
Abstract
Background
Type 1 diabetes (T1D) is a lifelong condition affecting all aspects of life. Although Lifestyle Redesign® interventions support diabetes self-management, little is known about which intervention exposure and engagement indicators are associated with changes in glucose outcomes, quality of life (QoL), and diabetes-related distress.
Purpose
To explore intervention exposure and engagement indicators associated with pre–post changes in glucose, QoL, and diabetes-related distress among individuals receiving the REAL-Telehealth (REAL-T) intervention.
Method
Using an as-treated analytic approach, data from the REAL-T randomized controlled trial were analyzed. Outcomes included changes in A1c, glycemic risk index (GRI), QoL, and diabetes-related distress. Intervention factors included the number of goals, the number of occupational therapy sessions, goal attainment, and changes in occupational performance. Hierarchical regression analyses were conducted.
Findings
In models adjusted for baseline values and relevant demographic covariates, baseline A1c and a higher proportion of goals met were associated with greater reductions in A1c. Higher baseline GRI, non-Hispanic White race/ethnicity, a higher proportion of goals met, and greater improvements in occupational performance were associated with better improvements in GRI scores. Changes in QoL and diabetes-related distress were primarily explained by baseline levels, with limited additional contribution from intervention exposure and engagement indicators.
Conclusions
This exploratory, process-focused analysis identified a limited number of intervention exposure and engagement indicators associated with outcome changes. Findings highlight the importance of process-level analyses to better understand how Lifestyle Redesign® interventions operate in real-world contexts and to inform future intervention refinement.
Introduction
Type 1 diabetes (T1D) is a lifelong chronic condition that often first appears in childhood or adolescence. Individuals with T1D experience fluctuating glucose levels, which can cause bodily pain (Molvaer et al., 2020), decreased strength (Orlando et al., 2017; Tyagi et al., 2020), and fatigue (Goedendorp et al., 2014; Romadlon et al., 2022), alongside psychological challenges such as anxiety (Rechenberg et al., 2017), depression (Akbarizadeh et al., 2022; Farooqi et al., 2022), diabetes-related distress (DD; AlOzairi et al., 2024), and stress (Kelly et al., 2022). These medical and psychological burdens, combined with the constant demands of diabetes self-management, the unpredictability of glucose levels, and concerns about hypoglycemia, can disrupt daily routines and limit engagement in academic, work, leisure, and social activities (Babler & Strickland, 2015; Sawyer et al., 2022; Verbist & Condon, 2021). Stigma, discomfort with technologies such as insulin pumps, and environmental barriers such as weather and temperature further restrict social participation and contribute to feelings of difference or social withdrawal (Mattacola, 2020; Montali et al., 2022; Sawyer et al., 2022; Verbist & Condon, 2021). Such occupational challenges may influence parent and peer relationships (Raymaekers et al., 2020) and negatively affect quality of life (QoL), limiting engagement in meaningful daily roles (Molvaer et al., 2020).
The “transition period” toward adulthood and adult diabetes care, typically occurring between the ages of 18 and 22 (Monaghan & Baumann, 2016), is critical for young adults with T1D. During this time, they shift from a family centered, parent-assisted management pattern to a more independent one. Failure to adjust to health insurance changes and ensure an effective transition can result in loss of follow-up, reduced clinical attendance (Cadario et al., 2009), treatment adherence challenges (Monaghan & Baumann, 2016), and difficulty finding healthcare resources (Pyatak et al., 2014). Also, young adults with T1D are more likely than other age groups to engage in risky behaviors, such as substance use and disordered eating (Gill et al., 2014; Monaghan et al., 2015). This period also often involves significant changes in their educational, employment, and living circumstances (Gill et al., 2014). All of these issues contribute to elevated glucose levels (Rausch et al., 2012), higher hospitalization rates, and increased emergency service admissions for severe conditions (Nip & Lodish, 2021).
Occupational therapy (OT) plays a crucial role in supporting diabetes management among youth and adults. OT treatment may address many concerns, including the primary disorder, secondary complications, psychological issues, QoL, treatment adherence, and contextual variables that interfere with management (Pyatak, 2011; Shen & Shen, 2019). Lifestyle Redesign® is an OT intervention framework that guides individuals to understand how everyday behaviors impact health and develop meaningful health-promoting habits and routines, which has been shown to be effective in diabetes management (Pyatak et al., 2022). In a pilot randomized trial (n = 81), the Resilient, Empowered, Active Living with Diabetes (REAL Diabetes) intervention was shown to help improve HbA1c, health status, diabetes-related QoL, and habit strength for checking blood glucose among young adults with diabetes (Pyatak et al., 2018, 2019). The REAL-Telehealth (REAL-T) intervention, which followed the same framework and principles as the REAL intervention and provided services to young adults with T1D via telehealth, significantly improved participants’ occupational performance, occupational satisfaction, and health management (Mitchell et al., 2023), as well as their diabetes distress and diabetes-related QoL (Pyatak et al., 2025).
Individual characteristics may also influence diabetes outcomes, making it important to account for baseline differences among participants. Prior research indicates that age, self-identified gender, and race/ethnicity may affect both glucose control and psychosocial outcomes in T1D. For example, older age and certain racial/ethnic groups are associated with higher HbA1c levels, while female adolescents commonly report lower QoL and greater DD compared with males (Castellano-Guerrero et al., 2020; Nieuwesteeg et al., 2012; Ram et al., 2024; Yardley et al., 2018). Lifestyle Redesign ® can be considered a complex intervention due to its multiple components, which include targeting a wide range of behaviors, requiring specialized expertise from both providers and recipients, and allowing flexibility in its implementation across varied contexts (Skivington et al., 2021). Because such complexity makes it difficult to determine which specific components, processes, or levels of engagement contribute to observed intervention effects, and under what conditions these effects occur, investigating treatment mechanisms and interactions between intervention components and contexts is essential for identifying effective and critical elements of interventions and optimizing current treatments (Moore et al., 2015; Nock, 2007). In this context, intervention factors are conceptualized as indicators of participants’ exposure to and engagement with the intervention, such as participation in goal-directed activities, intensity or completion of the program, and engagement in the therapeutic process, rather than as intervention components or outcomes. Therefore, we use an as-treated, process-oriented analytic approach to explore associations between intervention components and engagement-related factors and changes in diabetes-related outcomes. This study thus aimed to answer the following research questions, among young adults receiving OT through the REAL-T study: What intervention factors are associated with more improvement in (1) glucose values, (2) QoL, and (3) DD?
Methods
Study Design
The purpose of this study is to explore intervention mechanisms using pre–post, descriptive data from the REAL-T study (NCT04023487). The REAL-T study is a two-arm, parallel-group, randomized controlled trial that aims to evaluate the efficacy of the REAL intervention delivered via telehealth. Participant recruitment and data collection occurred between October 2019 and November 2022. Detailed information on the overall study design, methodology, and outcomes of the REAL-T research program has been published previously (Mitchell et al., 2023; Pyatak et al., 2023, 2025). Below, we will briefly introduce relevant aspects of the present study.
