
Abstract
Introduction
Cerebral Palsy (CP) is the most common cause of life-long disability, and prevalence estimates range from 1.6 to 2.9/1000 live births in high-income countries to as high as 3.7/1000 in low-and middle-income countries (McIntyre et al., 2022). CP is a clinical diagnosis that includes all permanent and nondegenerative disorders of movement and posture due to disturbances in the developing brain (MacLennan et al., 2019). Although CP diagnosis and prediction of future motor prognosis is possible between 3 and 5 months adjusted age (Romeo et al., 2008), in many settings, diagnosis is delayed due to multiple factors, potentially delaying implementation of effective interventions (teVelde et al., 2019).
The Gross Motor Function Classification System (GMFCS) is a valid and reliable 5-point classification of mobility function for individuals meeting the clinical definition of CP (Smithers-Sheedy et al., 2014). Children at GMFCS I are the most able and their primary means of community mobility is walking, while children at GMFCS V have the most physical impairment and are unable to maintain body position or move independently without assistance or sophisticated assistive devices (Palisano et al., 1997).
Children with CP use a wide range of assistive devices to compensate for their motor impairments (Moen & Østensjø., 2023). Children at GMFCS IV and V are primarily dependent on wheeled mobility, while children at GMFCS III walk short distances using hand-held walkers and rely on wheeled mobility for longer distances (Palisano et al., 1997). Children at higher GMFCS levels use the greatest number of devices (Novak et al., 2012; Østensjø et al., 2005) and their families incur greater out-of-pocket expenses as a result (Bourke-Taylor et al., 2014; Novak et al., 2012).
Assistive devices are one means to enable occupational participation. As the Canadian Model of Occupational Participation describes, they may facilitate accessing, initiating, and sustaining valued occupations within meaningful relationships and contexts, including age-appropriate activities, meeting basic, biological and safety needs, and addressing needs for autonomy, competence and relatedness, now and in the future (Egan & Restall, 2022). For young children with CP, and their parents and/or caregivers, occupational participation may include use of devices to assist with bathing, toileting, eating, drinking, dressing, sleeping, positioning, play, education, mobility, and family routines.
Early introduction of assistive devices to enable occupational participation takes advantage of motor and cognitive neuroplasticity (Novak et al., 2017). Cross-sectional studies suggest that 80–90% of children classified as GMFCS III-V use wheeled mobility outdoors, and around 70% are dependent or pushed in manual wheelchairs (Noten et al., 2024; Rodby-Bousquet & Hägglund, 2010). Manual wheelchairs ease caregiving (Østensjø et al., 2005) and increase participation in daily activities (Moen & Østensjø, 2023), even for those unable to self-propel (Andrews et al., 2023). A recent study exploring changes in assistive device use for individuals with CP (GMFCS IV) in the home setting from preschool to adulthood (Cheng et al., 2025) found that while 7/10 children used strollers and 2/10 used manual wheelchairs, none used power wheelchairs at preschool age. Across growth-stages, manual wheelchairs were found to promote mobility and social participation, while strollers merely facilitated transitions. Little is known about use of different types of manual wheelchairs or strollers by young children with CP, or factors influencing parent-choice or therapist recommendation.
Adaptive seating may improve postural alignment (Chung et al., 2008) and promote participation in self-care and play activities (Angsuipaisal et al., 2015), although evidence level and quality are limited. More recent experimental studies have measured improved postural alignment and function in young children (GMFCS III–V) using adaptive seating in comparison to a regular chair (Sahinoglu et al., 2017) and improved trunk and head control, fine-motor, self-care abilities, and child and family functioning following provision of a first adaptive seating system (Inthachom et al., 2021). Child and family functioning may also be improved or maintained following adaptive seating replacement (Ryan et al., 2014). Families believe that adaptive seating can help prevent secondary impairments, increase functioning (e.g., eating, drinking, or play/hand use), and enhance participation as well as ease caregiving (Moen & Østensjø, 2023; Cheng et al., 2025). In longitudinal studies, families also report increased child function, socialization, participation, and reduced burden-of-care (Barton et al., 2022; Kurne & Gupta, 2016).
Research on the use and benefits of any type of assistive device to support self-care activities or abilities of children with CP is very limited. Older regional surveys suggest that personal hygiene devices, such as those used for toileting or bathing, are primarily used at home (Korpela et al., 1992), although some children use toilet seats at daycare or school (Korpela & Koivikko, 1992). Bathing devices primarily ease caregiving, while toileting devices also improve function and independence (Moen & Østensjø, 2023). However, bathing and toileting devices may be discontinued if they do not ease caregiving (Østensjø et al., 2005).
Although it may be assumed that children with more impaired motor abilities use more supportive devices for mobility, supported sitting and activities of daily living, and spend more time using these devices, little has been published to substantiate this. As part of a larger study exploring the effects of a 6-month power mobility device loan (Field & Livingstone, 2022; Livingstone & Field, 2021, 2023), use of other positioning and mobility devices was collected along with longitudinal use of the power mobility device. To help guide clinical practice, and advance research evidence, it is also important to explore associations between children's functional classifications, specific types of devices used (describing both function and degree of adaptability for individualized needs), and time spent using these devices.
The primary aim in this paper was to describe use of wheeled mobility, adaptive seating, bathing and toileting devices by young children with CP (GMFCS III-V), and to examine whether child factors (e.g., age, gross motor, manual, or postural control abilities) influence type of device used. The secondary aim was to examine whether child factors or device type, including function (mobility, positioning or self-care) and degree of adaptability (typical or adaptive), are associated with the time spent using these devices.
Method
This secondary analysis examined parent-reported use of wheeled mobility, adaptive seating, bathing, and toileting devices by children who had been provided with power mobility devices as part of the pre-post research study. Selection and use of these other devices was not manipulated as part of the research study but represents community-based provision. Typical early childhood equipment such as strollers, high chairs, or booster seats were chosen and purchased by the family. Specialized and adaptive equipment such as wheelchairs, adaptive strollers, adaptive seating, bathing, and toileting devices were recommended by children's community therapists in collaboration with parents, funded and provided within clinical practice.
Participants
Recruitment included a subgroup of children functioning at GMFCS III–V who were part of a larger pre-post power mobility study.
Inclusion Criteria
Thirty-five children meeting clinical criteria for a CP diagnosis, and classified at GMFCS III–V were included. Since seven children participated in two separate power mobility loans at different ages, data was available for 42 participants at two time-points.
Exclusion Criteria
Children diagnosed with: CP but classified as GMFCS I or II; neuro-degenerative disorders; degenerative neuromuscular conditions; spina bifida; or Down syndrome.
Ethics approval was granted by University of British Columbia and Children's and Women's Health Centre of British Columbia Research Ethics Board (H15-02666). All parents provided written informed consent.
Data Collection
Details regarding device use were collected via parent-report using the Home Use of Technology for CHildren (HUTCH) (Ryan & Campbell, 2009). Researchers completed the HUTCH form with parents via interview either in-person or by telephone. The first time point (T1) took place three to four weeks after the child started using the power mobility device and the second measurement point (T2) was at the end-of-loan appointment approximately 5–6 months later. At each time-point, parents did not complete a daily paper diary, but estimated average daily time their children had used mobility, seating, or bathroom devices during the previous week.
The original research version (2008, R1) of the HUTCH diary was used in this study. It has seven device categories with time reported on a six-point scale (≤1 h, 2, 3, 4, or 5 h and ≥6 h). The final version of HUTCH includes nine device categories (dividing toileting and bathing devices so time for each is collected separately). This final version uses the same six-point time-scale and has minor differences in wording and layout. It has good face and content validity, and test-retest reliability (ICC = 0.91; 95% CI = 0.69–0.97) (Ryan & Campbell, 2009).
