
Abstract
This article looks at the arrangements for the care of elderly in Shanghai through the conceptual framework of the ‘care diamond’ and ‘continuum of care’. The findings, that are based on fieldwork conducted by the authors in Shanghai, delineate what constitutes care diamond in the city for the elderly population. This is mapped through the levels of care from home-based to tertiary-level end-of-life services that are needed by the elderly population. It also looks at the emerging markets of care in this sector and discusses whether multiple actors providing a range of services achieve continuum of care for Shanghai’s elderly population.
INTRODUCTION
As the world ages, there is a need to approach ageing and care for the aged as integral to broader questions of changing socio-economic structures. The trajectories of ageing in Asia are very different from the developed world. Unlike the Western countries where demographic transition and economic advancement occurred after industrialisation, ageing in Asian societies presents a varied scenario. Many East Asian countries that fall into the high- or middle-income groups like China, Japan and South Korea have seen demographic transition, which is different from countries in Southeast and South Asia that are lower-middle-income and middle-income societies. Given this variation, the policy response for the care of elderly is also very varied. Living arrangements and support for the older population has posed many challenges in these societies. While there might be lessons to be learnt from the West, policy initiatives have to address the diverse socio-economic and cultural contexts of this region.
An ageing population creates demand on the health services and caregivers within households and supportive institutions. Many countries have separate healthcare policies for older people, and there is diversity in the scope and depth of interventions. Given the variations in the demographic and epidemiological profiles, public investments and effectiveness of health services, and the role of non-governmental organisation and needs of the elderly, there are several models of care across the world.