Participants
The inclusion criteria for participants were as follows: aged 18–30 years, fluent in English or Spanish, diagnosed with T1D for at least 12 months, and HbA1c (average glucose levels) of ≥7.5% at the time of enrollment. REAL-T participants included residents of the greater Los Angeles area and other states where the study occupational therapists were licensed (CA, CO, OR, TX, and WA). Exclusion criteria included being currently pregnant or planning to become pregnant within the next 12 months, or having cognitive impairments. Individuals with severe disabilities were also excluded because the REAL-T intervention focuses on long-term lifestyle redesign strategies and behavior change processes that require stable participation over time. In addition, excluding participants with severe medical complexity helped minimize the introduction of confounding factors unrelated to diabetes self-management. Participants with limited access to technology for telehealth were provided with laptops, webcams, and internet hotspots, as well as training on how to use these devices, in order to facilitate participation. All participants provided informed consent prior to completing study procedures, and the study was approved by the University of Southern California Institutional Review Board.
Intervention
The REAL-T intervention applies a Lifestyle Redesign® approach to address how diabetes is embedded within daily life roles, routines, and environments. Rather than just providing standardized education content, occupational therapists work collaboratively with participants to identify personally meaningful goals across multiple life domains and implement individualized behavior change strategies. The REAL-T intervention also offers flexible participation options, allowing participants to meet with their occupational therapists from any location and at times that fit within their daily routines, thereby supporting the integration of diabetes care into everyday life. In the REAL-T study, participants were randomly assigned to either the intervention group or the control group. The current analysis includes only data from participants assigned to the intervention group, as our aim was to examine intervention mechanisms using as-treated process data. Participants assigned to the intervention group received 6 months of telehealth OT (via HIPAA-compliant Zoom). The frequency of the intervention sessions was tailored to participants’ preferences and treatment goals, occurring either weekly or bi-weekly. The occupational therapists were trained in Lifestyle Redesign® and motivational interviewing, which is a client-centered approach that emphasizes collaboration, autonomy, and eliciting individuals’ motivations for behavior change. Motivational interviewing-informed strategies were used to support participants’ goal setting and facilitate participant engagement. An initial evaluation was conducted by therapists to gather detailed information about client strengths and barriers, and establish goals, which were set collaboratively by clients and therapists. The intervention included five core domains addressing (1) Healthy Habits and Routines: encompassed nondiabetes-specific daily activities and routines, including activities of daily living (ADLs), time management, leisure, rest, and lifestyle organization (i.e., goals that could reasonably apply to individuals without diabetes); (2) Managing Diabetes: focused on diabetes-specific self-management behaviors, such as blood glucose monitoring, insulin administration, ketone checking, diabetes device management, hypoglycemia prevention and management, and reviewing glucose trends; (3) Emotions and Well-Being: included goals related to stress management, emotional regulation, and coping with the psychosocial demands of living with diabetes; (4) People and Places: addressed participation in social and community contexts, including self-advocacy in interpersonal, educational, workplace, or healthcare settings; and (5) Accessing Care: focused on navigating healthcare systems and resources, such as scheduling appointments, obtaining supplies, insurance-related tasks, and communicating with healthcare providers. Goals and treatment activities were categorized within these domains, helping therapists structure treatment sessions and track progress toward goals.
Measures and Data Collection
Participants in the REAL-T intervention group were used, and data were collected before and after the 6-month intervention. Full data collection procedures were described in a previous publication (Pyatak et al., 2023); for the purposes of this analysis, we focused on the following measurements. Glucose outcomes were assessed using A1c and glycemic risk index (GRI), a composite metric derived from continuous glucose monitoring data (Klonoff et al., 2023). GRI provides a quick assessment of the overall risk of glycemic variability, including both hyperglycemia and hypoglycemia, to identify patients most in need of care (Klonoff et al., 2023). The GRI ranges from 0 to 100, with higher GRI values indicating poorer overall glycemia. QoL was assessed using the Audit of Diabetes-Dependent Quality of Life Questionnaire-15 (ADDQoL-15), a questionnaire to evaluate the impact of diabetes on various life domains (Bradley & Speight, 2002). Its scoring ranges from −9 to +3, with lower scores reflecting a more negative impact of diabetes on QoL. The ADDQoL-15 has demonstrated strong internal consistency (Cronbach's α = 0.95; Ostini et al., 2012) and sensitivity to diabetes severity and treatment outcomes (Wee et al., 2006). Diabetes distress was evaluated using the Diabetes Distress Scale (DDS), a scale that assesses diabetes-related emotional burden and stress (Polonsky et al., 2005). The DDS comprises four subscales indicating various sources of diabetes distress: emotional distress, physician distress, regimen distress, and interpersonal distress. Total scores and subscale scores range from 1 to 6, with higher scores reflecting greater diabetes distress. The DDS has shown adequate internal reliability across its four subscales (Cronbach's α > 0.87) and validity supported through associations with depression, regimen behaviors, and clinical indicators (Polonsky et al., 2005).
According to the Process Evaluation Model mentioned in Moore et al. (2015), a theoretical model providing a framework designed to capture participants’ exposure to and engagement with the REAL-T intervention was developed (Figure 1). These indicators were selected to reflect variation in how participants engaged with the intervention and included: (1) number of goals collaboratively established during treatment; (2) number of OT sessions attended, reflecting intervention dose; (3) proportion of goals met and partially met, conceptualized as an indicator of engagement with goal-directed intervention activities, and calculated by dividing the number of goals rated as “met” or “partially met,” respectively, by the total number of goals set by each participant; and (4) change in Canadian Occupational Performance Measure (COPM) scores (performance and satisfaction). The COPM is an evidence-based tool designed to capture a client's self-perception of their ability to perform daily tasks with good internal consistency (Cronbach's α = 0.93 for performance; Cronbach's α = 0.89 for satisfaction; Berardi et al., 2019), validity, and responsiveness (Carswell et al., 2004; Canadian Occupational Performance Measure (COPM), n.d.). COPM scores range from 1 to 10, with higher scores representing better occupational performance and satisfaction. Importantly, goal attainment and COPM change scores were treated as process-related indicators rather than intervention components or primary outcomes, and were used to explore potential mechanisms through which participation in the intervention may be associated with changes in diabetes-related outcomes.
