
Abstract
Background
In occupational therapy with children, the therapeutic relationship is a fundamental and complex component. However, for a long time, little was known about how children experienced the therapeutic relationship. New findings about children's experiences offer valuable insights for occupational therapists to reflect upon.
Purpose
This study aimed to explore occupational therapists’ perspectives on their therapeutic relationships with children, building on emerging evidence from children's experiences.
Method
A qualitative interpretive description design was used, involving four 1-hr online focus groups with a total of 29 occupational therapists from Québec (Canada). Data were analyzed using an interpretive approach outlined by Baribeau to identify emerging themes.
Findings
Three key themes were developed: (a) the therapeutic relationship is an important process shaped by occupation and collaboration with families and partners; (b) children are often excluded from decision-making and have limited opportunities to share their views within the therapeutic relationship; and (c) the relationship can be improved through strategies such as supporting children's expression of their emotions and perspectives and following their lead.
Conclusion
The emerging evidence from children's experiences has prompted important reflections among participants. A key reflection concerns the importance of creating space for children's active participation and expression within the therapeutic relationship.
The therapeutic relationship plays a central role in effective rehabilitation services. Studies have linked a positive relationship to increased client satisfaction, greater interest in the therapeutic process, and stronger engagement and adherence to therapy (Hansen et al., 2024). From the client's perspective, the relationship fosters trust and makes services feel more personalized (Heredia-Callejón et al., 2023). Moreover, it improves functional outcomes and enhances both the physical and mental health of clients (Alodaibi et al., 2021; Hall et al., 2010).
The therapeutic relationship, initially conceptualized within the field of psychology, has been defined in various ways in the literature. In this article, we adopt Bordin’s (1979) definition because it is widely recognized and aligns well with the context of rehabilitation (Morrison & Smith, 2013). Bordin defines the therapeutic relationship, which he terms the therapeutic alliance, as a collaborative and trusting bond between a therapist and a client. It involves the development of trust rooted in reciprocal positive regard. This definition is unique in that it encompasses both a shared agreement regarding intervention goals and a mutual understanding of the tasks and strategies necessary to achieve those goals. In occupational therapy, these tasks and strategies are grounded in meaningful occupations. This relationship is thus uniquely shaped through the client's engagement in these occupations, positioning occupation as the vehicle through which the relationship is built (Taylor, 2020).
In occupational therapy with children, the therapeutic relationship involves multiple stakeholders, including the child and their parents. While the importance of building a positive therapeutic relationship with parents is well established (D’Arrigo et al., 2020; McCarthy & Guerin, 2022), forming this relationship with children is equally essential. Such a relationship allows children to feel heard and promotes meaningful communication (Gagné-Trudel et al., 2024). The relationship between children and their therapist also contributes to their engagement in therapy (King et al., 2020).
The therapeutic relationship in occupational therapy with children has largely been examined from an adult-centric perspective, emphasizing the views of parents and occupational therapists. For example, McLean (2019) explored the association between families’ and occupational therapists’ reports of the therapeutic relationship, as well as the correlation of these reports with variables such as adherence and treatment outcomes. Her study involved parents (n = 25) and occupational therapists (n = 4). Similarly, McAnuff et al. (2015) sought to identify instances of relational and participatory interactions between families and therapists within occupational therapy. Their data comprised 217 self-reported therapeutic actions from occupational therapists. Numerous other studies have investigated the therapeutic relationship exclusively through the perspective of adults (e.g., Kruijsen-Terpstra et al., 2014; Pereira & Seruya, 2021; Wiart et al., 2009). This focus reflects an adult-centred paradigm in research in occupational therapy with children, wherein understanding is shaped predominantly by adult norms and interpretations (Tourigny & Lafantaisie, 2022). This prevailing adult-centred paradigm underscores a critical gap in the occupational therapy literature: the lived experiences of children remain largely unexplored.
In response to the need to better understand children's own lived experiences of the therapeutic relationship, a recent phenomenological study explored how children perceive their relationship with their occupational therapist (Gagné-Trudel et al., 2026). Fourteen children, between the ages of 2 and 10 years, reported a range of experiences. Several participants described positive aspects of the therapeutic relationship, including a sense of trust fostered by humour, feeling understood in relation to their everyday challenges, and shared meaning in the occupations addressed during therapy. Others reported feeling misunderstood, inadequately supported in facing difficulties, or overwhelmed by challenging emotions they kept to themselves. Such relational challenges affected how engaged children felt during therapy and limited their acknowledgement as active participants in their therapeutic journey. Across their experiences, one conclusion stands out: children expressed a strong desire to be heard, understood, and actively engaged in therapy activities that align with their interests and goals.
