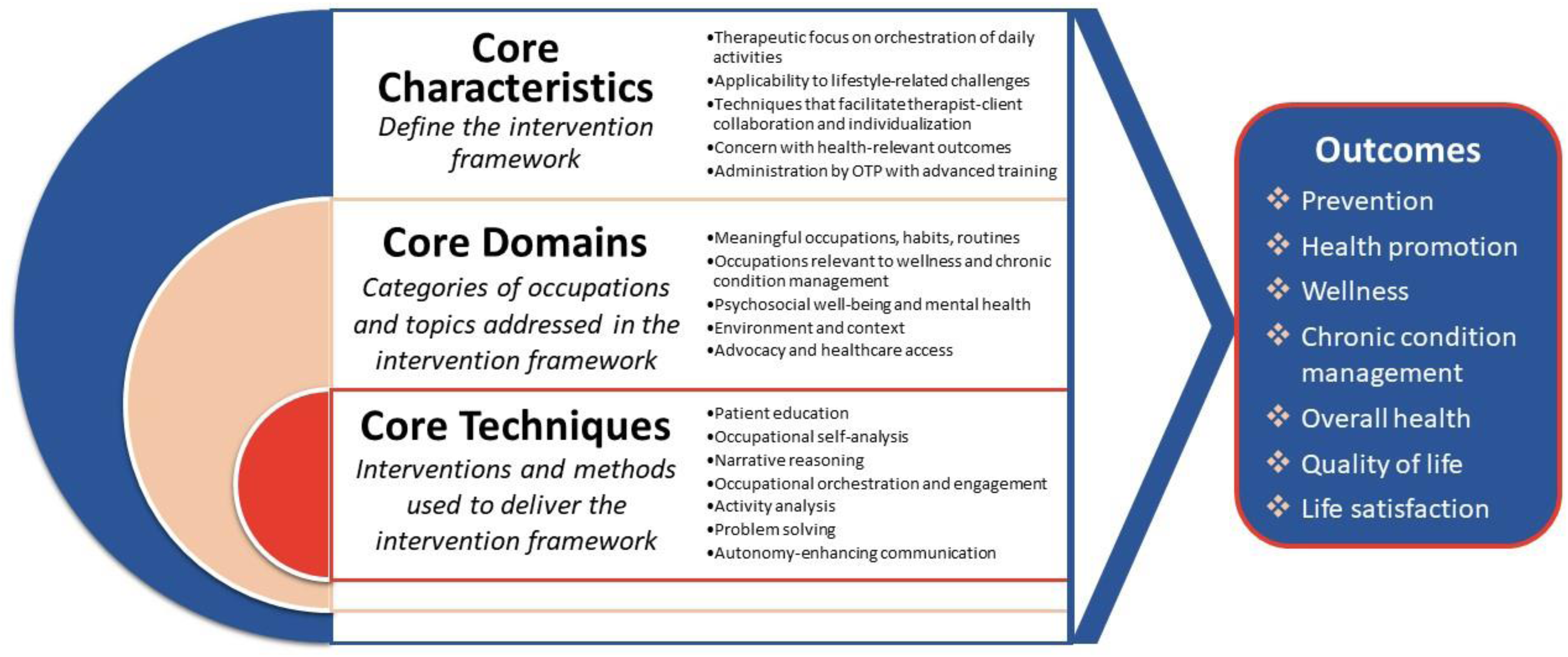
Core Elements of the Lifestyle Redesign® Occupational Therapy Intervention Framework.
Study Purpose
The purpose of this paper is to apply FRAME to characterize adaptations made to four distinct case examples of adapted LR-OT programmes. These four cases were selected because they reflect diverse adaptations across populations, settings, and delivery models, offering a unique opportunity to systematically document adaptation processes. Together, they illustrate how LR-OT has been translated in research and practice and highlight the balance between adaptation and fidelity across varied contexts. Secondarily, we examine the fidelity-consistency of these interventions by mapping their components to the structure of the original WE EBP and core elements of the overarching LR-OT framework. By analysing these cases, we offer insights into how evidence-based OT interventions can be responsibly adapted while maintaining fidelity, thereby expanding representation of OT EBPs in the implementation science literature.
Method
Adapted LR-OT Case Examples: Programme Descriptions
This paper examines four adapted LR-OT implementation efforts, representing different populations, settings, and stages of implementation. Two of these efforts have been fully implemented and two are currently in a pilot phase. General descriptions of each programme, along with the adaptation processes employed, are included below and are referred to by their abbreviated names throughout this paper: Diabetic Foot Ulcer Self-management (DFU-SM) programme, Remodeler sa Vie (RV), Primary Care Chronic Condition Management (PC-CCM) programme, and Lifestyle Redesign® for Weight Management (WM). Programme/study details are summarized in Table 1, allowing for direct comparison to the original structure of the LR-OT WE programme (Supplemental Table 1). Terminology referring to participants varies intentionally by programme context: participants in clinical settings (PC-CCM and DFU-SM) are referred to as “patients,” participants in the private practice intervention (WM) as “clients,” and participants in the community-based programme (RV) as “older adults” or “individuals.” This distinction reflects the relationship of the participants to the intervention.