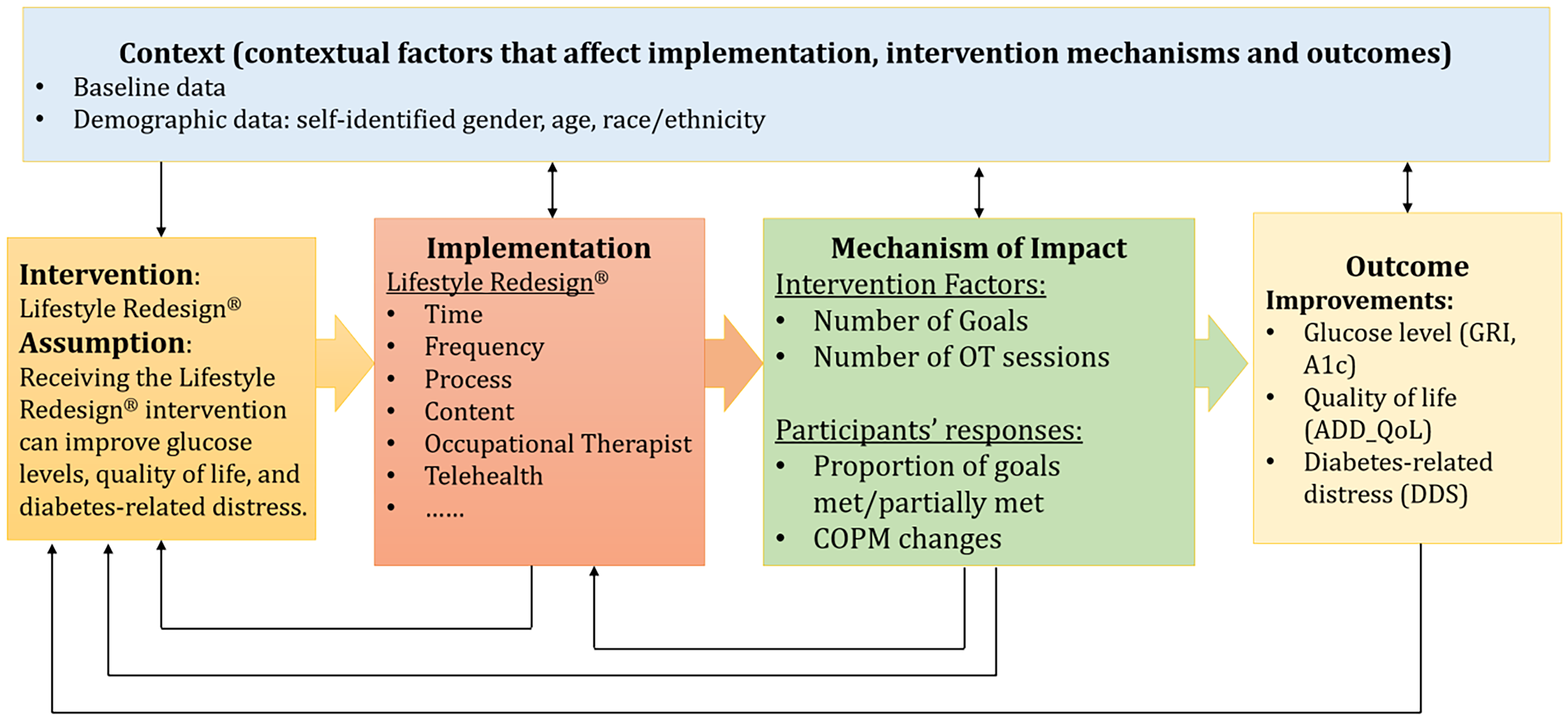
Conceptual framework for process-focused analysis of REAL-T intervention.
Control variables used in the analysis included: baseline A1c and baseline GRI scores, baseline ADDQoL-15 scores, baseline DDS-total scores, as well as age, self-identified gender, and race/ethnicity, which were selected based on prior evidence showing their associations with HbA1c, QoL, and diabetes distress in T1D populations.
Data Analysis
Data was stored in REDCap, and downloaded and imported into SPSS software version 26.0 for analysis. The analytic sample included all 104 participants assigned to the intervention group. As this study was an exploratory, hypothesis-generating secondary analysis of an existing trial, no a priori power calculation was conducted. Given that this study is an exploratory analysis intended to identify potential intervention mechanisms and factors for intervention refinement, rather than definitively assessing intervention efficacy, we prioritized minimizing the risk of Type II error over strict control of Type I error. Increasing the Type I error rate to 0.1 can reduce Type II errors and improve overall statistical decision accuracy in exploratory research contexts (Carlin et al., 2024; Jiménez-Gamero & Analla, 2023). Accordingly, we used a two-sided p-value <.1 to indicate potentially meaningful associations that may warrant further investigation.
Descriptive statistics were calculated for the demographics and baseline characteristics of the intervention group. The extent of missing data varied across variables, with available sample sizes ranging from n = 64 to 104, corresponding to missingness rates of 0% to 38.5%. Missing data primarily resulted from incomplete follow-up assessments rather than baseline differences. Preliminary analyses indicated that observed variables were associated with missingness patterns, consistent with the assumption that data were plausibly missing at random.
Missing data were handled using multiple imputation by the fully conditional specification that uses a separate conditional distribution for each imputed variable. We specified logistic regression for binary/categorical variables and linear regression for continuous variables. The multiply imputed data sets were then analyzed by using standard procedures for complete data and combining the results from these analyses. This process results in valid statistical inferences that properly reflect the uncertainty due to missing values (for complete discussions, see Enders, 2023; Schafer and Graham, 2002). A total of 100 imputed data sets were generated and used for data analysis. Auxiliary variables were included primarily to support multiple imputations for missing data and to account for baseline participant characteristics and contextual factors that could influence the accuracy of imputed values. These variables included baseline REAL-data quality scores, number of occupational deficits, evaluation code complexity, prognosis, intervention-related process indicators, baseline and changes of the study outcomes, as well as other baseline characteristics including recruitment sources (clinic or social media), employment status, social deprivation index, continuous glucose monitoring (CGM) data source (study or personal CGM), age, race/ethnicity, and self-identified gender. While some of these variables could also provide insight into for whom the intervention might be more effective, their primary role in this analysis was to improve the validity and precision of multiple imputation and adjusted analyses, ensuring robust estimation of associations between intervention process indicators and changes in diabetes-related outcomes.
In all models, the dependent variable was the pre–post change score for the outcome of interest (post minus pre). Hierarchical multiple regression analyses were conducted to examine whether specific intervention factors predicted improvements in outcomes and to evaluate their contribution to each model. Variables were entered in sequential blocks that reflected the temporal ordering of intervention delivery and associated process indicators: first, participants set treatment goals in collaboration with their therapists (number of goals); next, they began treatment, with the number of OT sessions recorded; after which goal attainment was evaluated (proportion of goals met and partially met), and the COPM were reassessed to capture changes (pre–post COPM changes).
In the unadjusted models, the number of goals was entered first, followed by the number of OT sessions, and then the proportion of goals met and partially met, and pre–post COPM changes. In the adjusted models, baseline clinical and demographic characteristics (baseline A1c and GRI; baseline ADDQoL; baseline DDS-total score; age, self-identified gender, and race/ethnicity) were entered in the first block as control variables, followed by the intervention variables in the same sequence as the unadjusted models. A detailed description of the variable entry order for each block is provided (Supplemental File and Table 1).