Previous literature has explored occupational therapists’ perspectives on building therapeutic relationships with parents and children. Now that new research findings have been developed regarding children's experiences of this relationship, it would be relevant to revisit occupational therapists’ perspectives to understand how they respond to these insights. Accordingly, this research aimed to examine how occupational therapists interpret and respond to children's lived experiences of the therapeutic relationship, building on emerging evidence from children's experiences.
Method
A qualitative interpretive description research design was chosen (Thompson Burdine et al., 2021). This design from health sciences is well suited to the present study, as it facilitates an in-depth exploration of participants’ perspectives and how they make sense of real-life situations, particularly in relation to their professional practice (Miaux & Roult, 2023; Thompson Burdine et al., 2021). This study received research ethics approval from Centre intégré universitaire de santé et de services sociaux de la Mauricie-et-du-Centre-du-Québec (MP-29-2024-754,955) and Université du Québec à Trois-Rivières (CER-24-312-10.02).
Participants
To be eligible, participants had to be occupational therapists working with children, regardless of their practice setting, in Québec (Canada). This was the only inclusion criterion, and there were no exclusion criteria. Participants were recruited using a volunteer-based approach (Pires, 1997). They were recruited via posters shared in online professional communities, newsletters, and an invitation email circulated within a healthcare institution. Occupational therapists interested in participating in the research could fill in the online consent form by scanning a QR code on the posters. A total of 34 occupational therapists were recruited; four cancelled due to a change in availability, and one did not show up, resulting in 29 participants.
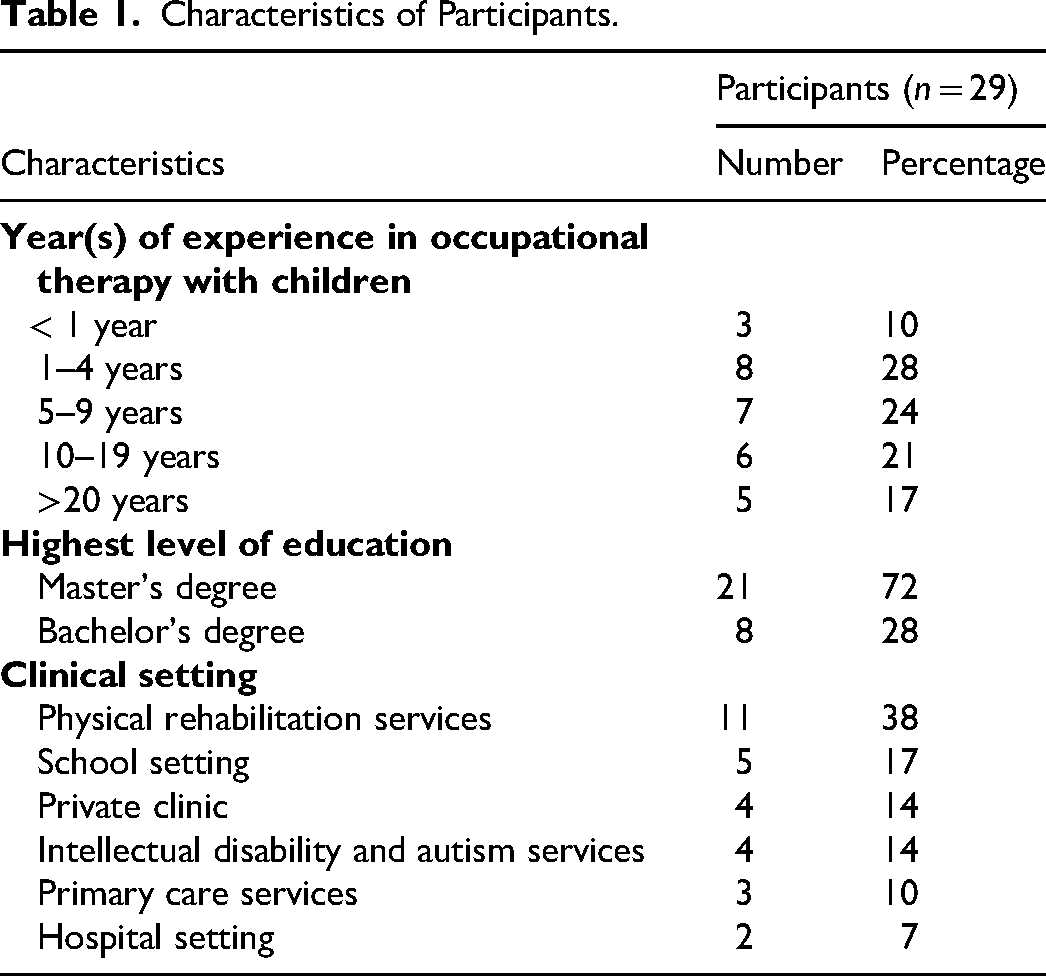
All 29 participants were women. They worked in 12 of Québec's 17 administrative regions, with the three most represented regions being Mauricie, Montreal, and Lanaudière. Participants represented diverse clinical settings, education levels, and years of professional experience, as shown in Table 1.