HUTCH was modified to meet the needs of the larger pre-post study:
Since HUTCH authors reported floor effects for both power mobility and bathroom devices, time of use ≤1 h was broken down into: ≤15 min, 16–30 min, and 31 min–1 h, resulting in a total of eight time-increments. Device use was collected for all settings during the entire day since several families planned to use power mobility devices in community settings.
No additional reliability testing was completed for these minor modifications.
GMFCS levels were classified, based on child usual function at the end of the larger pre-post study. Manual abilities were classified by Manual Abilities Classification System (MACS) (Eliasson et al., 2006) or MiniMACS (Eliasson et al., 2017) for children under 4 years of age. These are referred to simply as MACS for ease of reading. GMFCS and MACS are validated for use with individuals who have CP. Scores range from I to V, with V being the most impaired. In this study, participants’ manual abilities were dichotomized into two groups: more functional (II–III) and more impaired (IV–V).
Level of Sitting Scale (LSS), an indicator of seated postural control, was researcher-administered, to classify children's ability to maintain bench sitting for 30 s with feet unsupported (Fife et al., 1991). Children who are able to move in and out of the seated position are classified at levels 6–8, while children who can sit without movement are classified at level 5. Children at levels 1–4 require support to maintain a seated position ranging from 1 (unable to be supported in this position by one person) to 4 (requiring support at the pelvis). LSS is valid and reliable for use with multiple diagnoses (Field & Roxborough, 2011; 2012; Fife et al., 1993). For our population, levels were dichotomized as able to sit (5–8) and require support (2–4).
Data Analyses
Data were managed using REDcap (Harris et al., 2009), checked and exported to open-source R Version 4.2.1 for all statistical analyses (R Core Team, 2022; Bonnett, 2022; Kassambara, 2021; Mangiafico, 2022; Patil, 2021). Descriptive analyses summarized participant characteristics (age, sex and functional classifications), device types, and time used. Depending on data-type, analyses included frequencies, percentages, range, measures of central tendency, and dispersion.
Time spent in each device was divided into three categories (≤1 h, 2–5 h, and ≥6 h) to differentiate light, moderate and heavy device use (Ryan & Campbell, 2009). The additional categories of ≥15 min and 16–30 min were used only to analyze bathroom device and power mobility device time. Detailed results regarding power mobility devices used, and associations between time in power mobility device and child classifications have been previously reported (Livingstone, Paleg & Field, 2024).
For nominal statistical analyses, primary manual mobility and seating devices were included for children where more than one device was reported in each category. Primary devices were grouped as follows:
Manual mobility: tilt-in-space wheelchair, upright wheelchair (folding or rigid) or stroller (typical or adaptive). Seating: Adaptive (adaptive seat with or without base, floor or corner seat, comfort or beanbag chair), Typical (high chair or booster seat), None (no adaptive seating), or Wheelchair (uses mobility base with specialized supportive seating only). Personal hygiene devices: Due to small numbers, both toileting and bathing devices were dichotomized as: supportive device or no device. For toileting, no device indicated that the child was not toilet training and used diapers/pull-ups only. For bathing, no device indicated that the child could sit in the bath without support.
McNemar and exact symmetry tests compared time and device choice for all devices at T1 and T2. Fisher's Exact Test (two-sided) examined nominal comparisons at one time-point with alpha <0.05. Odds ratios and Phi coefficients were reported for 2 × 2 contingency tables. Phi effect size was interpreted as: small 0.10–<0.30; medium 0.30–<0.50; and large ≥0.50 (Cohen, 1988). Cramér's V effect size was reported for larger tables and interpreted as: small 0.07–<0.20; medium 0.20–<0.35; and large ≥0.35 (Cohen, 1988). For post-hoc tests of statistically significant results, Bonferroni correction adjusted for multiple comparisons. Influence of child age was examined visually using boxplots.
Results
Parent-reported data was collected for 42 participants (35 individual children) aged 18–80 months at T1 and 24–87 months at T2. HUTCH interviews were completed with 34 mothers, four fathers, three foster parents, and one caregiver. McNemar and exact symmetry tests confirmed no statistically significant differences in device or time using devices between T1 and T2.
Table 1 provides details of child profile and device-use. An additional manual mobility device (most commonly a stroller) was reported for nine participants at T1 and for two participants at T2, while one child at each time-point did not use any manual mobility device. Only 10/23 children under 48 months used strollers as their primary mobility device. Tilt-in-space wheelchairs were used from 22 months, and upright wheelchairs from 42 months.
Manual Mobility, Adaptive Seating, Toileting, and Bathing Device Use Reported by Parents at Start and End of 6 Months
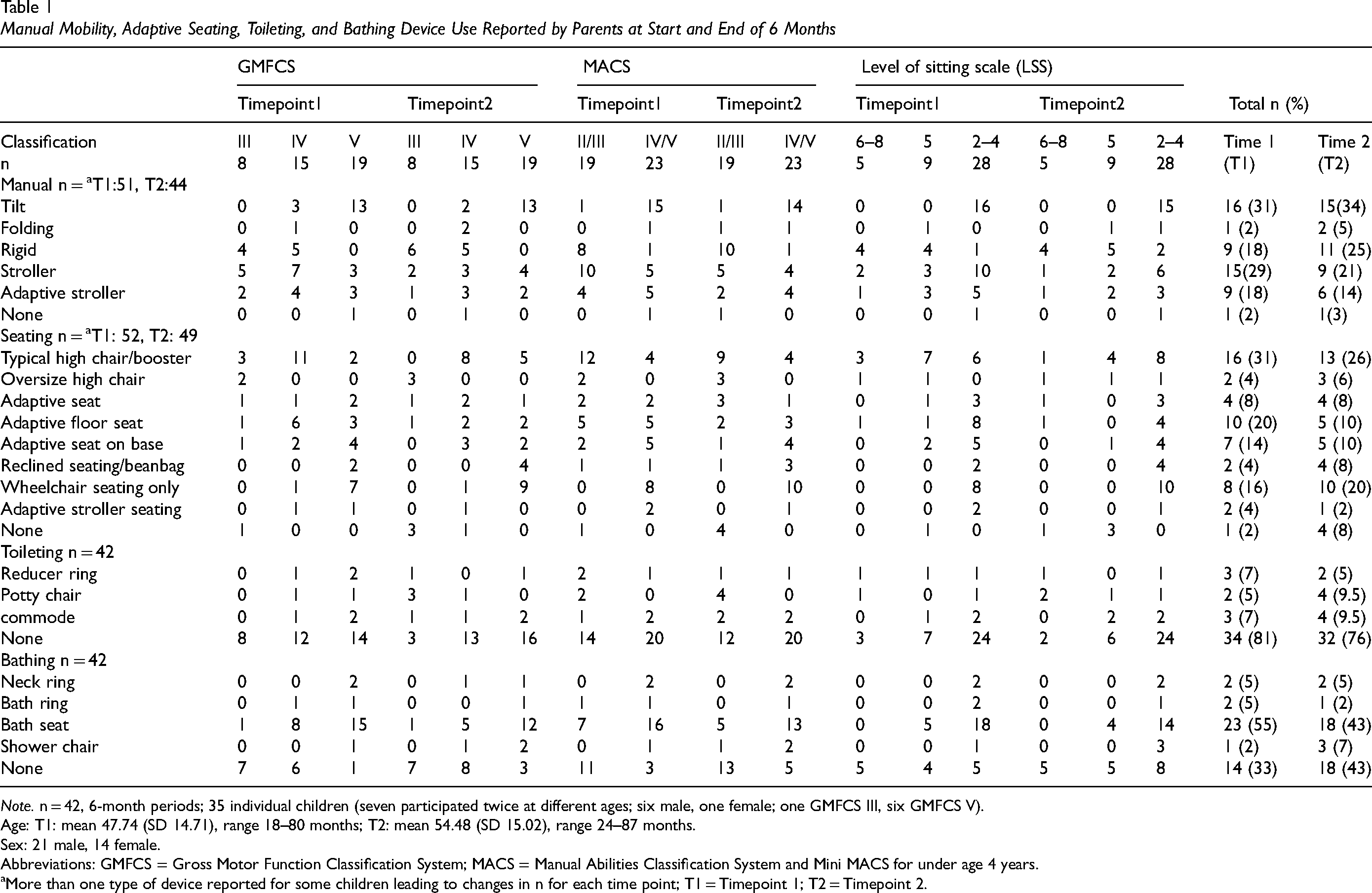
Note. n = 42, 6-month periods; 35 individual children (seven participated twice at different ages; six male, one female; one GMFCS III, six GMFCS V).