Diabetic Foot Ulcer Self-Management (DFU-SM) programme
In an ongoing pilot study, an LR-OT outpatient programme is being developed for patients with diabetes who are managing diabetic foot ulcers (DFUs) and prescribed offloading treatment (i.e., physician-prescribed devices or techniques to relieve pressure on the ulcer and promote healing; Chapman et al., forthcoming). The programme supports lifestyle changes that will improve wound healing and overall quality of life. The programme's primary long-term goal is to promote limb preservation in patients at high risk for lower-extremity amputation.
Primary Care Chronic Condition Management (PC-CCM) programme
This programme delivers LR-OT to underresourced patients with diabetes and/or hypertension receiving primary care at a single clinic within a safety-net medical centre (Pyatak et al., 2019). The overall goal of PC-CCM is to improve occupational performance, clinical outcomes, and healthcare utilization. The current model is implemented by newly licensed OT practitioners as part of their OT residency training at the clinic.
Remodeler sa Vie (Reshape Your Life; RV)
Modelled closely after the WE programme, RV has been culturally adapted for French-Canadian older adults, focusing on late-life well-being and health self-management in a Canadian (Québec) context (Levasseur et al., 2022). Delivered by a trained OT in a community setting, this 6-month programme empowers participants to develop healthy routines and engage in meaningful activities. The intervention follows 12 French-translated and culturally adapted modules developed from the English WE manual (Clark et al., 2015) to guide goal-setting in areas such as physical, social, and spiritual health.
Lifestyle Redesign® for weight management (WM)
This LR-OT programme is delivered in a private practice setting to help clients achieve and maintain a healthy weight through personalized, sustainable lifestyle changes (USC Chan Division of Occupational Science and Occupational Therapy, n.d.-b). The objective is to promote long-term health and well-being by addressing clients’ unique needs and goals. Services are offered individually in-person or via telehealth, with flexible content and duration.
Programme Adaptation Documentation and Analysis
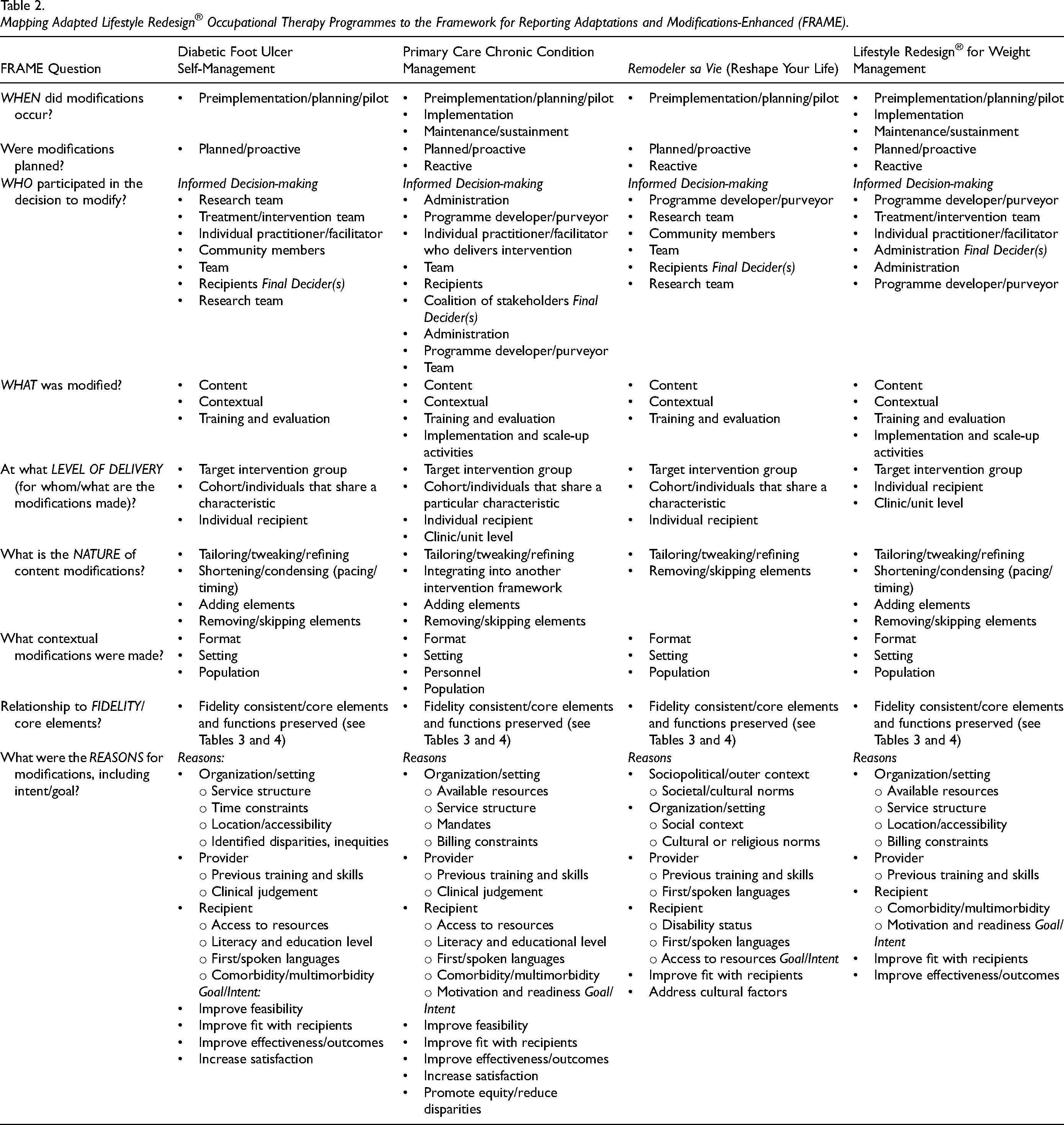
Individuals with in-depth knowledge of each adapted programme, invited as coauthors, received a structured form to document programme modifications. The form included: (1) for reference, a summary of the original WE LR-OT programme structure (Supplemental Table 1) along with descriptions of the LR-OT core characteristics, domains, and techniques; (2) a section to outline steps taken to modify the programme into its current form; (3) a table informed by the template for intervention description and replication (Hoffmann et al., 2014) to document the programme's structure (Table 1); (4) a mapping table of questions, definitions, and predefined responses from the FRAME Coding Manual (Stirman, 2023; see Table 2), and space for detailed responses to ensure accuracy and alignment with FRAME definitions; and (5) a mapping template to link adaptations to LR-OT's core characteristics (Table 3) and domains (Table 4), which served as a fidelity check.