Characteristics of Participants.
Data Collection
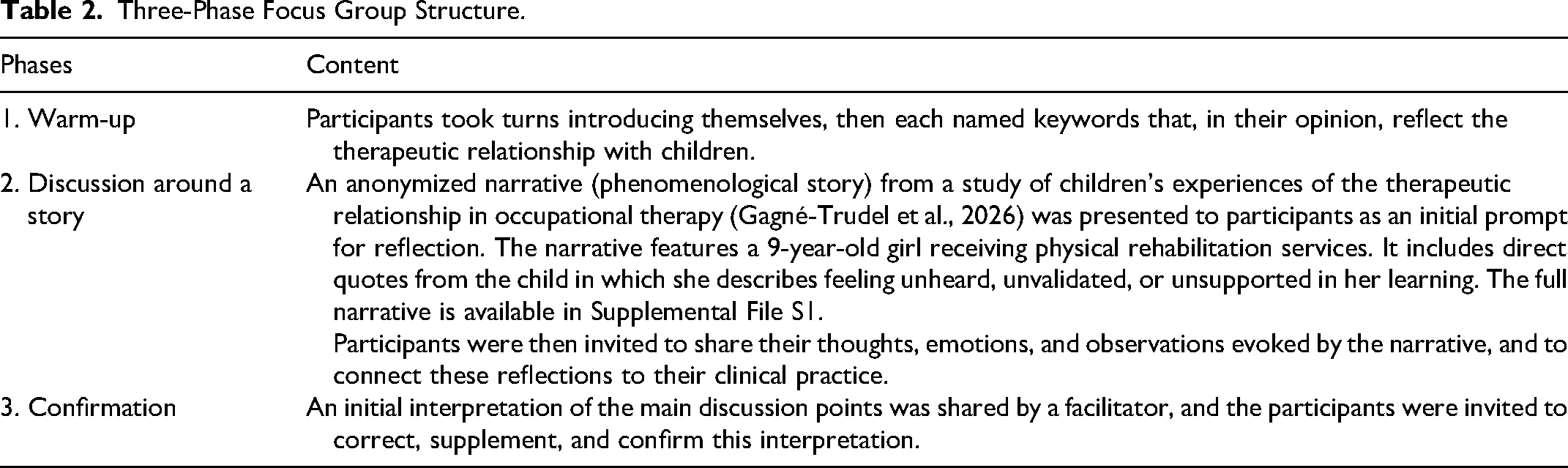
Four 1-hr online focus groups, each composed of seven to eight occupational therapists, were conducted. Focus groups are suited to interpretive descriptive designs, as they facilitate an exploration of participants’ perspectives while capturing the diversity of viewpoints (Davila & Domínguez, 2010). All focus groups were conducted in French and video-recorded. The focus groups were co-facilitated by two moderators (a researcher with extensive experience in group facilitation and a doctoral candidate with experience in occupational therapy with children) following a pre-established script. The discussion was structured in three phases (Davila & Domínguez, 2010), as illustrated in Table 2. To characterize the sample, participants were also asked to complete an online questionnaire regarding their clinical practice.
Three-Phase Focus Group Structure.
Data Analysis
Sample descriptive statistics were used to analyze the data collected with the online clinical practice questionnaire. The group data were analyzed using the interpretive approach for focus group data outlined by Baribeau (2009). In interpretive description, codes are generated inductively, an approach that Baribeau's method supports (Thompson Burdine et al., 2021). All stages of the analysis were led by the first author. Verbatim transcripts of the focus groups were first prepared, and all transcripts were anonymized using pseudonyms. Initial readings were conducted, and spontaneous reflections were documented in a reflexive journal. An initial round of open coding, staying as close as possible to participants’ own words, was then performed using NVivo 15. Similar codes were grouped into broader categories, each defined by a descriptive statement. Throughout the coding process, the reflexive journal was maintained to capture ongoing reflections. In parallel, a separate analysis of interactions within each focus group was conducted, focusing on how participants’ positions and nuances evolved within each category before and after the presentation of the child's narrative. This analysis was carried out using Word documents with colour coding and arrows. Based on the combined analysis of both the thematic categories and the interactional dynamics, overarching themes were co-constructed collaboratively by the first and second authors, using concept maps as a tool. By iteratively reviewing the concept maps, interaction analyses, and transcripts, these themes were then drafted into text to produce the final synthesis. They were verified and validated by the second and third authors. For the final synthesis, the themes, sub-themes, and quotes were translated from the original French.