Age: T1: mean 47.74 (SD 14.71), range 18–80 months; T2: mean 54.48 (SD 15.02), range 24–87 months.
Sex: 21 male, 14 female.
Abbreviations: GMFCS = Gross Motor Function Classification System; MACS = Manual Abilities Classification System and Mini MACS for under age 4 years.
More than one type of device reported for some children leading to changes in n for each time point; T1 = Timepoint 1; T2 = Timepoint 2.
For adaptive seating, one child used three seating devices at both time-points, while another used three at T1 only. Two devices were used by seven children at T1, and six at T2. The most common additional device was a typical high chair (10/13 reports). However, 9/19 children at GMFCS V used only their customized seating device within tilt-in-space manual wheelchairs.
Figure 1 illustrates the influence of child age using boxplots. Children using strollers appeared to be younger, while children using supportive seating only within their wheeled mobility device appeared to be older, particularly at T2. Age did not appear to influence use of bathing devices, but there was a slight trend toward increased use of toileting devices with older children.
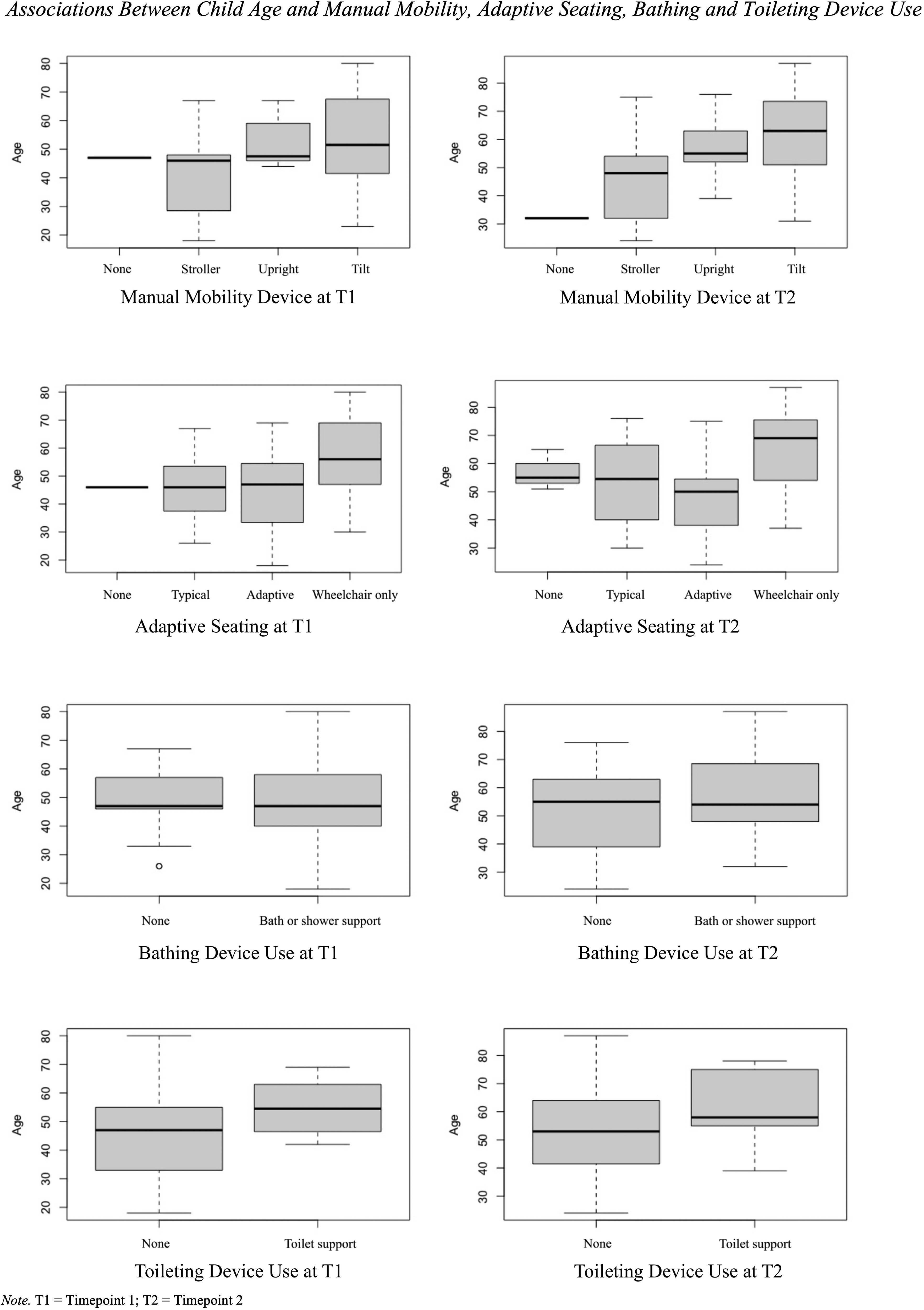
Associations between child age and manual mobility, adaptive seating, bathing, and toileting device use.