Participant Demographic and Clinical Characteristics.
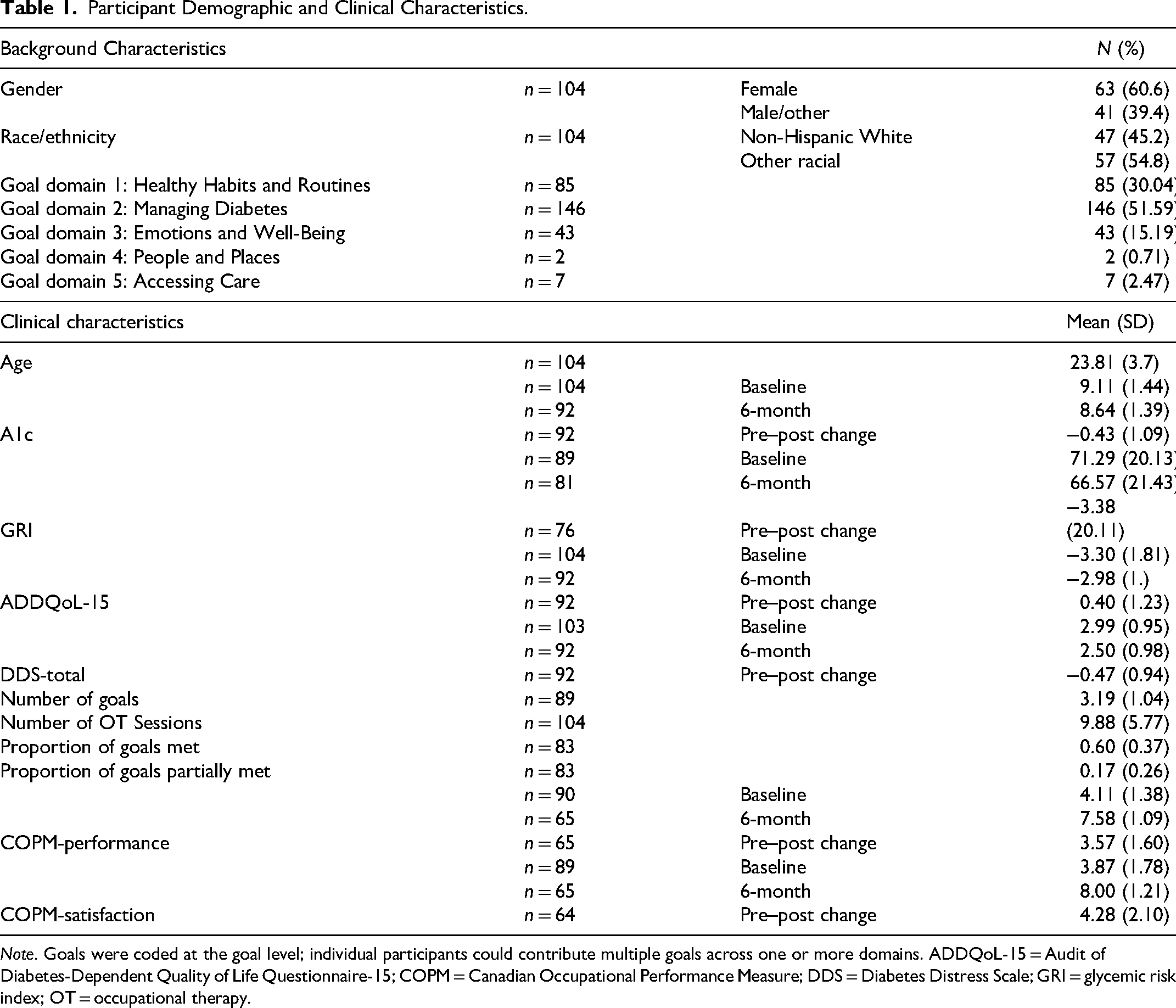
Note. Goals were coded at the goal level; individual participants could contribute multiple goals across one or more domains. ADDQoL-15 = Audit of Diabetes-Dependent Quality of Life Questionnaire-15; COPM = Canadian Occupational Performance Measure; DDS = Diabetes Distress Scale; GRI = glycemic risk index; OT = occupational therapy.
We reported the pooled estimates for the coefficients (B value) and 90% confidence intervals (CIs), along with the calculations of the mean values for R2 and change in R2 (ΔR2). We also examined the variance inflation factor (VIF) associated with each predictor to ensure that multicollinearity was not present, and a VIF < 5 indicates no concern of multicollinearity.
Results
The average age of the participants was 23.81 years old. At baseline, participants had an average A1c of 9.11%, indicating glycemic levels substantially above recommended targets for adults with T1D. The mean GRI was 71.29, reflecting elevated overall glycemic risk due to both hyperglycemia and hypoglycemia. Participants also reported impaired diabetes-related QoL (mean ADDQoL-15 = −3.30) and moderate diabetes distress (mean DDS-total = 2.99), consistent with clinically meaningful psychosocial challenges. Baseline occupational performance and satisfaction were low (COPM-performance = 4.11; COPM-satisfaction = 3.87), indicating difficulties performing and feeling satisfied with daily activities related to diabetes management. On average, participants attended 9.88 OT sessions over the 6-month intervention period. Participants set a total of 283 participant-defined goals, which were categorized into five different domains. Most goals focused on Managing Diabetes (Domain 2; n = 146, 51.6%), followed by Healthy Habits and Routines (Domain 1; n = 85, 30.0%) and Emotions and Well-Being (Domain 3; n = 32, 11.3%).
Results of the hierarchical multiple regression models are presented in Tables 2 to 5. In the unadjusted models, intervention exposure and engagement indicators explained 12% of the variance in pre–post A1c change (Table 2), 14% of the variance in GRI change (Table 3), 10% of the variance in QoL change (Table 4), and 9% of the variance in DDS change (Table 5). No intervention exposure and engagement indicators showed as a statistically meaningful predictor of outcome change in the unadjusted models.
Hierarchical Regression Model Predicting A1c (B, 90% CI).