Findings
The findings can be grouped into three overarching themes that illustrate how participants interpreted and responded to children's lived experiences of the therapeutic relationship. The first theme focuses on the participants’ understanding of the therapeutic relationship in occupational therapy. It provides a conceptual foundation, offering insight into the assumptions that shape how participants approach and interpret the therapeutic relationship, before being presented with a child's narrative (first phase of the focus group). The second theme focuses on participants’ reflections about how they build relationships with children during therapy in response to the child's narrative, as articulated during the second phase. The third theme highlights strategies proposed by participants to strengthen the therapeutic relationship with children, based on their reflections. Figure 1 illustrates the themes, subthemes, and the links between them.
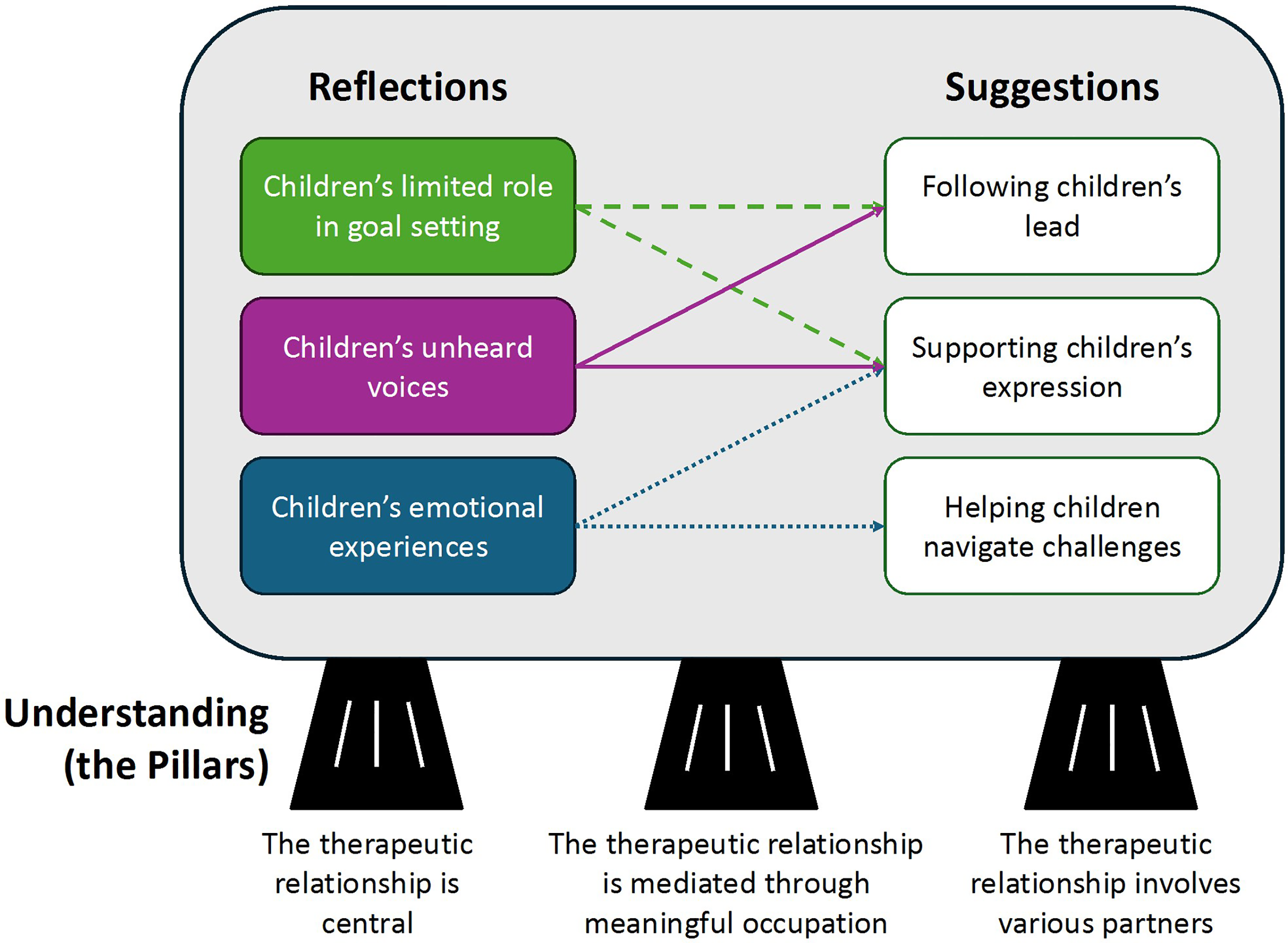
Thematic map. Note. This figure illustrates the themes and sub-themes related to participants’ views of the therapeutic relationship with children. The pillars represent their understanding of the therapeutic relationship. Participants’ reflections on building this relationship informed the identification of strategies to strengthen it, as indicated by the arrows.