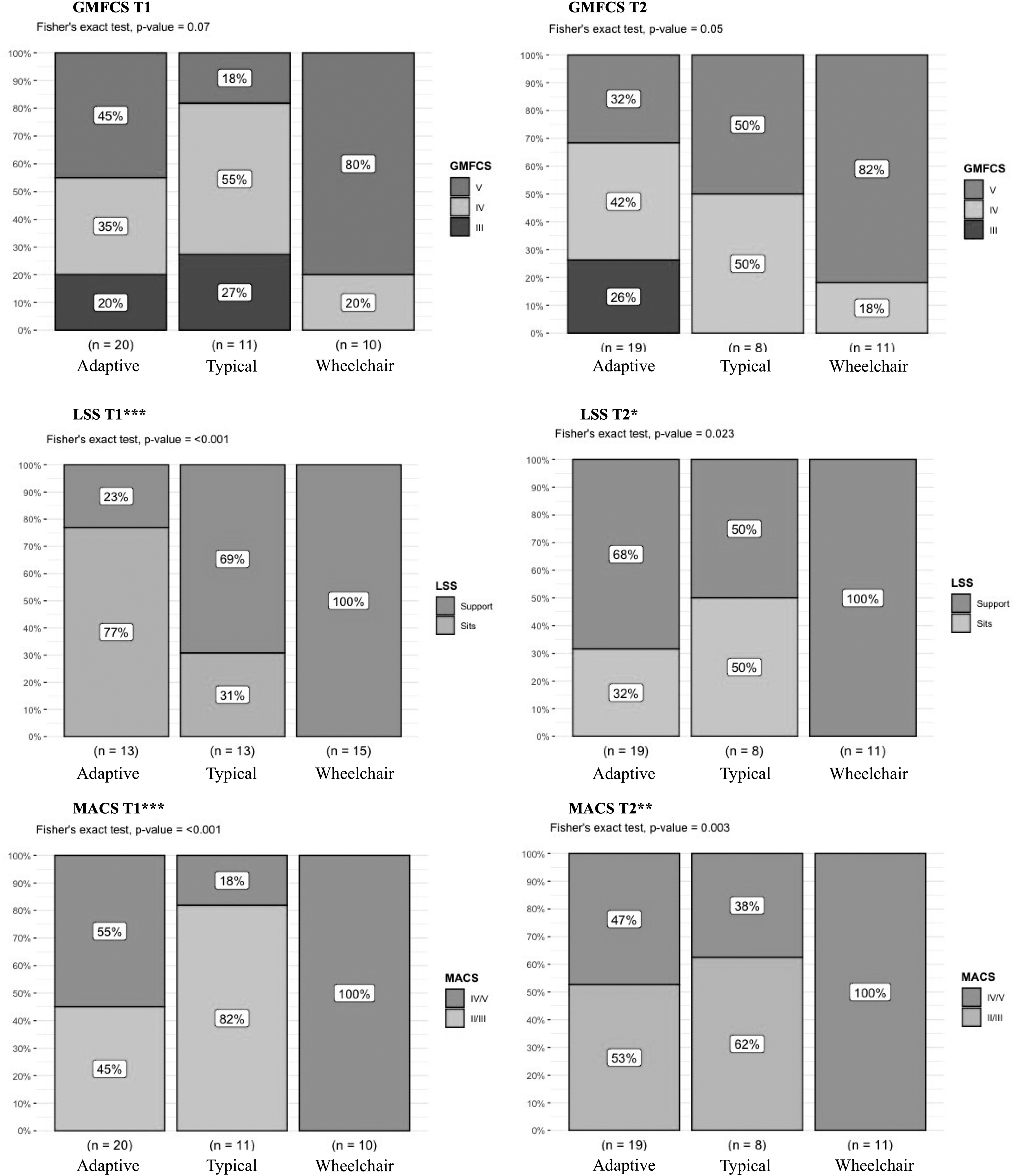
Table 2 and Figure 2 illustrate that GMFCS, LSS, and MACS classifications were all statistically significantly associated with choice of manual mobility device. Differences were seen between tilt and upright wheelchairs, with tilt wheelchairs more likely to be used by those at GMFCS V. In post-hoc tests, upright wheelchairs were less likely to be used by children at GMFCS V in comparison to GMFCS III, but this was statistically significant only at T2. Similarly, children who required support to sit (LSS 2–4) were more likely to use tilt than upright wheelchairs, with large effect sizes. They were also less likely to use upright wheelchairs than strollers, but this was only statistically significant at T1. Manual abilities were significantly associated with use of either tilt or upright wheelchairs, and tilt wheelchairs or strollers at T1, as well as tilt wheelchairs or strollers at T2.
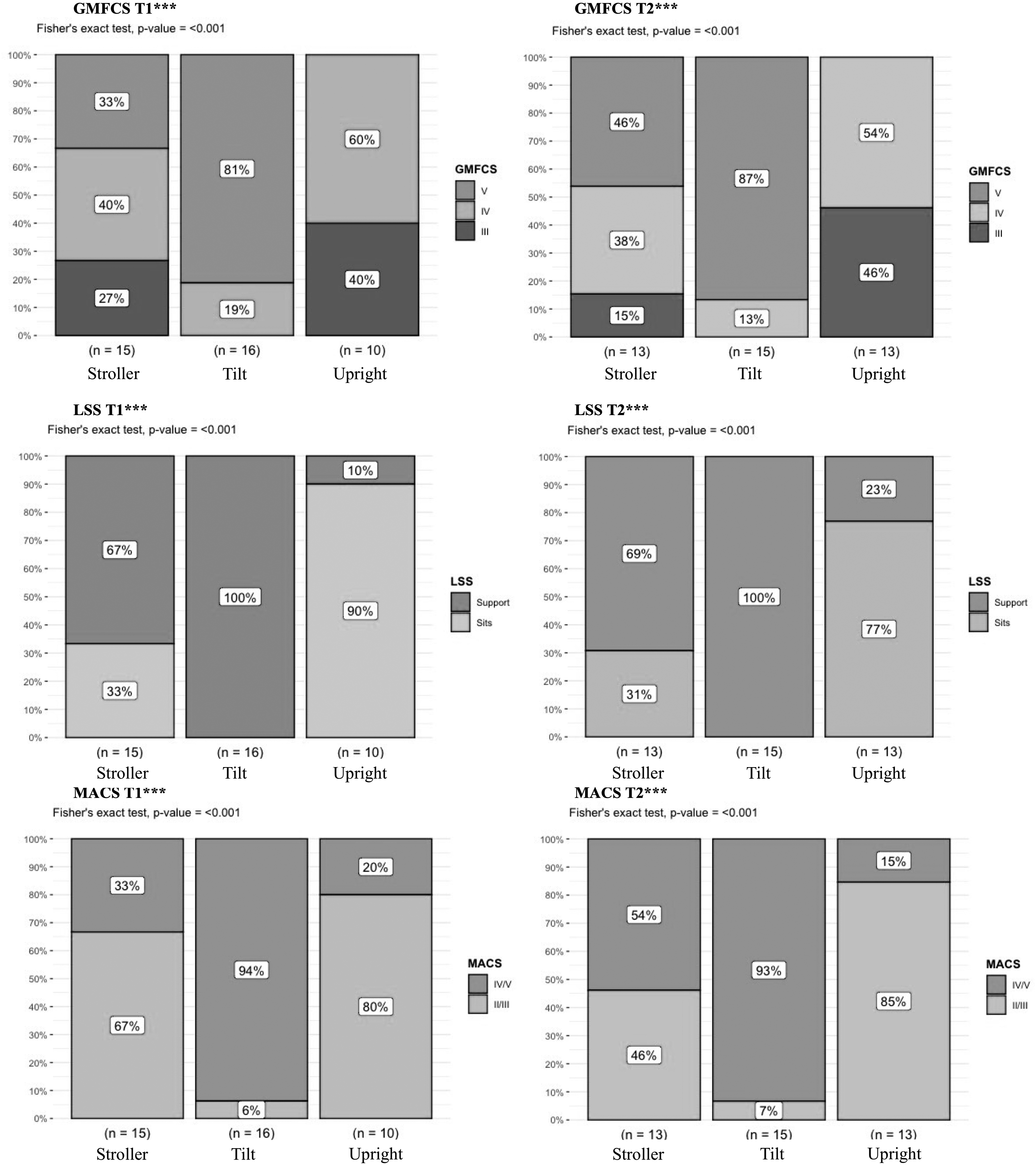
Fisher's exact test results for associations between manual mobility and classifications.
Associations Between Classifications and Manual Mobility or Seating Device at Start and End of 6 Months.