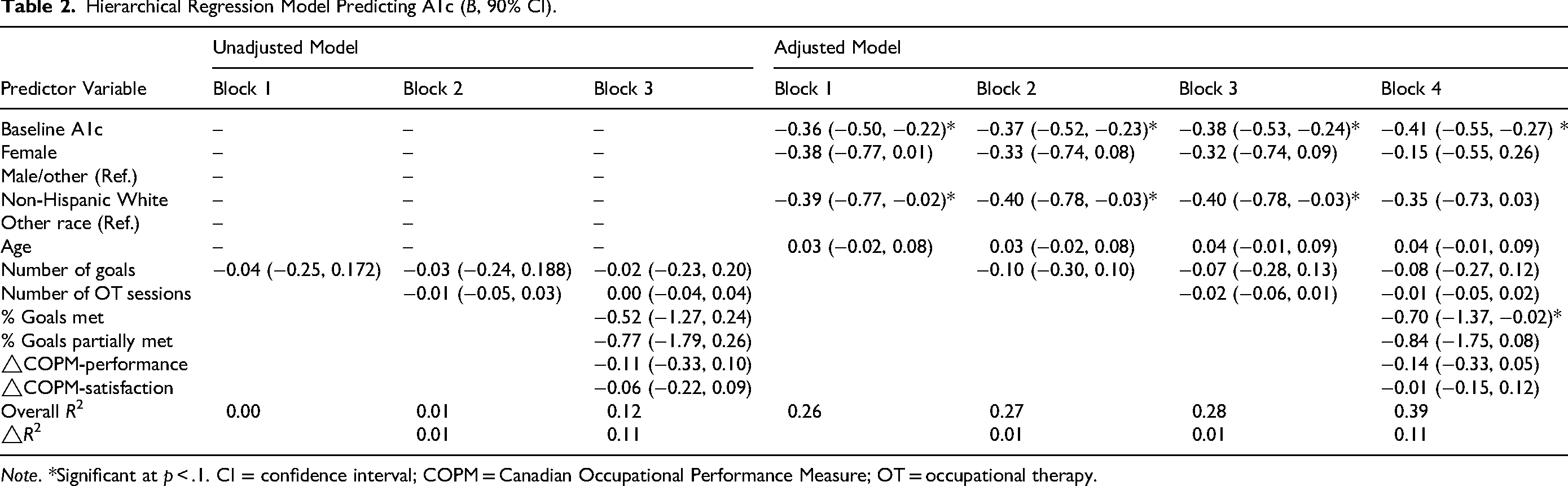
Note. *Significant at p < .1. CI = confidence interval; COPM = Canadian Occupational Performance Measure; OT = occupational therapy.
Hierarchical Regression Model Predicting GRI (B, 90% CI).
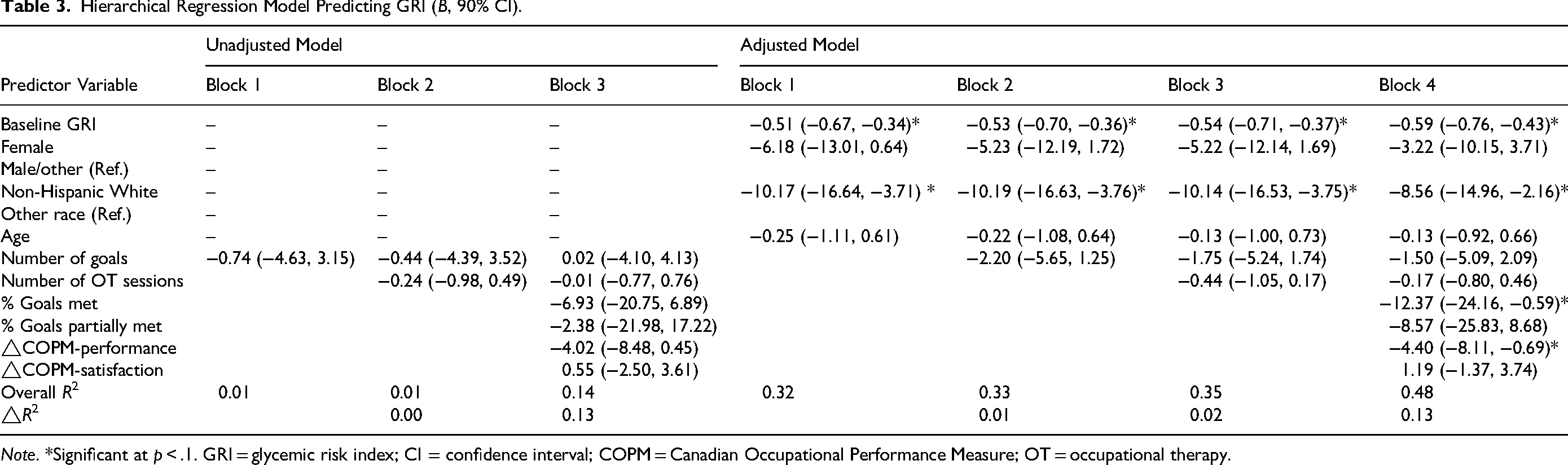
Note. *Significant at p < .1. GRI = glycemic risk index; CI = confidence interval; COPM = Canadian Occupational Performance Measure; OT = occupational therapy.
Hierarchical Regression Model Predicting ADDQoL-15 (B, 90% CI).
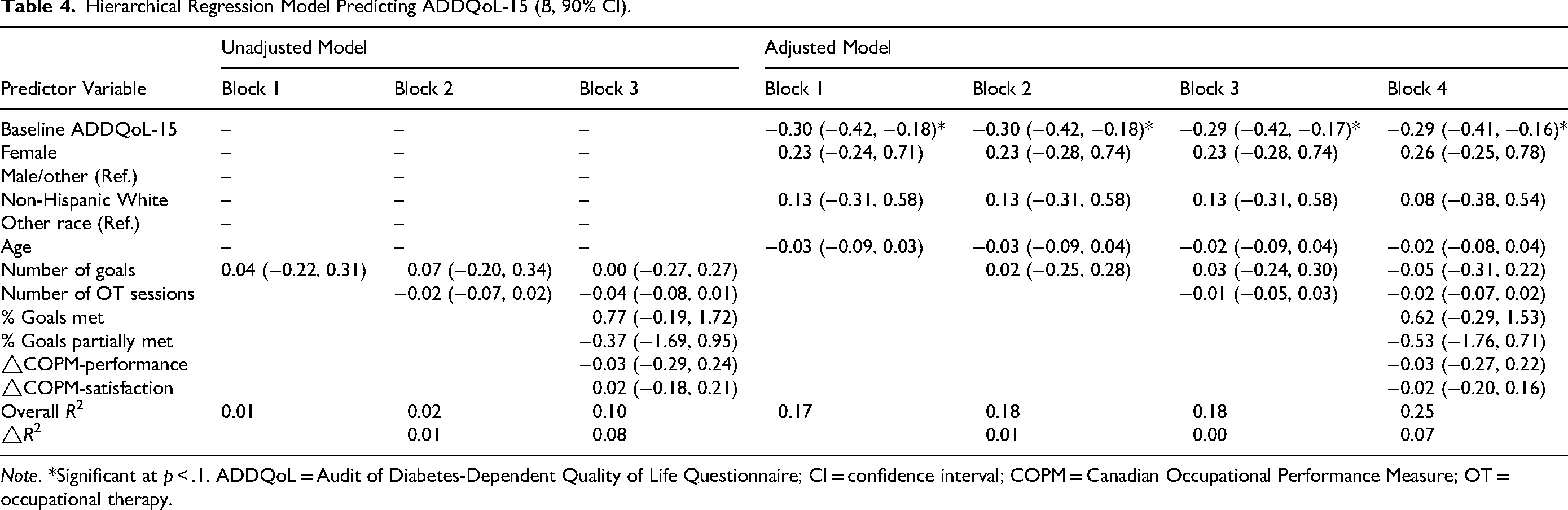
Note. *Significant at p < .1. ADDQoL = Audit of Diabetes-Dependent Quality of Life Questionnaire; CI = confidence interval; COPM = Canadian Occupational Performance Measure; OT = occupational therapy.