Mapping Adapted Lifestyle Redesign® Occupational Therapy Programmes to the Framework for Reporting Adaptations and Modifications-Enhanced (FRAME).
Examples of how the Well Elderly Programme and Adapted Programmes Align With Lifestyle Redesign® Core Characteristics.
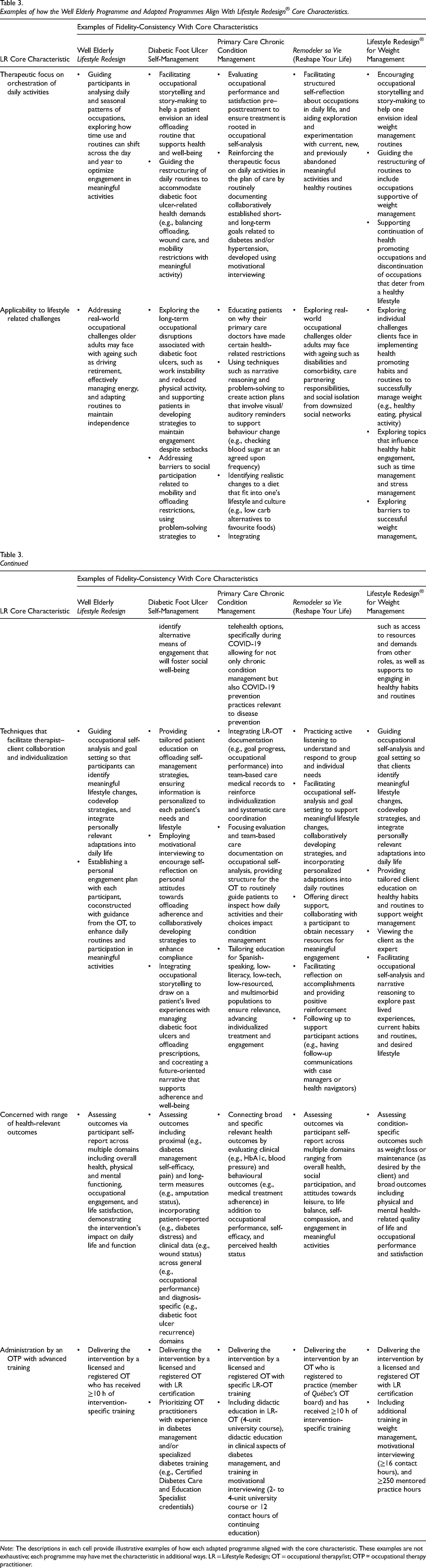
Note: The descriptions in each cell provide illustrative examples of how each adapted programme aligned with the core characteristic. These examples are not exhaustive; each programme may have met the characteristic in additional ways. LR = Lifestyle Redesign; OT = occupational therapy/ist; OTP = occupational therapy practitioner.
Examples of Content from the Original Well Elderly Programme and Tailored Topics from Each Adapted Programme That Align With Lifestyle Redesign® Core Domains.
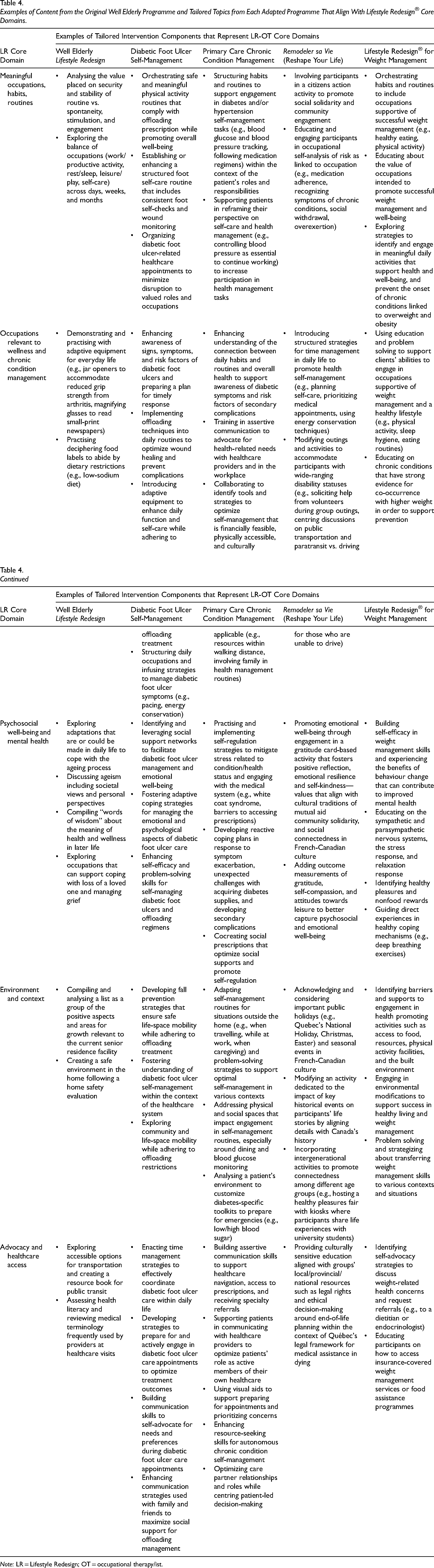
Note: LR = Lifestyle Redesign; OT = occupational therapy/ist.