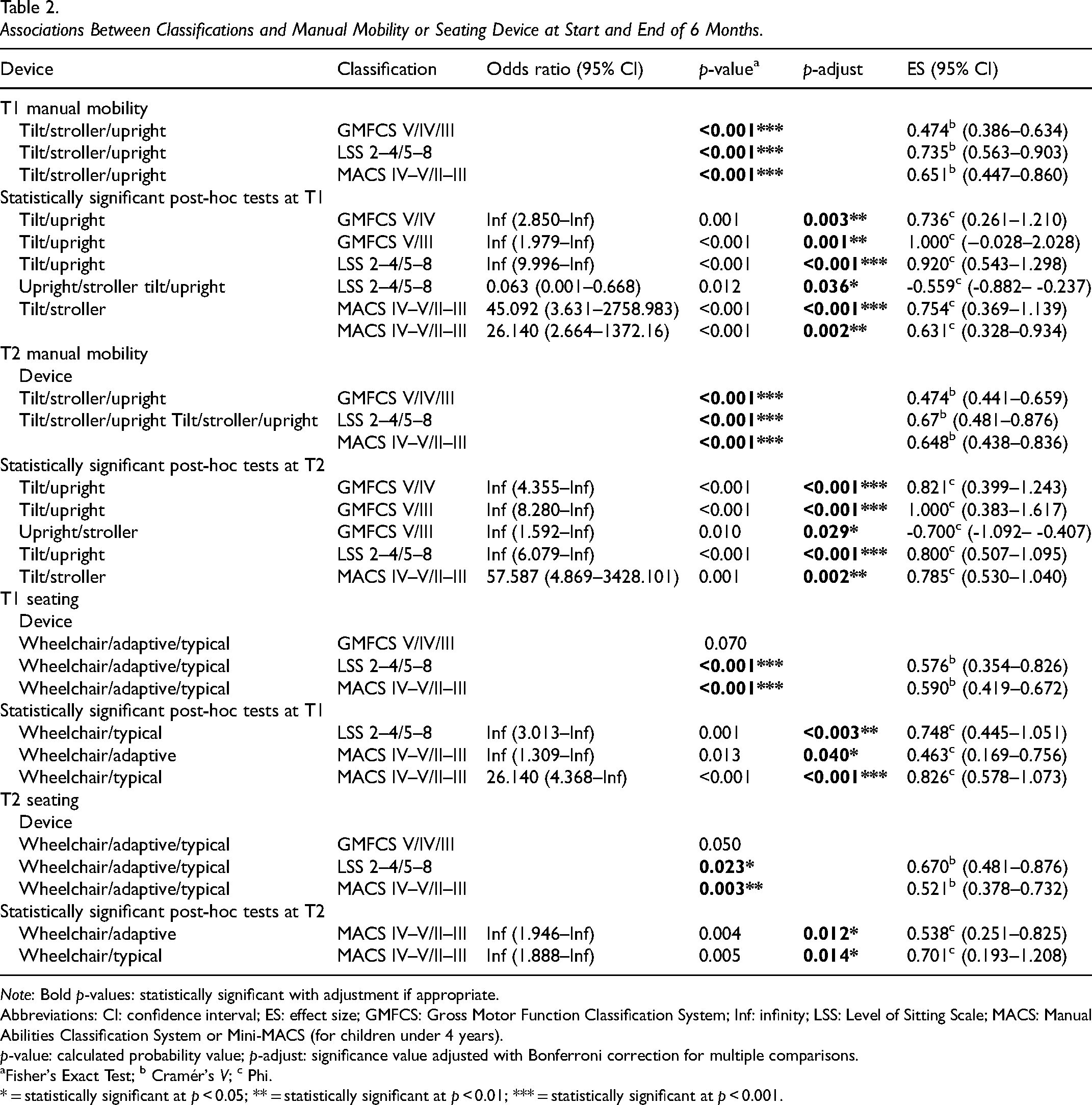
Note: Bold p-values: statistically significant with adjustment if appropriate.
Abbreviations: CI: confidence interval; ES: effect size; GMFCS: Gross Motor Function Classification System; Inf: infinity; LSS: Level of Sitting Scale; MACS: Manual Abilities Classification System or Mini-MACS (for children under 4 years).
p-value: calculated probability value; p-adjust: significance value adjusted with Bonferroni correction for multiple comparisons.
Fisher's Exact Test; b Cramér's V; c Phi.
* = statistically significant at p < 0.05; ** = statistically significant at p < 0.01; *** = statistically significant at p < 0.001.
Table 2 and Figure 3 illustrate associations with use of adaptive seating. Children requiring support to sit (LSS 2–4) were more likely to use the seating within their manual mobility device as their primary seating device, rather than typical high chairs or booster seats. Although differences were statistically significant overall, post-hoc tests were only significant at T1. Significant associations and large effect sizes were found for manual abilities in post-hoc tests at both time-points among wheelchair seating and adaptive seating, as well as among wheelchair and typical seating devices.
Fisher's exact test results for associations between adaptive seating and classifications.
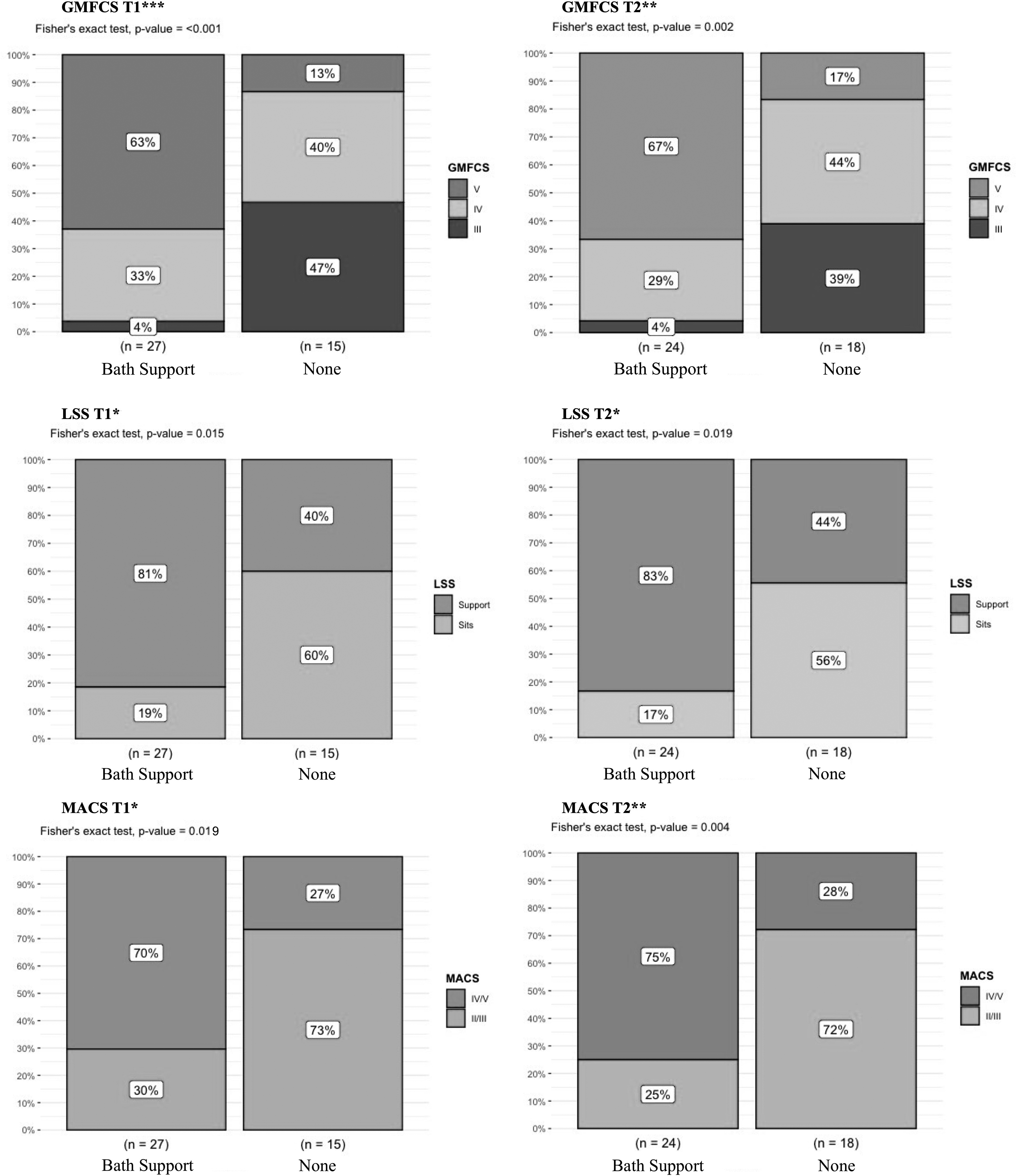
Figure 4 illustrates children's use of personal hygiene devices. Although more impaired functional levels, for all classifications, were significantly associated with use of a bathing device, GMFCS showed the strongest association (T1: p < 0.001; Cramér's V = 0.592; T2: p = 0.002; Cramér's V = 0.553). Most children at GMFCS V used bathing devices, while almost all children at GMFCS III could sit independently in the tub.