Hierarchical Regression Model Predicting DDS-Total (B, 90% CI).
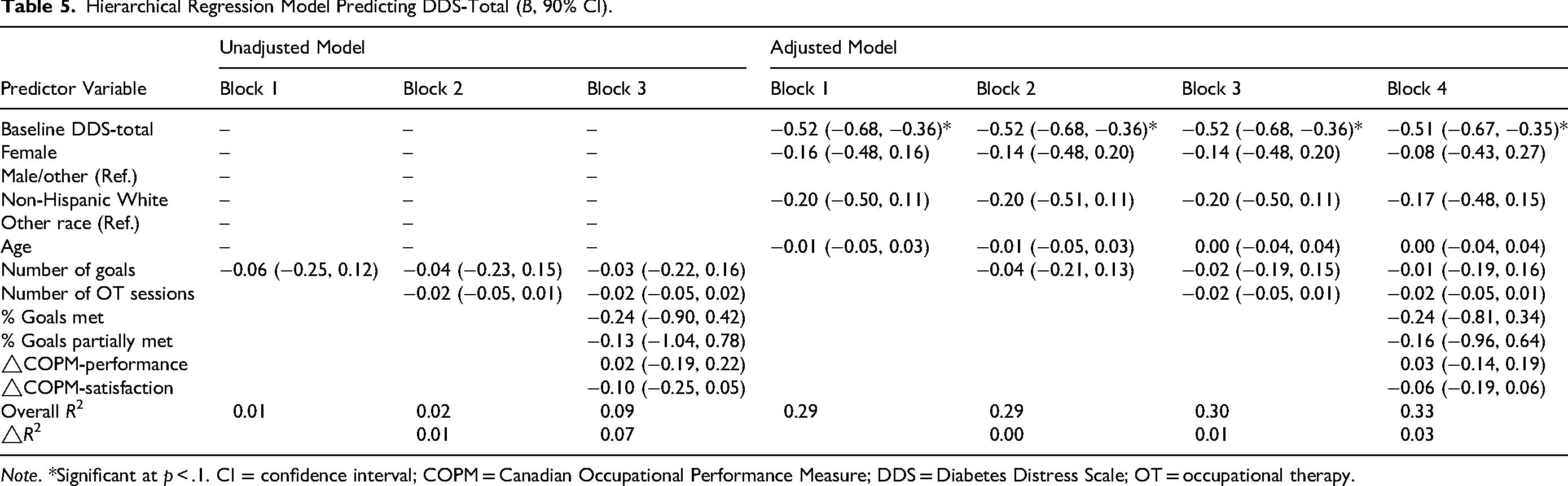
Note. *Significant at p < .1. CI = confidence interval; COPM = Canadian Occupational Performance Measure; DDS = Diabetes Distress Scale; OT = occupational therapy.
In the adjusted A1c models, the final model accounted for 39% of the variance in the pre–post A1c change. Higher baseline A1c (CI: −0.55, −0.27) and a higher proportion of goals met (CI: −1.37, −0.02), reflecting greater engagement in the intervention process, were statistically associated with larger reductions in A1c over the intervention period. Demographic and baseline clinical characteristics accounted for 26% of the variance, while intervention exposure and engagement indicators accounted for 13%. No sociodemographic variables were significantly associated with changes in A1c after adjustment.
For the adjusted GRI models, the final model accounted for 48% of the variance in the pre–post GRI change. Higher baseline GRI (CI: −0.76 to −0.43), non-Hispanic White race/ethnicity (CI: −14.96 to −2.16), a higher proportion of goals met (CI: −24.16 to −0.59), and greater improvements in COPM-performance (CI: −8.11 to −0.69) were associated with larger improvements in GRI scores. Overall, demographic and control variables accounted for 32% of the variance in GRI change, while intervention exposure and engagement indicators explained an additional 15%. Among sociodemographic variables, non-Hispanic White race/ethnicity was the only factor significantly associated with greater improvements in GRI scores.
In the adjusted QoL models, the final model explained 25% of the variance in the pre–post ADDQoL-15 change. Baseline QoL (CI: −0.41, −0.16) was the only variable associated with the pre–post change. Overall, baseline and demographic variables accounted for 17% of the variance in QoL change, whereas intervention exposure and engagement indicators accounted for 8%. No sociodemographic characteristics were significantly associated with changes in QoL after adjustment.
The adjusted DDS-total model revealed that 33% of the variance in the pre–post DDS-total change was explained by the included variables. Baseline DDS-total score (CI: −0.67, −0.35) emerged as the sole variable associated with change in diabetes distress. Overall, demographic and control variables accounted for 29% of the variance in DDS change, while intervention exposure and engagement indicators accounted for 4%. No sociodemographic variables were significantly associated with changes in diabetes distress.
Across all models, VIF values were <5 in 95% of imputed samples, indicating that no significant multicollinearity was observed.
Discussion
Lifestyle-oriented interventions have shown variable and often modest effects across populations, and the mechanisms through which they influence health outcomes remain insufficiently understood. Given this background, the purpose of this study was to explore potential associations between intervention exposure and engagement indicators and pre–post changes in glucose levels, QoL, and diabetes distress among intervention recipients. The findings suggest that certain intervention factors are differentially associated with changes across outcomes, although the magnitude of these associations was modest.
Factors Contributing to Glucose
In this study, the proportion of goals met was associated with greater pre–post improvements in both A1c and GRI. Although causal inferences cannot be drawn, this finding suggests that the extent to which individuals implement their self-identified treatment goals may be an important process-level indicator of the REAL-T intervention.
While the present analyses did not formally test the effects of individual goal domains, the distribution of treatment goals provides contextual information for interpreting this association. Most goals set by participants were concentrated in Diabetes Management (Goal Domain 2) and Healthy Habits and Routines (Goal Domain 1), both of which are theoretically closely linked to glycemic control. Goal Domain 2 focused on glucose-related knowledge and behaviors, including blood glucose awareness, glucose monitoring routines, insulin knowledge and use, and diabetes device management (e.g., “Client will check glucose levels 3x a day”). These behaviors are foundational components of diabetes self-management education and are consistently associated with improved glycemic outcomes in prior research, particularly when supported by diabetes technologies such as continuous glucose monitoring (Brown et al., 2022; Teo et al., 2022).