Completion of the structured documentation was guided by multiple sources of data, including: (a) programme records (e.g., study protocols, manuals, Institutional Review Board [IRB] applications); (b) publications, including those that reported implementation context, feasibility, and other process indicators; and (c) the experiential knowledge of team members directly involved in programme design, delivery, or evaluation. This triangulated approach ensured that adaptation documentation reflected both written materials and lived experience with the programme's implementation. Upon submission, two LR-OT-certified authors (SSN, EAP), both with in-depth knowledge of the WE programme and LR-OT framework, reviewed each form for accuracy and completeness. Discrepancies or unclear classifications were discussed and resolved with the broader authoring team. The compiled materials were then analysed to identify frequency and patterns of adaptations across teams.
The research activities described in this paper involve a review and analysis of programme adaptations and do not involve human participants or identifiable private information. As such, these activities were determined to be Not Human Subjects Research in accordance with the University of Southern California IRB guidelines and did not require IRB oversight.
Results
Adaptation Processes Across Programmes
Overview
This section overviews the adaptation processes used across the four programmes, illustrating how each team approached LR-OT modification. The DFU-SM study team followed the ADAPT-ITT (Assessment, Decision, Administration, Production, Topical experts, Integration, Training, and Testing) model (Wingood & DiClemente, 2008) to adapt LR-OT by including the following steps. Assessment: DFU patients’ needs were identified via literature reviews and the team's prior needs assessment research (Crocker et al., 2021). Decision: adaptation was chosen over adoption. Administration: theatre testing of diabetes-focused LR-OT was conducted to gather tailoring recommendations from key informants (e.g., DFU patients, podiatrists). Production: DFU-specific materials and intervention processes were drafted. Topical experts: modifications were made to initial materials/processes with guidance from DFU experts (e.g., wound care nurse, orthotist). Training: a certified LR-OT intervener and research staff were trained in intervention- and study-specific details. Testing: a pilot clinical trial (goal N = 20) is ongoing to assess programme feasibility and potential for improving patient outcomes.
The PC-CCM team began the adaptation process (see Pyatak et al., 2019) by meeting with primary care clinic leadership at a safety-net medical centre to discuss clinic needs and integration of LR-OT services. The target patient population was selected—patients with uncontrolled diabetes—and the REAL Diabetes treatment manual (another LR-OT adapted programme) was trialled in a 1-year hybrid effectiveness–implementation study (N = 73; Pyatak et al., 2019). Following the pilot study, the team met with clinic leadership to explore sustaining LR-OT services within the clinic's interdisciplinary team, and expanding services to include hypertension management. Upon securing support, the team developed processes to onboard a resident, including training the resident in clinic-specific procedures and in delivering modified LR-OT services that address both diabetes and hypertension management in the primary care setting.
The RV study team undertook a transcultural adaptation process involving rigorous translation of WE LR-OT materials into French and collaboration with end users, older adult organizations, and OT associations to ensure cultural appropriateness. The RV programme retained many structural features of the original WE intervention but modified content to reflect the healthcare system, social norms, and values of Francophone older adults. A mixed-methods feasibility and pilot study was conducted with older adults (N = 17), OTs, and decision-makers to ensure programme relevance, acceptability, and preliminary efficacy in the Québec context (Levasseur et al., 2022).
The WM programme emerged organically from knowledge gleaned from the WE studies, expert consultations (e.g., nutritionist, economist), and review of relevant evidence. Designed for immediate clinical implementation without pilot testing, it incorporated preplanned adaptations based on anticipated needs of clients pursuing WM and to improve its appeal to private health insurers and self-insured employers. As the healthcare landscape evolved and new funding opportunities emerged—such as obesity becoming a billable diagnosis—clinic leadership engaged in iterative adaptations to align with changing reimbursement models, including integration into broader healthcare systems and insurance networks. These adaptations were guided by assessments of logistical feasibility, financial sustainability, and client engagement. Throughout, adaptation decisions reflected a dynamic process shaped by contextual demands, resource availability, and client input.