China, which is now a middle-income country, had 16.1 per cent population over 60 years of age in 2016 (Xinhua 2016). In China, the challenges are further compounded by rapid urbanisation and changing family structures. The outcomes of the one-child policy has created enormous stress for the family that provides care and support for them. Services responding to differential needs of the elderly are provided by the government, for-profit, non-profit and partnerships between them. There is significant subnational variation, given significant regional disparities, urban–rural dichotomy and inter- and intra-provincial differences in socio-economic status.
CARE FOR ELDERLY: THE CONCEPTUAL FRAMEWORK
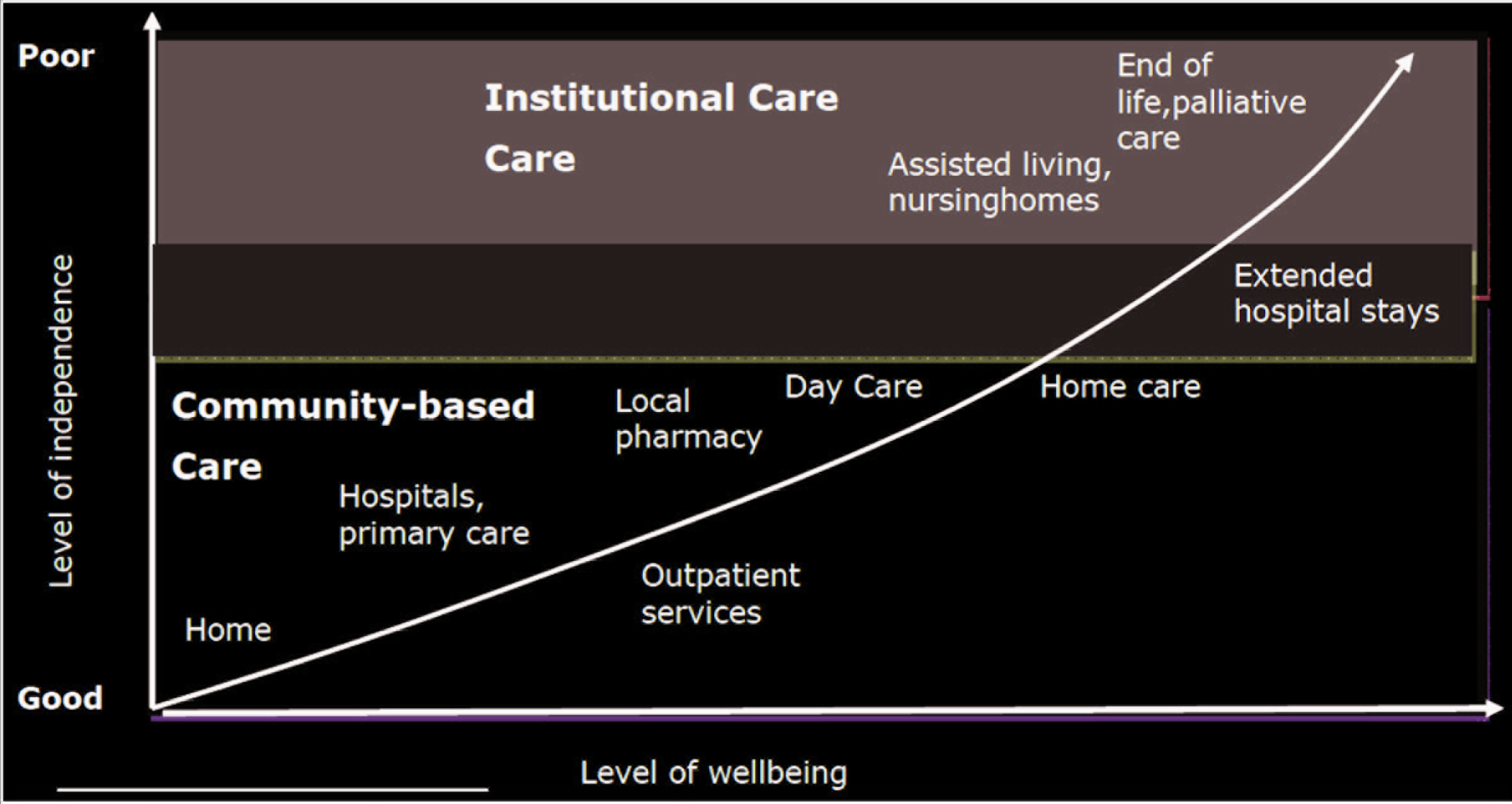
The term care for the elderly in its broadest sense includes preventive, promotive, curative and rehabilitative services. In addition, home-based nursing support and a range of other technical caregivers become necessary since co-morbidities develop as ageing progresses. Therefore, caregiving for the elderly includes a continuum of the family, health service institutions and policies for a range of social services. Figure 1 explicates this continuum in the health services for an understanding of the institutional arrangements for effective care for the elderly.
While health services play an important role for attending to morbidities, the care for elderly goes much beyond, to embrace social provisions like pensions, food security and other forms of social support. This diversity of institutions and actors in this continuum of care is explicated by Razavi’s ‘Care Diamond’ (see Figure 2).
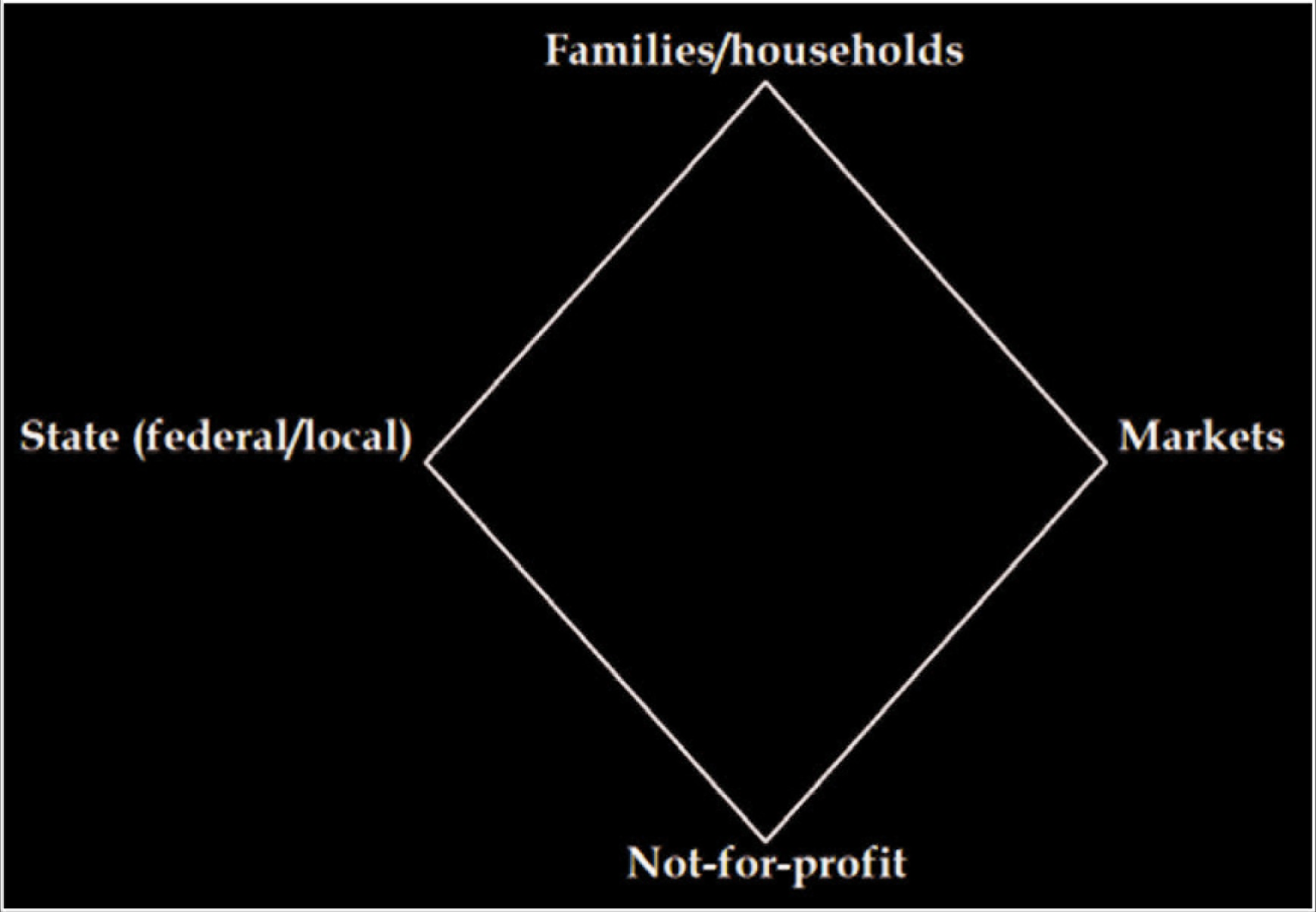
The institutions involved in providing care are conceptualised in a care diamond with four points depicting the state (federal/local), markets, family/households and not-for-profit (Razavi 2007). There are no fixed boundaries between these institutions, and people navigate across these institutions seeking care.