Goal Domain 1 emphasized the integration of diabetes management strategies into daily routines, including ADLs, rest, leisure, and other lifestyle modifications. Examples included reducing fast-food consumption (e.g., food quality, mealtime routines, and carbohydrate intake) or establishing regular exercise routines (e.g., “Client will exercise for 60 min at least 3x per week”). Such goals align with evidence indicating that integrating diabetes care into consistent daily habits can improve glycemic regulation by enhancing individuals’ awareness of how diet, activity, and routines influence blood glucose levels (Gal et al., 2022; Lin et al., 2017).
Some participants also set goals related to education or employment to enhance self-efficacy (e.g., “Client will pursue a new job or educational path in order to improve self-efficacy, motivation, and sense of independence”). Although these goals were less directly related to glycemic behaviors, improvements in self-efficacy and role engagement may indirectly support diabetes management by increasing motivation and adherence to self-care routines (Lin et al., 2017; Xu et al., 2008). Taken together, the predominance of goals addressing diabetes management and daily routines suggests that a higher proportion of goals met may reflect more consistent engagement with behaviors that are relevant to glycemic control.
Additionally, improvements in COPM-Performance were associated with changes in GRI, but not A1c. This finding further supports the potential differences in how functional performance relates to distinct glucose outcomes. GRI is sensitive to glycemic variability and risk, which may be more directly influenced by participants’ ability to effectively carry out diabetes-related tasks in daily life. Improvements in occupational performance may thus reflect participants’ increased effectiveness in behaviors such as regular blood glucose monitoring (Teo et al., 2022), adopting healthy lifestyle behaviors (Riddell et al., 2017), and managing diabetes devices appropriately (Molfetta et al., 2025), which could help reduce glycemic risk.
In addition to the intervention exposure and engagement indicators, baseline clinical and demographic characteristics were also associated with glucose outcomes. Higher baseline A1c and GRI were associated with greater pre–post improvements, and similar results were supported by previous research (Eldib et al., 2023; Sbroma Tomaro et al., 2017). This may be due to their greater potential for improvement compared to those closer to their glycemic targets. Moreover, pre–post GRI change differed by race/ethnicity. A previous study found that demographic variables (including age, gender, race/ethnicity, marital status, and socioeconomic status [SES] variables) explained variability in GRI scores, with race/ethnicity being the single demographic variable with significant impact (Hoogendoorn et al., 2023). Compared to other racial/ethnic groups, non-Hispanic White individuals with T1D are more likely to have private insurance, which provides more access to medical services and diabetes technology (Majidi et al., 2021). Furthermore, they tend to have higher SES, higher household income, greater educational attainment, and more frequent use of diabetes technology than other racial/ethnic groups (Agarwal et al., 2020). This finding highlights the importance of considering social factors of health when interpreting glucose outcomes, and suggests that interventions such as REAL-T may benefit from more explicit attention to addressing disparities in access to resources and diabetes technologies. However, these interpretations are speculative and should be interpreted cautiously, given that the present study was not designed to examine mechanisms underlying demographic differences.
Factors Contributing to QoL
Changes in diabetes-specific QoL were primarily associated with baseline QoL levels, with no additional intervention factors explaining variance in pre–post change. Participants with lower baseline QoL may have had greater room for improvement following the intervention, whereas those with relatively higher baseline QoL may have experienced more limited change, potentially reflecting a ceiling effect.
QoL represents an individual's perception of overall well-being, encompassing physical and mental health, social relationships, environmental context, work and financial status, and perceived independence and autonomy. While some intervention components could theoretically influence QoL via goal attainment, in the current study, goals targeting QoL-related domains (e.g., social participation, role balance, or emotional well-being) were relatively infrequent compared with goals focused on diabetes management and daily routines, which may help explain the limited associations observed between intervention exposure and engagement indicators and changes in QoL. As such, QoL is shaped by a combination of factors, including personal demographic characteristics (e.g., age), disease-related factors (e.g., T1D duration and presence of complications), glycemic control indicators such as HbA1c levels, and social and family support (Ahola et al., 2010; Anderson et al., 2017; Laffel et al., 2003). Given this complexity, interventions such as REAL-T are more likely to influence QoL indirectly through improvements in functional performance, diabetes self-management behaviors, and daily routines rather than exerting direct changes in global QoL perceptions. The absence of strong associations between intervention factors and QoL change in the present study may therefore reflect limitations in capturing these more indirect or less proximal effects within the study timeframe. This finding suggests that future refinements of the REAL-T program could benefit from incorporating more explicit QoL-oriented components, such as interventions targeting social participation, role balance, environmental barriers, or long-term life goals.
Factors Contributing to DDS
Similar to QoL, changes in DD were largely explained by baseline DDS scores, with intervention exposure and engagement indicators accounting for minimal additional variance. This pattern suggests that baseline levels of distress strongly influence pre–post change and may limit the detectability of intervention-related effects over a relatively short follow-up period.
DD refers to the emotional burden associated with the daily demands of living with diabetes, including concerns related to disease management, interactions with healthcare providers, and perceived lack of support. Approximately one quarter of individuals with T1D experience severe DD (Ventura et al., 2016). In the present study, some participants set goals related to emotions and well-being, which primarily focused on stress management and coping strategies (e.g., “Client will utilize strategies learned in session to implement boundaries with loved ones in order to optimize coping with stressors and reduce negative impacts on mental health”).
Prior research indicates that DD is closely linked to emotional factors such as depressive symptoms, anxiety, and feelings of powerlessness (Fisher et al., 2015; Powers et al., 2017). Beyond emotional functioning, DD is also shaped by disease-related and contextual factors, including glycemic control, diabetes self-management demands, and the use of diabetes technologies (Joensen et al., 2016; Lorenzen et al., 2024). Among younger individuals with T1D, concerns related to diet, weight, and body image may further contribute to distress (Powers et al., 2017). Additionally, demographic and social factors—such as age, sex, race/ethnicity, the presence of diabetes-related complications, and the availability of family and social support—have been shown to influence DD levels (Hernar et al., 2024; Joensen et al., 2016; Luo et al., 2021).
While the present analysis showed limited associations between intervention exposure and engagement indicators and changes in DD, prior evaluations of the REAL-T program found that participants experienced meaningful improvements in occupational performance, occupational satisfaction, and health management (Mitchell et al., 2023), along with reductions in DD and enhancements in diabetes-related QoL (Pyatak et al., 2025). Taken together, these findings suggest that the absence of observed associations in the current analysis may reflect contextual or implementation-related factors rather than a lack of intervention relevance for DD. In this context, and consistent with prior diabetes self-management literature emphasizing peer support as a core component, the telehealth delivery format and the absence of structured peer support may have constrained the potential impact on DD for some participants. Peer support is recognized as a key component in diabetes self-management programs, providing social modeling, emotional validation, and shared problem-solving opportunities that can help mitigate diabetes-related stress (Raymaekers et al., 2017; Yakubu et al., 2024).