Patterns of adaptations
Despite varying adaptation strategies, common patterns and distinctions emerged across the four programmes. The DFU-SM team adhered to a formalized, stepwise process using the ADAPT-ITT framework. The other teams followed more flexible adaptation processes but still featured key steps commonly included in systematic adaptation frameworks (Escoffery et al., 2018). For example, the PC-CCM team adapted based on stakeholder input and prior research, while RV employed a rigorous translation and cultural tailoring process. The WM programme, in contrast, implemented a fluid adaptation process informed by client feedback, clinical context, and evolving payer requirements. Pilot testing was conducted by all except the WM team. Although pilot testing can be an effective method that reduces the need for extensive reactive adjustments, it can also be resource-intensive and delay scale-up (Beets et al., 2021). Teams weighed these trade-offs in light of their goals and resources.
As mapped to FRAME, all programme adaptations began at the preimplementation/planning/piloting stage (Table 2). Adaptations during preimplementation and planning phases were proactive (e.g., the DFU-SM and RV teams conducted linguistic translation before pilot testing), whereas those occurring during pilot testing or implementation were reactive (e.g., the WM team pivoted screening practices to accommodate reimbursement changes). Unlike the PC-CCM and WM teams which had to rapidly transition to telehealth due to the pandemic, the DFU-SM team preemptively incorporated a telehealth model, enabling careful planning to optimize intervention quality. The PC-CCM and WM teams also enacted proactive modifications during the maintenance/sustainment phase. The PC-CCM group explored the residency model to sustain the piloted programme after the conclusion of the grant-funded preliminary study, while the WM programme focused on maintaining financial viability by seeking Preferred Provider Organization coverage following conclusion of initial contracted services.
Engagement of key players was essential across all programmes (Table 2). Decision-making was collaborative, and input ranged from expert perspectives on condition management (e.g., consulting nutritionists in adapting the WM programme) to administrative considerations (e.g., budgeting for staff training and ensuring alignment with patient privacy laws in the PC-CCM programme). Among all programmes, PC-CCM was the only one that explicitly identified a coalition of affected stakeholders (e.g., the IT department responsible for building electronic medical record forms). The PC-CCM and WM programmes, having progressed to full implementation, involved a broader group of decision makers including individuals responsible for integrating programmes into routine care, such as clinical leadership. Because the DFU-SM (pilot ongoing) and RV programmes had not yet reached the implementation stage, their research teams served as the sole final deciders.
Each team aimed to adapt their programme primarily to improve fit with recipients. All programmes except for RV sought to improve outcomes, a distinction likely due to RV's close alignment with the original WE programme and prioritization of replicating WE's excellent outcomes that were relevant to the French-Canadian population. The PC-CCM team uniquely emphasized reducing disparities as a driver for adaptation, particularly within the underresourced, safety-net patient population, highlighting its focus on social determinants of health.
Reasons for adaptation aligned with FRAME's four categories. Organizational/setting factors played a role across all programmes, with the clinically focused teams adapting to fit within service structures and address practical constraints such as resource availability and billing. Recipient factors were also universally considered, with teams adapting most commonly for resource access, comorbidity, and language needs. For the latter recipient factor, the DFU-SM and PC-CCM teams proactively modified materials for Spanish-speaking communities and the RV team rigorously adapted resources and content for the Francophone community.
All teams identified provider-level previous training and skills as a reason for adaptation, with the DFU-SM and PC-CCM teams also noting clinical judgement. Training adaptations incorporated condition-specific requirements in the DFU-SM, PC-CCM, and WM programmes, while the RV group capitalized on newly created training resources for the OT community made available at the conclusion of the WE studies. Finally, sociopolitical factors were relevant for the RV programme, which placed strong emphasis on selecting societal and cultural norms applicable to the social context of French-Canadian older adults.
Characteristics of Programme Structure and Delivery Model Adaptations
The above adaptations shaped key structural and delivery modifications across programmes. All teams reported training and evaluation, contextual, and content modifications, and two identified implementation and scale-up activity adaptations. These modifications occurred at delivery levels, ranging from target intervention group-level (e.g., the RV team's translation of materials into French for the Francophone community) to clinic/unit-level changes (e.g., clinic-wide workflow adjustments in the WM and PC-CCM programmes).
Training and evaluation adaptations
Modifications to training and evaluation were made with the intention to ensure interventionists possessed the prerequisite knowledge and skills to treat the target population and that programme outcomes were suitably captured. For instance, the DFU-SM team implemented a combined guided and self-study approach to orienting the OT to DFU self-management to complement the LR-OT's assumed baseline knowledge of general diabetes care. (Although programme teams reported that orientation and training approaches were modified to support interventionists’ preparedness, this study did not directly measure knowledge acquisition or competency.) Regarding evaluation, the RV team added measures of self-compassion and gratitude which aligned with the intervention's cultural changes. The clinically focused DFU-SM, PC-CCM, and WM teams introduced objective clinical indicators to their assessment batteries (e.g., electronic medical record-documented wound healing status, Hemoglobin A1c [HbA1c], and body composition, respectively) to sync with expected healthcare service outcomes. In contrast, the original WE programme focused exclusively on self-report measures.