Fisher's exact test results for associations between bathing device and classifications.
In contrast, GMFCS was the only classification associated with use of toileting devices, at T2 only (p = 0.028; Cramér's V = 0.441; 95% CI 0.153–0.765) and post-hoc tests were not significant. Supplementary Appendix S1 details associations with classifications for all devices.
Time spent using devices ranged from 15 min to ≥6 h in manual mobility or seating devices with most time spent in tilt-in-space wheelchairs by children who used wheelchair seating as their only form of adaptive seating device. Time spent using bathing and toileting devices was fairly evenly distributed between ≤15 min, 16–30 min, and ≤60 min, with 16–30 min slightly more reported. Time using power mobility devices ranged from 15 min to 3 h with ≤60 min being most common at both time-points, and no statistically significant difference between T1 and T2 (McNemar test χ2 = 4, df = 3, p = 0.289).
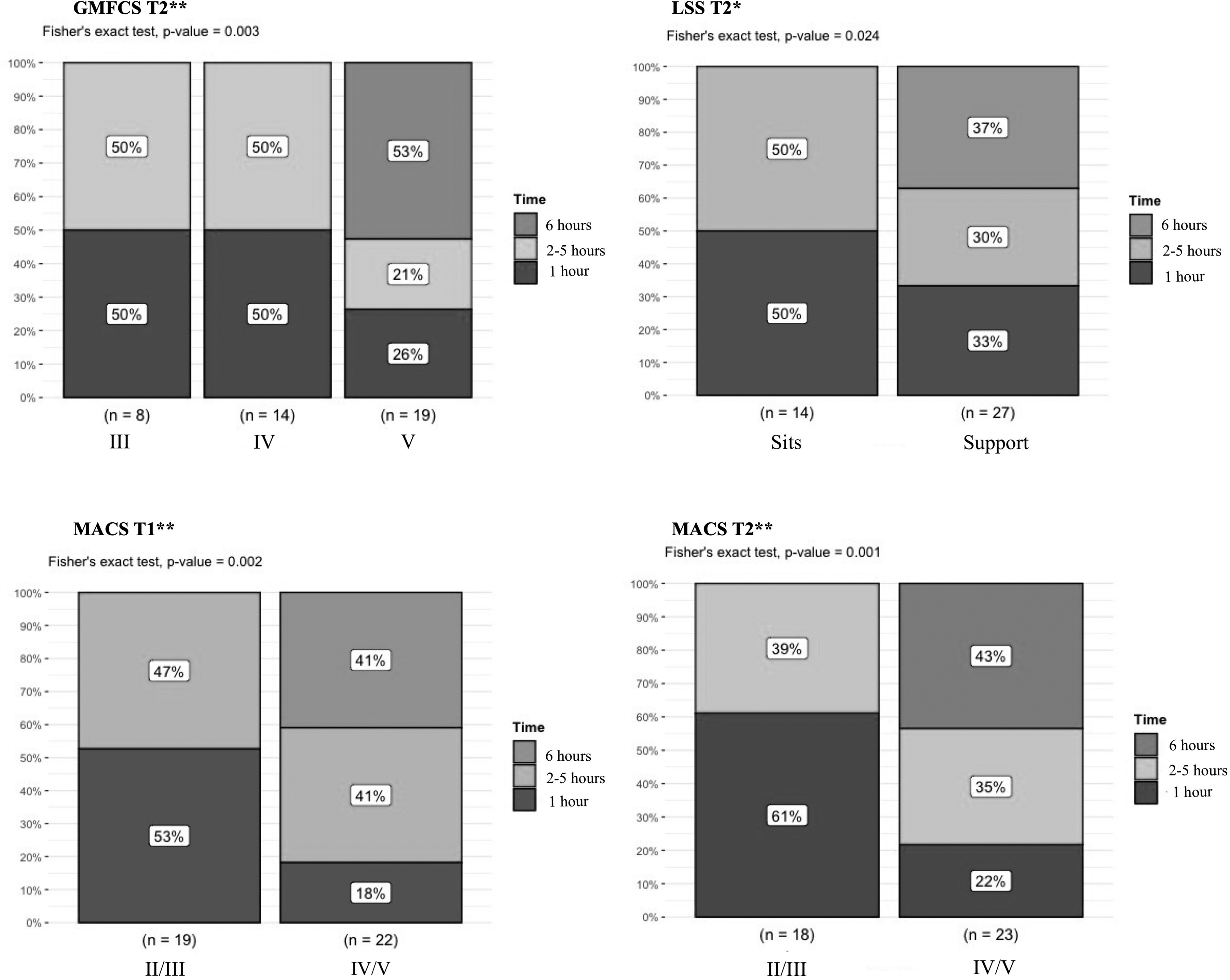
Figure 5 illustrates statistically significant associations between time in manual mobility and classifications. GMFCS and LSS were statistically significant at T2 only, while MACS was significant at both time-points. Post-hoc tests found significant differences, with large effect sizes (Phi = 0.624–0.674), between heavy and moderate use, and heavy and light use for children classified as GMFCS V in comparison to GMFCS IV. Similarly, differences were measured between children able to sit, and those requiring support with medium to large effect size (Phi = 0.48–0.509). For manual abilities, differences between heavy and moderate use, and heavy and light use were measured at T1 with medium (Phi = 0.5) to large effect sizes (Phi = 0.703), while at T2, differences were only statistically significant between moderate and light use with large effect size (Phi = 0.677).
Fisher's exact test results for significant associations between time using manual mobility devices and classifications.
Supplementary Appendix S2 provides details of all analyses between time and GMFCS, LSS, and MACS classifications, and between time and device-type. Time using seating devices was statistically significant only for GMFCS and MACS at T2. Few children used adaptive seating ≥6 h, and heavy use was reported primarily for children using seating devices only within manual wheelchairs. Differences were seen between light and moderate seating device use for children classified as GMFCS V versus III, and between MACS II–III versus IV–V with large effect sizes (Phi = 0.822 and 0.553, respectively).
There were no statistically significant differences between time children spent using adaptive seating devices or high-chairs/booster seats, and no associations between seated postural control and time using adaptive seating devices. When comparing time spent using manual mobility devices or adaptive seating and power mobility devices, there were no statistically significant associations between time at either T1 or T2.
Supplementary Appendix S3 provides details of time change analyses. Time change in manual mobility was associated with time change in power mobility (p = 0.012), but time change in adaptive seating devices was not (p = 0.56). The full dataset may be found in Supplementary Appendix S4.