Given the multifactorial nature of DD, it is plausible that an OT-based intervention such as REAL-T may exert only indirect or partial effects on DD, particularly when emotional support is not the primary focus of treatment. Although REAL-T incorporated goal-setting and stress-management elements, many contributors to DD—such as healthcare system interactions, perceived stigma, and long-standing emotional burden—may require more targeted psychosocial or mental health-focused interventions. Future program refinements could incorporate more explicit social or peer-oriented components, such as virtual group sessions or structured peer mentoring, to further enhance intervention effects on emotional well-being while maintaining the accessibility and flexibility of telerehabilitation. Additional recommendations include more structured screening for elevated DD, integration of distress-focused coping strategies, closer collaboration with mental health professionals, and longer follow-up periods to determine whether improvements in self-management and daily functioning could lead to sustained reductions in DD over time. In addition, modifying DDS language (e.g., replacing “physician” with “healthcare professional”) may improve construct relevance in interventions delivered primarily by nonphysician providers such as occupational therapists.
It is also important to consider the alignment between the core emphases of the REAL-T intervention and the outcomes assessed while interpreting findings. Although REAL-T is grounded in OT principles and targets daily routines, habits, and health management behaviors, some intervention components—such as goal setting, problem-solving around diabetes tasks, and education related to self-management routines—may resemble elements commonly found in therapeutic education programs. These components may exert more immediate and detectable effects on proximal biomedical outcomes such as glycemic control, particularly HbA1c, which is sensitive to relatively short-term changes in self-management behaviors.
In contrast, occupational outcomes and broader psychosocial constructs, including occupational performance, satisfaction, and QoL, may require more sustained engagement, cumulative behavioral change, and longer follow-up periods to demonstrate measurable improvement. Occupational outcomes are also inherently individualized and context-dependent, which may reduce their responsiveness to standardized indicators of intervention exposure within the timeframe of the present study. As a result, the observed stronger associations between intervention exposure and engagement indicators and HbA1c, compared with occupational or psychosocial outcomes, may reflect differences in outcome sensitivity and temporal dynamics rather than a misalignment between the intervention's occupational focus and its intended targets.
Importantly, prior evaluations of the REAL-T program have documented meaningful improvements in occupational performance, occupational satisfaction, and health management, as well as reductions in diabetes distress and improvements in diabetes-related QoL, indicating that the intervention is capable of producing occupationally relevant and psychosocial benefits. The absence of associations between the intervention exposure and engagement indicators examined in the present study and changes in QoL or DD does not necessarily contradict these earlier findings. Rather, it suggests that improvements in these outcomes may reflect the overall therapeutic context or cumulative effects of participation in REAL-T, which may not be fully captured by the specific intervention indicators operationalized in this secondary analysis. In contrast, glycemic outcomes such as HbA1c and GRI may be more sensitive to variation in concrete self-management behaviors and goal implementation, making them more likely to show associations with indicators of intervention engagement. Taken together, these findings underscore the importance of distinguishing between intervention effectiveness and the identification of specific mechanisms or components that explain variability in outcomes. Future research should therefore aim to more comprehensively examine how different intervention elements, relational processes, and contextual factors jointly contribute to both biomedical and occupational outcomes.
Strength
This exploratory study was designed to examine which intervention exposure and engagement indicators were associated with pre–post changes, rather than simply evaluating whether the intervention was effective. To support this purpose, the intervention process was operationalized into specific, theory-informed components, including the number of intervention goals, proportion of goal attainment, treatment duration (dose), and changes in occupational performance. Examining these components in relation to multidimensional outcomes spanning physiological, psychological, and social domains allowed for a more refined understanding of intervention-associated changes in both biological and psychosocial functioning.
In addition, the analyses were grounded in real-world clinical practice. Treatment goals were generated collaboratively by participants and therapists and reflected authentic therapeutic processes, enhancing the ecological validity of the findings and supporting their relevance to OT interventions for individuals with diabetes.
Limitations
This study has limitations. First, as an exploratory, hypothesis-generating secondary analysis, the study was not designed to establish causal relationships between intervention components and outcomes, but observed associations as descriptive of potential mechanisms.
Second, the operationalization of intervention exposure and engagement indicators was limited by the structure of available clinical data. For example, goal attainment was summarized using proportion-based indicators, which may not fully capture qualitative differences in goal complexity, clinical relevance, or individual effort. Similarly, the number of OT sessions may reflect both treatment dose and participants’ evolving needs during therapy, limiting its interpretation as an independent predictor.
Third, missing data were more prevalent for intervention exposure and engagement indicators (e.g. COPM) than for other outcome measures, which introduced greater uncertainty in estimating the contribution of these variables despite the use of multiple imputation. This may have reduced the ability to detect associations involving occupational performance changes.
Finally, the COVID-19 pandemic and the transition to remote trial implementation may have influenced both participant experiences and data completeness. Pandemic-related disruptions could have affected glycemic control, mental health, and access to diabetes management resources, thereby limiting the generalizability of findings to nonpandemic contexts.
Conclusion
This exploratory, process-focused analysis examined associations between intervention exposure and engagement indicators and pre–post changes in glucose outcomes, QoL, and DD among participants who received the REAL-T intervention. Baseline levels accounted for a substantial proportion of variance in outcome changes, while a limited number of intervention exposure and engagement indicators—most notably the proportion of goals met—were associated with changes in selected glucose-related outcomes. Few intervention exposure and engagement indicators were associated with changes in QoL or DD.
These findings highlight the complexity of linking specific intervention processes to multidimensional health outcomes. Engagement with goal-directed intervention activities may be a potential pathway through which REAL-T is associated with improvements in glycemic indicators, while changes in psychosocial outcomes may depend on broader contextual and personal factors not fully captured in the present models. Overall, this finding highlights the value of process-oriented analyses for informing future refinement of lifestyle-focused OT interventions.
Key Messages
Baseline clinical status explained a large proportion of observed change across outcomes, highlighting that initial disease burden and distress levels strongly shape the magnitude and direction of pre–post change in secondary analyses of complex interventions.
Greater attainment of participant-defined treatment goals was associated with better improvements in glucose-related outcomes, highlighting that goal attainment may be a potentially meaningful process indicator within OT-based diabetes interventions.
Few intervention exposure and engagement indicators were associated with changes in QoL or DD, suggesting that these outcomes may depend on broader psychosocial and contextual influences not fully captured by intervention process measures.
Supplemental Material
sj-docx-1-cjo-10.1177_00084174261445818 - Supplemental material for Exploring Treatment Mechanisms of the Resilient, Empowered, Active Living-Telehealth (REAL-T) Intervention
Supplemental material, sj-docx-1-cjo-10.1177_00084174261445818 for Exploring Treatment Mechanisms of the Resilient, Empowered, Active Living-Telehealth (REAL-T) Intervention by Zhixin Liu, Gabrielle Granados, Pey-Jiuan Lee, John Sideris and Elizabeth A. Pyatak in Canadian Journal of Occupational Therapy
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute of Diabetes and Digestive and Kidney Diseases (grant number R01DK116719-01A1).
Declaration of Conflicting Interests
The authors declare no conflicts of interest with respect to this research.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.