Contextual adaptations
Contextual modifications included adaptations to the intervention's format, target population, implementation setting, and personnel. The delivery format of the DFU-SM and PC-CCM interventions focused exclusively on one-to-one treatment sessions whereas the WM programme initially offered both individual and group formats before transitioning to an individually focused model. The RV programme maintained a primarily group-focused model with monthly one-to-one sessions, preserving a “peer exchange” element from WE not featured in the other programmes. A fully telehealth delivery mode is being tested in the DFU-SM study, while the PC-CCM and WM programmes pivoted from in-person to telehealth during the COVID-19 pandemic. Postpandemic, the WM programme now offers telehealth or in-person options. Of the four programmes, only the PC-CCM team modified personnel from the WE model of practicing OTs, integrating postprofessional doctoral OT residents to build workforce capacity.
Content adaptations
Although the WE study allowed for flexibility in delivery, all four programmes made content modifications designed for specific target populations. These adaptations included tailoring/refining, adding elements, removing/skipping elements, shortening/condensing pacing or timing, and in the PC-CCM programme's case, integrating the intervention into another framework.
Tailoring was a common strategy, as the broad topics outlined in the WE study provided a foundation for customization. The PC-CCM programme aligned its content with safety-net primary care patients’ needs, while the DFU-SM programme tailored elements related to foot self-care and offloading management. Similarly, the RV programme was culturally adapted for French-Canadian older adults, incorporating local healthcare organizations and resources. The WM programme adjusted its content to include WM topics such as the psychological and behavioural aspects of eating, refining the WE content on dining and social eating to include emotional eating and alternatives to food-based reward systems. Additionally, most programmes—except for RV—removed age-specific language so that the materials were not limited to older adults but could be applied across a broader adult audience.
Language modifications were also prominent. Although the WE study permitted tailoring language for participant comprehension, the DFU-SM, PC-CCM, and RV teams proactively translated materials at the outset to meet the known linguistic needs of their target populations. Spanish translations were incorporated into the DFU-SM and PC-CCM programmes, while the RV programme adapted materials into French. Other refinements included modifications to worksheets and handouts. For instance, the DFU-SM team tailored coping strategies to address offloading management for foot wounds. Healthcare content was also revised to reflect the realities of different healthcare systems, such as the RV programme's focus on navigating Canada's public health system and the PC-CCM programme's integration within a patient-centred medical home model.
Beyond tailoring, three of the programmes introduced additional content to address population-specific concerns. The WM programme incorporated structured materials on eating routines, meal planning/preparation, and grocery shopping; the DFU-SM programme added content on foot self-care routines, adaptive equipment for offloading, and safe physical activity; and the PC-CCM team expanded content to address issues such as building emergency toolkits for high/low blood sugar and planning for common comorbid conditions such as visual impairment and peripheral neuropathic pain.
In contrast, each programme removed or skipped content that was less relevant to their populations. All but the RV team eliminated the WE “group outing,” primarily to align with the transition to one-to-one sessions and fit with altered programme delivery settings. For their initial groups, the RV team did not target WE content related to hormones, ageing, and sexuality, as participants did not choose these topics.
Adjustments to the pacing or length of the WE programme (6–9 months) were also noted. The DFU-SM team reduced its programme to an eight-session, approximately weekly model to accommodate grant funding timeline constraints. Similarly, the WM programme originally implemented a 4-month weekly format to fit with established contracts but allowed clients to engage in additional continuation sessions if requested.
The PC-CCM team was the only group that integrated LR-OT into an alternate intervention framework: the team-based care model. This was accomplished through electronic health record messaging, structured documentation, and in-person discussions with the clinical team to ensure that patients’ daily habits, routines, and goals were incorporated into collaboratively managed health plans.
Despite making content modifications, none of the teams reported deviations from the intervention framework, such as drifting from LR-OT principles or integrating other treatments into the programme. Rather, adaptations were made to preserve the relevance, feasibility, and accessibility of the intervention while maintaining fidelity to its foundational approach. Although Table 2 categorizes these content modifications, the next section will examine the extent to which the adapted programmes remain consistent with LR-OT's core characteristics (Table 3) and core domains (Table 4).
Implementation/scale-up adaptations
The PC-CCM and WM teams also made adaptations to support implementation and scale-up efforts, as the WE studies involved research-based implementation and did not have an established method of integrating services into routine community programming. For the PC-CCM programme, the team educated referring providers during staff meetings to increase awareness of LR-OT services and coordinate care with other clinical team members from the unit. The WM programme involved modifications to facilitate programme implementation (e.g., securing insurance coverage and extending eligibility for reimbursement).
Fidelity Consistency with LR-OT Core Elements
Given the breadth of adaptations made across multiple programme components, it is essential as part of the FRAME to assess whether these modifications remained aligned with LR-OT's core elements (Figure 1). In this section, we describe how the adapted programmes preserved fidelity to LR-OT's core characteristics (Table 3) and core domains (Table 4), based on illustrative examples provided by each team. Although teams were not asked to supply exhaustive accounts, the examples demonstrate consistency with LR-OT's defining features and were deemed sufficient to indicate fidelity alignment.