Discussion
Based on 42 parent reports of device-use for 35 individual children, this study provides preliminary data illustrating the complexity of children's profiles and differences in their use of wheeled mobility, adaptive seating and personal hygiene devices. Results addressing our primary aim suggest that child age, gross-motor function, and manual abilities were statistically significantly associated with the choice between a stroller, upright, or tilt-in-space wheelchair, while age, postural control, and manual abilities were associated with the choice between wheelchair-based or other seating devices. Few children used toileting devices limiting analyses; however, more impaired gross motor abilities were associated with use of a bathing device across the age-span.
Clinical significance of time analyses addressing our secondary aim was less clear although, overall, children with more impaired abilities spent more time using devices. Time spent using manual mobility devices was statistically significantly associated with more impaired gross-motor, postural control, and manual abilities at T2, but only with manual abilities at T1. Heavy use of adaptive seating was seen primarily for children who used seating within their tilt-in-space wheelchairs influencing analyses. Although this study describes community-based provision, results suggest an appropriate match since more supportive mobility and positioning devices were used by children with greater functional limitations. Children required multiple devices, appropriately matched to their functional profile, in order to participate and engage in meaningful activities.
As a therapeutic intervention, modifying the physical environment through use of appropriate assistive devices is considered a compensatory, environmental, or context-focused approach; and is increasingly recommended for children with nonambulant CP (de Campos et al., 2024; Novak, 2014; Novak & Honan, 2019), with early introduction to take advantage of neuroplasticity. An appropriate match (between the child, caregiver, and environment) is essential, and devices that parents value as having a positive influence on both the child's participation and family life, are more likely to be used (Benedict et al., 1999). Manual mobility device-type was associated with GMFCS level, seated postural control and manual abilities. Upright wheelchairs were primarily used by older children at GMFCS III or IV, while younger children used strollers. Tilt-in-space wheelchairs were primarily used by children at GMFCS V and almost half used supportive seating devices only within this mobility device at T2. These findings are in line with illustrations (Version 2) created to accompany the GMFCS descriptors (https://canchild.ca/system/tenon/assets/attachments/000/002/114/original/GMFCS_English_Illustrations_V2.pdf). A study of adults with CP confirmed that almost all classified at GMFCS V used tilt-in-space wheelchairs, while those at GMFCS III and IV were more likely to use upright styles (Rodby-Bousquet & Agustsson, 2021).
In a Norwegian study, parents of 12–81-month-old children with CP reported that while both manual wheelchairs and adaptive strollers enhanced participation in daily activities, manual wheelchairs increased functional abilities, while strollers eased care (Moen & Østensjø, 2023). In our study, children with better manual abilities were more likely to have a lightweight, upright manual wheelchair, while those with more impaired function were more likely to have a tilt-in-space wheelchair. However, children's ability to self-propel was not measured, nor were parents asked about level of independent use. It is likely that most children were primarily pushed by others, particularly outdoors, regardless of wheelchair style as has been reported in other studies (Noten et al., 2024; Rodby-Bousquet et al., 2016). Wheelchair style may relate more to postural support needs, since more impaired LSS levels have been associated with greater use of external postural supports in the wheelchair (Field & Roxborough, 2012).
An older survey study from the United Kingdom suggested that parents are reluctant to transition their child from a stroller to a wheelchair even by school-age (5 years), with concerns about transportation, maneuverability, and space in the home (Shahid, 2004). However, in our study, less than half used strollers as their primary mobility device, and tilt-in-space wheelchairs were introduced before 2 years. In the Nordic countries, one study reported manual wheelchair use by 44% (122/277 GMFCS I–V) under 4 years, and 41% (212/517 GMFCS I–V) under 5 years (Rodby-Bousquet et al., 2016). These differences may relate to funding availability, differences in cultural or societal attitudes, or perhaps to practice changes over time.
In our study setting, funding is typically available for only one adaptive seating device. These may be transferred between a manual wheelchair and an indoor activity base or chair, perhaps influencing parent use of a wheelchair at an earlier age. Lightweight, self-propelling wheelchairs are typically funded for children with potential to self-propel, however parental preference may also relate to ease of use, transportation, aesthetics, and/or acceptance of their child's condition. A tilt-in-space wheelchair may be used only when the child cannot be comfortably supported in a lighter, upright wheelchair.
Seated postural control and manual abilities were associated with type of seating. Typical high-chairs or booster seats were used by children who could sit independently and those who required support. They were used more by children at GMFCS IV and those with better manual abilities, suggesting that children with more impaired manual skills, are not able to use their hands unless provided with more supportive adaptive seating devices. For the young children in our study, parent choice to use seating devices only within the wheelchair may reflect: challenges in transferring the child; difficulties in transferring seating devices to other bases; need for adjustable tilt-in-space for different activities; the complexity of seating required; and/or funding limitations. Adults with CP primarily use seating within the wheelchair rather than separate adaptive seating devices due to transfer challenges (Rodby-Bousquet & Agustsson, 2021).
Parents of young children with CP have prioritized participation and efficiency in self-care and mobility, with eating being highest priority for children at GMFCS IV–V, followed by dressing, toileting and bathing (Chiarello et al., 2010). In our study, large numbers used typical high chairs for eating and drinking, and adaptive floor seating devices for play, while more children used bathing than toileting devices. These differences may relate to our younger sample.
Across our study's age span, bathing devices were predominantly used by children with more impaired abilities. Other than at older ages, children with more impaired abilities were less likely to use toileting devices. A survey study suggested that children classified at GMFCS IV–V may master toilet training around 5–6 years, compared to 3 years in children who are typically developing. However, as with our study, most children at GMFCS IV–V wore pull-ups/diapers (O'Shea et al., 2018). Another study suggested that adaptive toileting devices may be useful for play and grooming activities in the bathroom, even for children not yet toilet training (Rigby et al., 2009; Ryan et al., 2009). GMFCS level has been suggested as the strongest predictor of independence in bathing or toileting, with age and learning difficulties influencing abilities (Østensjø et al., 2007), similar to our study findings. A toileting pathway for children with CP recommended starting around 48 months, considering cognitive and behavioral as well as postural and motor control factors; with toileting devices recommended for children unable to sit hands-free for 10 min (Millard et al., 2013).
In addressing our secondary objective, time in device was only associated with manual mobility device use. Change in time using manual mobility and power mobility devices was also associated, and may be linked to more children using manual wheelchairs at T2, rather than strollers. Children who used tilt-in-space wheelchairs spent more time using them than children using upright wheelchairs or strollers. However, children using tilt-in-space wheelchairs were also more likely to be using these, not only as a mobility device, but as their primary seating device, explaining the heavy use (≥6 h). School-aged children with CP spend an average of 11 h daily in wheelchairs with supportive seating (Lacoste et al., 2009), while adults with CP typically spend 8–12 h in wheelchairs (Rodby-Bousquet & Agustsson, 2021). In our study, there were no statistically significant differences between time spent in typical high chairs or booster seats and other adaptive seating devices, other than adaptive seating within the manual wheelchair.
In the initial HUTCH study (Ryan & Campbell, 2009), including 12 children (GMFCS III–V) aged 4–10 years, parents recorded device use over 7 consecutive days, and repeated this process 2–3 weeks later. Moderate manual wheelchair use was reported by 67–50%, and >6 h by 8.7–15%. In contrast, based on parent-estimated use over the previous 7 days, 24% in our study used their manual wheelchair for ≥6 h, 36% reported moderate, and 38% reported light (≤1 h) use. Similar to Ryan and Campbell's study, moderate use of adaptive seating was most commonly reported; 71–40% in comparison to 41–50% in our study, and bathing and toileting devices were used by all children for ≤1 h daily.