Understanding of the Therapeutic Relationship With Children
The participants’ understanding of the therapeutic relationship with children can be divided into three sub-themes: (a) they viewed the therapeutic relationship with children as a central component of their practice; (b) they emphasized that this relationship is mediated through occupation; and (c) it involves various partners, including children, parents, and other stakeholders such as teachers and daycare educators.
The Therapeutic Relationship Is Central
The participants emphasized that the therapeutic relationship is both “central” and “a priority” in the context of interventions with children, regardless of the child's age. Participants described how the relationship not only fosters children's engagement in therapy but also serves as a meaningful connection in their broader life. To discuss the relationship, Marie-Ève (Group 4) used the metaphors of a toolbox and a house to illustrate its crucial role in fostering children's engagement while also creating a secure environment: I think engagement [is linked] with the therapeutic relationship. […] It's a tool in our toolbox that we want to use to improve engagement. […] The relationship is [also] like a house, just like a child needs a secure base to explore and develop their skills. That feeling of safety is essential.
The Therapeutic Relationship Is Mediated Through Meaningful Occupation
Participants explained that the therapeutic relationship is mediated through occupation. It is through shared occupational experiences that the connection between therapists and children is built and strengthened. According to them, these occupations must be meaningful to the children, enjoyable, and offer a just-right challenge. In this excerpt, Sophie (Group 1) emphasized the importance of ensuring that occupations are meaningful to children: Every time I do [“classical OT activities”], I try to think: is this going to feel relevant to the child and the family? We need to ask ourselves whether we are doing it because we think that, at their age, they should be able to do it, or whether it is meaningful to the child.
The Therapeutic Relationship Involves Various Partners
Participants also underscored the distinctive nature of the therapeutic relationship in practice with children, emphasizing its multi-party structure. This relationship often extends beyond the child to include key stakeholders such as parents, daycare educators, and school-based teams. According to participants, interactions with these various stakeholders can complicate the therapeutic process, particularly when their goals and expectations diverge. Laurence (Group 3) illustrated this dynamic by stating: “In occupational therapy with children, there's an added challenge. The relationship isn’t just between two people. It's often tri-directional, involving, for example, a teacher or a parent.”
Reflections on Children's Experiences of the Therapeutic Relationship
Following the presentation of research findings in the form of a child's narrative describing her experience of the therapeutic relationship, participants expressed feelings of surprise, frustration, concern, and discomfort. The narrative prompted reflective discussions, during which participants drew connections with observations from their own clinical practice. These reflections underscored three sub-themes: (a) children's limited involvement in setting therapeutic goals; (b) the difficult emotions they may experience during therapeutic activities; and (c) the restricted opportunities they have to express their perspectives throughout the therapeutic process.
Children's Limited Role in Goal Setting
A strongly emphasized reflection among participants was that children play a limited role in selecting intervention goals, even though the goal setting was seen as an important factor in the therapeutic relationship to foster their self-determination, motivation, and engagement. Participants expressed discomfort and frustration upon realizing that, in the narrative, the child appeared to have no opportunity to participate in goal setting and was affected emotionally by this situation. At the same time, participants acknowledged that children's limited involvement in goal setting reflects the realities of clinical practice. Participants explained that they often relied on parents or other stakeholders to determine goals, a practice that may reduce the significance of therapy for children. Valérie (Group 1) shared this observation related to her practice: When it comes to parents’ goals, they are often framed like […] “She's always asking for help [with this task].” […] Sometimes, it's the parent's goal, and it doesn’t make sense for the child. But we usually go with the parent's goal anyway.
Participants emphasized that younger children played an even more limited role in goal setting. In many cases, they considered it challenging, or even unfeasible, for children to articulate meaningful goals. Nancy (Group 4) discussed the differences related to age: I realize that when children are younger, they are less involved in the choice of goals. It's often chosen with the parents. Sometimes, I'll ask them […] “Do you want to be better at cutting?” But older children […] are more involved in selecting goals.
Children's role in goal setting was also limited when the participants felt the parents had important goals to address, particularly within resource-constrained settings. In this context, they reflected on the meaningfulness of the goals being pursued, particularly when those goals are selected by the parents. Isabelle (Group 4) pointed out how parental priorities could overshadow children's perspectives in the therapeutic process: I know we’re supposed to listen to the child and select at least one goal that really matters to them. But with how limited our services are, it's hard to include a goal the child wants to prioritize. There are so many goals that adults around the child see as more important.