Core characteristics
All four adapted programmes, as characterized through programme team accounts and available documentation, maintained fidelity to the core characteristics of LR-OT, reinforcing the intervention framework's adaptability across diverse populations and contexts (Table 3). The RV programme most closely mirrored the original WE programme, with its primary distinction being cultural and linguistic adaptations for French Canadians. As a result, its mapping to the core characteristics largely paralleled that of the WE programme. Across all programmes, a key emphasis remained on optimizing daily routines, whether through assisting patients in structuring offloading regimens in the DFU-SM programme or guiding adjustments to routines to support healthy weight in the WM programme. Similarly, each programme provided examples of lifestyle-related challenges specific to its target population, such as the PC-CCM programme addressing the potential mismatch between diabetic dietary restrictions and favourite foods, and the RV programme acknowledging evolving care responsibilities with ageing. Health-related outcomes remained a central focus, with the clinically adapted programmes expanding beyond the original WE programme's psychosocial measures to include physiological markers such as blood pressure and body composition. The therapist–client dynamic was consistently shaped by core LR-OT techniques that supported collaboration and individualization, ranging from motivational interviewing to occupational self-analysis. Although the specific training requirements for interventionists varied by programme, all OT practitioners required advanced training in LR-OT, with some adaptations necessitating additional clinical expertise, such as diabetes management for the DFU-SM and PC-CCM programmes or specialized knowledge of weight regulation in the WM programme.
Core domains
The adapted programmes remain aligned with the core domains. Table 4 illustrates how both the original WE programme content and the modified content from the adapted programmes mapped onto these domains while also addressing the unique needs of each target population and implementation context.
Across all adaptations, meaningful occupations and psychosocial well-being remained central, with numerous examples demonstrating how content was tailored while upholding these foundational elements. Although some programmes modified session topics or introduced additional materials beyond those in the WE programme, they consistently addressed essential LR-OT domains—for instance, attending to the physical environment for fall prevention, which in the DFU-SM programme specifically focused on safe use of an offloading device. Certain programmes emphasized particular domains more heavily to meet their population's needs, such as the clinically based programmes prioritizing advocacy and healthcare access. Similarly, the DFU-SM and PC-CCM programmes, relative to the original WE programme content, placed greater emphasis on chronic condition management, given their focus on patients with specific diagnoses.
Discussion
This study applied the FRAME to examine four programmatic adaptations of LR-OT. Through a multiphase process, each team engaged in adaptations to align the intervention with contextual and population-specific needs while maintaining fidelity to LR-OT's fundamental principles. Analysis was informed primarily by structured documentation completed by team members with in-depth knowledge of each programme, supplemented by programme records and published materials. Several key adaptation patterns emerged, highlighting strategies that upheld core characteristics and domains of the intervention while ensuring appropriate contextual fit.
By analysing adaptation strategies and evidence of fidelity-consistency across programmes, we identified critical factors that contributed to successful modifications. Specifically, teams balanced fidelity and fit, a well-documented tension in implementation science (Mejia et al., 2017). Rather than treating fidelity and adaptation as opposing forces, teams navigated this balance by implementing culturally responsive modifications, adjusting programme delivery, engaging key stakeholders in decision-making, and leveraging interdisciplinary partnerships. These strategies reflect the perspectives of LR-OT programme insiders and available documentation, though the actual impact on participant outcomes was not directly measured. Thus, this study builds on the work of Pyatak et al. (2022) by further clarifying the essential elements of LR-OT, situating core domains and techniques within real-world adaptations. Further, the study highlights considerations for scaling and sustaining LR-OT interventions. Modifications such as telehealth integration, alignment with clinical workflows, and condensed programme structures tailored to health system constraints may enhance programme scalability but require further empirical validation. Additionally, ensuring sustainable financial structures, including reimbursement opportunities, appears essential for broader programme dissemination.
A critical challenge involved addressing practical constraints and resource limitations inherent to different settings. For example, in medical contexts, LR-OT was adapted to align with clinic workflows and the priorities of interdisciplinary teams, such as the requirement to integrate objective health indicators. Such modifications facilitated programme adoption and sustainability, reinforcing the importance of contextual fit in implementation success. The role of structured flexibility in scaling interventions warrants further investigation. Researchers argue that scalability is enhanced when interventions maintain key core elements while allowing adaptable delivery mechanisms (Aarons et al., 2017).
The LR-OT variants examined in this study benefited from long-standing access to LR-OT developers, which may have provided atypical resources for ensuring fidelity-consistent adaptations. This highlights the importance of comprehensive training and deep understanding of intervention frameworks in successful adaptation efforts. Lifestyle Redesign® Certification (USC Chan Division of Occupational Science and Occupational Therapy, n.d.-a) may play a crucial role in supporting clinicians to achieve successful modifications while maintaining fidelity to core principles.
By systematically examining LR-OT adaptations, this study advances OT intervention research within the implementation science arena. Building on Piller and colleagues’ (2021) work using FRAME to report adaptations to a stepwise vestibular and bilateral integration OT intervention, this is the first application of FRAME to an individualized, client-centred OT intervention model. We emphasize that findings describe the adaptation processes as documented by knowledgeable programme team members and do not provide empirical evidence regarding intervention effectiveness for participants. Although LR-OT is a distinctive form of client-centred OT, the process and principles for documenting and guiding adaptations—particularly with FRAME—is broadly applicable to other complex OT interventions. This study bridges a critical gap between OT practice and implementation science by demonstrating how a flexible OT intervention framework can be adapted systematically while maintaining fidelity consistency, as assessed through structured documentation and mapping to core elements.