Differences may be explained by their smaller population, which was balanced between the three GMFCS levels (III–V), in comparison with the larger, younger and more complex population in our study. In addition, HUTCH authors’ participants recorded device use only at home for their predominantly school-aged sample, resulting in variability between weekends and school days. Results may also have been influenced by provincial funding differences, being conducted in two different Canadian provinces.
Consideration should also be given to the social and attitudinal environments (Anaby et al., 2017), as use of devices is influenced by parents and caregivers’ attitudes and needs. Acceptance of motor development prognosis and the consequent need for assistive devices that may cause others to perceive their child as being different may be challenging for parents of children with CP, GMFCS III–V (Bailes et al., 2018). These children are interdependent with parents and caregivers, and the selection and use of assistive devices is influenced by everyone interacting with, or assisting the child using the device (Paleg et al., 2024). Assistive devices may promote occupational participation by addressing needs for both child and family autonomy (e.g., for mobility, exploration, play, self-efficacy, community participation, etc.), competence (e.g., learning, education, independent mobility, communication, etc.), and relatedness with family, peers, friends, community, and wider society (Egan & Restall, 2022). Again, referencing the Canadian Model of Occupational Participation (Egan & Restall, 2022), in terms of health systems, families may require support to fund and access the assistive devices needed to assist with care and mobility for their child (Lahaije et al., 2023).
Following are some examples of how assistive devices may promote occupational participation for young children with nonambulant CP: a manual wheelchair may allow a child and their family access to the occupation of going on a family outing or walk; a bathing device may allow parents or caregivers to bathe a child safely, and allow the child to play in the water (at home or in the community); an adaptive seating device may facilitate trunk, head or upper limb control, and allow a child to initiate engagement in a play activity with siblings, or participate in family meals; and a supportive seating device within an appropriate mobility device may allow a child to participate and sustain engagement in a preschool program with peers, rather than being held or carried by adults.
Limitations
Generalizability may be limited since study results reflect prescription practices and funding limitations within one Canadian province. However, the range of urban, suburban, rural, and remote settings for included children (and the therapists that support them) may increase applicability of results to other settings. Although the type of manual mobility device and the time spent in that device were recorded, the level of independence or ability to self-propel wheelchairs designed for self-propulsion was not known for our sample. Due to limited numbers classified as GMFCS III, it was not possible to dichotomize GMFCS into more and less impaired. Our sample size overall influenced post-hoc analyses and was insufficient for more complex statistical analyses.
Although the HUTCH survey used was an earlier research version, there were no significant changes for the manual wheelchair and adaptive seating device sections. Estimates of device use over the previous week are subject to recall bias; however, we chose not to increase parent burden by asking them to document device use in a daily activity log. The original 6-point scale was modified to reduce likely floor effects for time using toileting and bathing devices. These modifications may have influenced reliability of results; however, statistically significant differences between the three device categories are unlikely. Time using adaptive seating within the manual wheelchair was analyzed under manual mobility and could not be separated, influencing adaptive seating device time results.
A mixed-methods approach would have been ideal to explore parental beliefs and values about the use of devices and reasons for outliers. Future prospective studies, with larger samples and more even representation among classification levels, should include qualitative and quantitative data to advance knowledge about factors influencing decision-making. In addition to child profile and functional classification influences, future research could further explore barriers and facilitators of device choice and use, such as physical, social, and attitudinal environmental factors, including funding and device provision environments.
Conclusions
Our analysis of parent-reported data for young children with CP, GMFCS III–V showed that: age, gross-motor function, and manual abilities were statistically significantly associated with choice between manual mobility devices; age, postural control, and manual abilities were associated with choice between wheelchair or other seating devices; and more impaired gross motor abilities were associated with use of a bathing device. Results suggest that children with limited mobility and postural control use multiple positioning and mobility devices as they engage in meaningful occupational participation.
In our study, most children functioning at GMFCS V used tilt-in-space wheelchairs, while children at GMFCS III and IV over 3 years old mainly used upright wheelchairs. Choice between a stroller and a wheelchair was influenced by child age, as well as gross motor and manual abilities. Children who required support to sit were more likely to use adaptive seating devices, while those with the most limited postural control and manual abilities were more likely to use supportive seating devices only within tilt-in-space wheelchairs. GMFCS level was most associated with use of bathing devices across the age span of the study, while the majority of children were dependent for toileting. Children with more impaired functional abilities spent greater amounts of time using adaptive seating and mobility devices, suggesting that parents found the devices useful to promote occupational participation and/or ease caregiving. Study findings provide evidence confirming associations between devices used and functional classifications that were previously assumed in clinical practice.
Key Message
Children 18 months to 7 years classified at GMFCS III–V use a variety of positioning and wheeled mobility devices to enhance daily functioning and facilitate engagement in occupational participation. Child profile, including age, gross motor, manual, and seated postural control abilities, influence choice and selection of different types of manual mobility, seating, toileting, and bathing devices, as well as time spent using these devices.
Supplemental Material
sj-pdf-1-cjo-10.1177_00084174261421406 - Supplemental material for Wheeled Mobility, Seating, and Bathroom Device Use by Children With Cerebral Palsy
Supplemental material, sj-pdf-1-cjo-10.1177_00084174261421406 for Wheeled Mobility, Seating, and Bathroom Device Use by Children With Cerebral Palsy by Roslyn W. Livingstone and Debra A. Field in Canadian Journal of Occupational Therapy
Supplemental Material
sj-pdf-2-cjo-10.1177_00084174261421406 - Supplemental material for Wheeled Mobility, Seating, and Bathroom Device Use by Children With Cerebral Palsy
Supplemental material, sj-pdf-2-cjo-10.1177_00084174261421406 for Wheeled Mobility, Seating, and Bathroom Device Use by Children With Cerebral Palsy by Roslyn W. Livingstone and Debra A. Field in Canadian Journal of Occupational Therapy
Supplemental Material
sj-pdf-3-cjo-10.1177_00084174261421406 - Supplemental material for Wheeled Mobility, Seating, and Bathroom Device Use by Children With Cerebral Palsy
Supplemental material, sj-pdf-3-cjo-10.1177_00084174261421406 for Wheeled Mobility, Seating, and Bathroom Device Use by Children With Cerebral Palsy by Roslyn W. Livingstone and Debra A. Field in Canadian Journal of Occupational Therapy
Supplemental Material
sj-pdf-4-cjo-10.1177_00084174261421406 - Supplemental material for Wheeled Mobility, Seating, and Bathroom Device Use by Children With Cerebral Palsy
Supplemental material, sj-pdf-4-cjo-10.1177_00084174261421406 for Wheeled Mobility, Seating, and Bathroom Device Use by Children With Cerebral Palsy by Roslyn W. Livingstone and Debra A. Field in Canadian Journal of Occupational Therapy
Footnotes
Acknowledgments
This work was supported by Jeffrey Bone, Biostatistical Lead, Clinical Support Unit, BC Children's Hospital Research Institute, who provided consultation on statistical methods.
Contributions
Roslyn W. Livingstone designed the study, completed the statistical analysis, and wrote the first draft of the manuscript with consultation from Debra A. Field. Both authors reviewed and refined tables, figures, appendices, and manuscript for publication and are in agreement with the final version.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: HUTCH data collection was completed by the authors as part of the larger pre-post power mobility study supported by Sunny Hill Health Centre for Children. Time to complete this portion of the analysis and write the manuscript was unfunded.
Data Availability Statement
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.