Children's Emotional Experiences
Participants emphasized that while the therapeutic relationship is fostered through engagement in occupations, the child's narrative deepened their reflection by highlighting that these occupations can be challenging for children. Participants realized that even seemingly simple tasks, such as tying shoelaces, can become emotionally charged moments for children in therapy. Laurie (Group 2) shared her reflection: Activities of daily living aren’t always the most engaging occupation. They’re often confronting, and this can be even more true for children. […] When the children are faced with two adults watching them struggle to tie their shoelaces, it puts a lot of pressure on them.
According to participants, the occupations addressed in occupational therapy can lead to anxiety in children. This anxiety was often linked to a fear of failure, particularly when children perceived the task as too difficult or felt pressure to succeed. When anxiety takes over, children may disengage from the activity, which limits their ability to learn and to connect with their occupational therapist. Manon (Group 3) shared this concern: The children may feel scared or anxious. If they’re afraid of failing or running out of time, it can create anxiety that isn’t helpful to achieve their goals. When children are too anxious, they’re not fully engaged in the present moment.
Children's Unheard Voices
As part of their reflections, participants also discussed that children are rarely invited to share their voices during therapy, which may limit their active participation. Participants acknowledged that their focus on their tasks may lead them to overlook children's experiences or preferences. This reflection was challenging for many participants, as they acknowledged that without actively inquiring into children's experiences, it becomes impossible to understand how they perceive the occupational therapy sessions, which can inevitably affect the therapeutic relationship. Sophie (Group 1) explained: We don't usually get this kind of feedback. I don't often ask: “Are you satisfied with the way things are going?” or “What are your daughter's emotions when she comes here?” If you just go by your “perceptions” of the relationship, [children] can pretend that they like it. […] So, all of this is shaking me up.
Participants noted that children's opportunities for self-expression may be limited unless intentionally supported, given that children do not always spontaneously articulate their emotions or perspectives regarding therapy. Considering the inherent power imbalance between therapists and children, children may feel hesitant to express themselves openly. Bianca (Group 2) reflected on this power imbalance: The child wasn't comfortable sharing […] I think that often happens because of the power difference between the therapist and the child. The therapist holds a position of authority, and that can make it challenging for children to feel safe enough to share how they’re feeling.
Some participants went further, suggesting that it is not only the lack of opportunities for children to express themselves, but also the absence of validation and demonstrated understanding toward children that can affect the therapeutic relationship. Ariane (Group 2) elaborated on this reflection: Perhaps the child didn't have the space to express that she didn't like it. But maybe it's also because we didn't validate her, and then we didn't show that we understood. Sometimes children name things, but adults quickly move on to other things. That's an issue that can affect the relationship.
Suggestions to Foster the Therapeutic Relationship With Children
Building on prior reflections, the discussions led to the identification of three key strategies aimed to strengthen the therapeutic relationship with children. These strategies are divided into three sub-themes: (a) supporting children's expression of emotions and experiences; (b) following their lead; and (c) helping them navigate the challenges inherent in the occupations addressed in therapy.
Supporting Children's Expression
In response to the reflections outlined earlier, participants emphasized the importance of supporting children's expression of their experiences and emotions to better understand their perspectives. They emphasized that children do not communicate solely through verbal language; therefore, supporting expression also requires careful attention to nonverbal cues. Sylvie (Group 3) described how she closely observes children's gestures to promote emotional safety and help them feel comfortable expressing their emotions, including those that may be unpleasant, by putting words to them: I tend to name what I see. Like, “Oh, you're turning away. Maybe you don't like that.” I try to help them put words to it. If I want us to have that trusting relationship, I need them to feel able to tell me how they feel.
Participants emphasized the importance of actively supporting children's expression, beginning from the very start of each session. Some described establishing routines that involve sitting with the child on floor cushions and taking time to check in, with the aim of understanding the child's emotional state. Karine (Group 1) explained how she integrates this practice not only at the beginning, but throughout the entire session: It's the first thing I address in sessions. How are you arriving? What state are you in? How do you feel? Where should we start? […] And every time we do an activity, I’m observing behaviours to see if the child is in the right state to engage. If not, that's what I focus on.
Following Children's Lead
Participants suggested that following children's lead, even at a young age, can enhance their participation within the therapeutic process. As illustrated by Manon (Group 3), when a child expresses disinterest in a given activity, acknowledging this response and offering alternative options aligned with the child's preferences can promote feelings of being heard: When a child isn’t motivated, we’re starting off with more difficulty. So, I say something like “You don’t feel like playing my game? That's okay, you can tell me.” This way, the child feels involved. Then I might say: “If you don’t want to play, help me put it away.” The goal is to keep children in a space of enjoyment, […] so they feel heard and involved.