Finally, these findings have policy implications for funding and supporting adaptable health interventions. Reimbursement models and grant funding structures should accommodate flexible intervention frameworks such as LR-OT, rather than imposing rigid protocol requirements or fixed intervention durations. Overly restrictive funding criteria risk undermining the effectiveness of client-centred EBPs. Additionally, grant funders should prioritize studies that compare different adaptation approaches to evaluate their impact on intervention outcomes, ultimately strengthening the evidence base for scalable, adaptable interventions.
Limitations and Future Directions
Several limitations warrant consideration. The retrospective, self-reported nature of the adaptation data may have introduced recall bias and compromised the accuracy of the documented modifications. The analysis reflects the subjective assessment of knowledgeable programme team members and available documentation; direct evaluation of the impact of adaptations on participant knowledge, skills, or outcomes was not conducted. Although fidelity consistency was assessed descriptively rather than through independent measurement, insider perspective provides deep contextual insight into how LR-OT adaptations are enacted in practice. Further, the inclusion of only four case examples may not capture the full diversity of adapted LR-OT programmes and limits the generalizability of findings. The use of FRAME also presents challenges. As an emerging tool, FRAME offers limited guidance on application across diverse types of EBPs and practice settings. Specifically, OT interventions often lack stepwise protocols, making FRAME less applicable to many OT EBPs (Piller et al., 2021). LR-OT, with its inherently flexible and client-centred design, complicates the use of FRAME further; its adaptability resists rigid classification and may obscure or hinder tracking of nuanced modifications. Furthermore, the original WE LR-OT programme lacks a standardized implementation protocol, making fidelity assessment difficult across adapted versions. Consequently, this study relied heavily on the programme's identified core characteristics and domains to anchor evaluation.
Looking ahead, the defined LR-OT core characteristics, domains, and techniques offer a useful foundation for guiding future adaptations. Developing an “adaptation data platform” or similar tracking tools, as Piller and team suggested (2021), could support systematic documentation, evaluation, reproducibility, and comparability of adaptations for other types of OT interventions. More broadly, there is a need within the OT field for empirical testing of adaptation strategies and rigorous assessment of their impact on implementation and client outcomes.
Conclusion
This study's findings highlight that structured flexibility within LR-OT enables successful adaptation as documented by knowledgeable programme personnel and investigators. Across programmes, team accounts reflected a successful balance between fidelity and fit through culturally responsive modifications, stakeholder engagement, and integration with local healthcare structures. The results contribute to implementation research in OT by providing a model for systematically documenting intervention adaptations. By demonstrating how fidelity-consistent modifications can enhance cultural and contextual relevance, this study offers practical insights for clinicians and researchers aiming to scale LR-OT or similar EBPs. Additionally, findings emphasize the importance of well-designed training processes, interdisciplinary collaboration, and sustainable funding models to support long-term implementation. At the same time, because these findings rely on insider team accounts rather than direct measurement, they should be interpreted as descriptive evidence of how adaptations were enacted in practice. Future research should investigate the impact of adaptations on client outcomes and develop standardized mechanisms for tracking modifications. Strengthening implementation science within OT will promote identification of scalable, client-centred interventions that remain responsive to evolving healthcare and community needs.
Key Messages
This study demonstrates how documented structured flexibility in the Lifestyle Redesign® occupational therapy (OT) intervention framework can support adaptations that aim to maintain fidelity while responding to diverse cultural and contextual needs.
By applying FRAME to an individualized, client-centred OT intervention, we provide a descriptive model for systematically documenting and analysing adaptations in OT practice, based on programme team knowledge and records.
Supplemental Material
sj-docx-1-cjo-10.1177_00084174251397723 - Supplemental material for Adapting Lifestyle Redesign®: Navigating Fidelity and Contextual Fit Across Four Case Examples
Supplemental material, sj-docx-1-cjo-10.1177_00084174251397723 for Adapting Lifestyle Redesign®: Navigating Fidelity and Contextual Fit Across Four Case Examples by Stacey L. Schepens Niemiec, Lauren Styer, Jasmine Chapman, Elizabeth A. Pyatak, Mélanie Levasseur, Gabrielle Granados, Valerie A. Tapia, Chantelle Rice Collins, Robyn Martinez and Tze-Woei Tan in Canadian Journal of Occupational Therapy
Footnotes
Acknowledgments
The authors would like to acknowledge the funding sources that supported the development and/or implementation of the adapted programmes described in this manuscript. The Diabetic Foot Ulcer Self-management Program and the Primary Care Chronic Condition Management Program were supported in part by the Southern California Clinical and Translational Science Institute through the National Institutes of Health/National Center for Advancing Translational Sciences (NIH/NCATS), Grant UL1TR001855. The Remodeler sa vie programme was supported by the Fonds de Recherche du Québec – Santé (Grants 298996, 26815), the Canadian Institutes of Health Research (Grant 148466), and the Quebec Network for Research on Aging. Mélanie Levasseur holds a Tier 1 Canadian Research Chair in Social Participation and Connection for Older Adults (CRC-2022-00331; 2023-2030). The Lifestyle Redesign® for Weight Management Program was conducted without external funding support. We extend special thanks to Dr. Mike Carlson for his editorial contributions, Dr. Rebecca Cunningham for providing additional background information on the Lifestyle Redesign core elements, and Drs. Katie Jordan and Camille Dieterle for providing additional historical context and details about the evolution of the LR-OT Weight Management Program.
ORCID iDs
Supplemental Material
Supplemental material for this article is available online.
Notes
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.