Participants also emphasized the value of directly asking children about their goals whenever possible and incorporating them into the intervention plan. Involving children in goal setting was seen as a meaningful way to recognize their perspectives in the therapeutic relationship. From the participants’ perspectives, following children's lead may involve the therapist taking initiative to better understand children's interests and goals to align interventions with what matters to them. Participants described offering choices such as selecting the order of activities, choosing preferred games, integrating personal interests, and contributing to the planning of future sessions. An example came from Jennifer (Group 4), who described how she integrates children's goals or interests into her sessions: With younger children, […] I make sure they have some choices, like including their interests […] or letting them choose which games to play. […] This increases their engagement and motivation. It makes it more likely that the goals will be achieved.
Helping Children Navigate Challenges
Participants recognized that occupational therapy activities can present significant challenges for children and shared a range of strategies to support their engagement. These strategies included enhancing the enjoyment of activities, accompanying children through their difficulties and emotions, advocating to parents for goals adjustment, and considering group-based interventions. Noémie (Group 3) illustrated one of these strategies by highlighting the importance of fostering a sense of competence and success throughout the therapeutic process: The strength of the therapeutic relationship lies in being able to accompany the children in their difficulties […] Once we've made the child feel competent, acknowledged, and that they're experiencing success with this occupation, let's say cycling, then the child can continue practising [cycling] at home.
Participants also highlighted the importance of adapting occupational goals, which may involve negotiating compromises or advocating on behalf of the child with parents to ensure that the goals are suitably challenging. Laurence (Group 3) spoke to this strategy: There's a lot of work to be done with the parent to make them realize the scope of the activity, and what it requires of their child, and then perhaps readjust the goal. It's a challenge to make the parent more observant of their child, to better target goals that are a fair challenge for the child.
Discussion
This study aimed to examine how occupational therapists interpret and respond to children's experiences of the therapeutic relationship. Participants described the therapeutic relationship as essential, complex, and grounded in occupation. The complexity stems from the involvement of multiple stakeholders—such as parents and other therapists—whose goals and expectations may diverge. Within this dynamic, children's perspectives, particularly those of younger children, are at risk of being overlooked. Participants also reflected on the emotional responses children may experience when facing the inherent challenges of occupations targeted during therapy, noting that these reactions are often overlooked when therapists focus on completing the activity. In response to these observations, they proposed strategies to strengthen the therapeutic relationship and promote children's participation, including facilitating children's expression of their experiences and emotions, following their lead, and supporting them in navigating challenges.
Challenging the Adult-Centred Paradigm
The new insights into children's lived experiences elicited reactions of surprise and reflective introspection among participants. They were particularly struck by the emotional impact that therapy can have on children. This reaction highlights a disconnect between adult perceptions of children's experiences and children's lived realities. Occupational therapists cannot truly understand children's experiences—or know what's best for them—without first creating spaces where children's voices are heard. This gap reflects a broader issue linked to the adult-centred paradigm in healthcare, as discussed by Carnevale et al. (2017). The adult-centred paradigm tends to prioritize adult interpretations, expectations, and assumptions about children's needs and experiences. Consequently, interventions are often shaped by what adults, such as parents or healthcare providers, believe is best, rather than by what children themselves express or demonstrate (Carnevale, 2024).
In line with this critique, a recent qualitative study by Davies et al. (2024) highlighted that children feel they have a voice in their healthcare when they are genuinely heard—being attentively listened to, taken seriously, and acknowledged as individuals with valid perspectives and emotions. Thus, an initial step is to recognize and challenge the adult-centred paradigm. Occupational therapists can critically examine how children's perspectives and emotional experiences are integrated into their practice. This requires the courage to reflect on their stance as listeners. Engaging with a narrative that immerses the reader in the child's lived experience—similar to what participants encountered in the focus group—is one way to foster such reflexivity (Schiavo, 2024).
Amplifying Children's Perspectives in Goal Setting
Among the key findings of this study, participants emphasized the importance of mutual agreement on goals within the therapeutic relationship. However, they explained that this becomes increasingly complex when working with children. The goals of children, parents, and other stakeholders often diverge. Existing literature supports this observation, noting that children tend to prioritize goals related to leisure and autonomy, while parents more frequently emphasize academic performance and physical functioning (Costa et al., 2017). In such contexts, participants explained they often prioritize parental goals, which limits the child's role in the goal-setting process. This tendency reflects a broader pattern across healthcare systems, where children's perspectives are frequently unheard in goal setting processes (Koller, 2017; O’Connor et al., 2021). Curtis et al. (2022) showed that barriers exist to involving children in these processes, particularly for young children and for those with cognitive or communication difficulties. In the absence of specific strategies, these children are often excluded.
It is crucial to address this exclusion, as this issue has significant implications. A lack of agreement on goals can lead to ruptures in the therapeutic relationship and undermine the development of a shared focus (Crom et al., 2020; Øien et al., 2010; Safran & Kraus, 2014). While integrating children's goals into the intervention process is a positive intention, it is now crucial to reflect on how this practice can be enacted. Future research should explore and evaluate inclusive strategies to goal setting. One promising avenue involves the PhotoVoice as a strategy for goal selection among a diverse range of children, enabling an understanding of what matters to children in their daily lives through photographs (Greco et al., 2017). Future research should also address two unanswered questions: how to address differing perspectives on goals and needs expressed by parents, children, and other stakeholders? How can occupational therapists move beyond systematically prioritizing the needs of adults? It would be valuable to investigate these questions through participatory research involving occupational therapists, parents, and children.
Strengths and Limitations
Several strategies were implemented to ensure the rigour of this qualitative study. Four focus groups were conducted which enabled the identification of shared themes across groups. Moreover, the lead analyst, who has clinical experience in occupational therapy with children, was deeply engaged in the research process through prolonged engagement, including attending all focus groups and transcribing the verbatim data. Thematic development was further strengthened through collaborative analysis sessions between the researchers. Prolonged engagement and triangulation of analysts enhance the rigour of qualitative research (Johnson et al., 2020).
However, the final analysis was not member-validated, which may limit the credibility of the findings. To mitigate this, participants were invited to react to preliminary interpretations at the end of each focus group, and the results were analyzed by two moderators present during the sessions. Additionally, the sample included French-speaking occupational therapists working in diverse clinical settings across Québec. The cultural specificity of this context calls for caution when considering the transferability of the findings to other regions. Because focus groups were conducted in French, the findings may not fully capture perspectives of occupational therapists who are non-French-speaking or who practise in other linguistic contexts. Another limitation is the lack of information on the age range of the clientele the participants worked with.
Conclusion
This study explored occupational therapists’ perspectives on the therapeutic relationship with children, building on emerging evidence from children's own accounts. Four focus groups were conducted with occupational therapists working with children in Québec. Through these discussions, participants observed that children often play a limited role in decision-making, particularly in goal setting, which is a key aspect of the therapeutic relationship. They also noted that children have few opportunities to express their perspectives and emotions regarding therapy. Participants also became aware that children may experience difficult emotions during therapeutic activities, underscoring the need for a supportive relationship. These observations elicited surprise and prompted critical reflection among participants. In response to these observations, they proposed strategies to strengthen the therapeutic relationship, including facilitating children's expression, following their lead, and supporting them in navigating challenges. These suggestions are closely tied to the recognition of children as active participants in therapy, deserving of space to express themselves and influence the therapeutic process.
Key Messages
Children, especially younger ones, have a limited role in decision-making and few opportunities to express their experiences and emotions, which can affect the therapeutic relationship.
A disconnect exists between occupational therapists’ perceptions of children's experiences and children's actual perspectives, highlighting the risk that these perspectives are overlooked unless they are actively elicited.
Fostering children's active participation in goal setting and responding meaningfully to their experiences are essential strategies for strengthening the therapeutic relationship.
Supplemental Material
sj-docx-1-cjo-10.1177_00084174261445814 - Supplemental material for Learning From Children's Perspectives: Occupational Therapists’ Reflections on Their Therapeutic Relationship
Supplemental material, sj-docx-1-cjo-10.1177_00084174261445814 for Learning From Children's Perspectives: Occupational Therapists’ Reflections on Their Therapeutic Relationship by Sandrine Gagné-Trudel, Pierre-Yves Therriault and Noémi Cantin in Canadian Journal of Occupational Therapy
Footnotes
Acknowledgments
Our research team would like to thank the occupational therapists who generously shared their perspectives during the focus groups. The authors also wish to thank the Ordre des ergothérapeutes du Québec for their support in the recruitment process.
During manuscript preparation, the authors used Microsoft 365 Copilot for translating the text from French to English and refining its language through spelling corrections and syntax improvements, applied to both the abstract and the main body. The authors acknowledge the inherent limitations of language models, including the potential for errors or gaps in knowledge. Therefore, the English text was subsequently reviewed by the authors, with attention to spelling and grammar.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research did not receive direct funding. The first author received financial support for doctoral studies, within which this research was conducted. This support included a scholarship from the Ordre des ergothérapeutes du Québec and the Comité partenarial – Fonds de recherche Inclusion sociale.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.