This article will look at ageing in China and arrangements for the care of elderly with specific reference to Shanghai. It will examine this through the lens of ‘care diamond’ and ‘continuum of care’ in Shanghai, an urban city which provides the best-case scenario of care for elderly in the Chinese context. This article focuses exclusively on care in an urban setting for two reasons. First, the rapid urbanisation and rural-to-urban migration poses challenges for meeting the health needs and access to health services to the population. Second, the urban sector is home to many innovative practices and new experimental initiatives in health and social service delivery for older people in this context. The challenges in provisioning of health services in urban areas and innovations in meeting the needs of the elderly population in Shanghai may provide useful insights.
The findings are largely based on primary data derived through key-informant interviews and observations during a 2-week field study conducted in March 2018 in Shanghai. The typology defined by the care diamond will be used to map the diverse actors and institutions providing care to the elderly population in Shanghai. It provides insights into how the municipal government of Shanghai plans and delivers health and social services to this group.
SOCIAL CARE AND HEALTHCARE SERVICES IN THE CHINESE CONTEXT
China has made some dramatic leaps over the past four decades since its economic reforms and opening up to the world in 1979. Along with the economic transformations, the Communist Party of China (CPC) took some dramatic decisions towards social reforms, like implementing the one-child policy in the early 1980s to slow population growth. Fertility rates that are indicators of demographic transition dropped to 1.6 births per woman in 2012, much below the replacement rates. Due to rapid economic growth and resulting migration and urbanisation, there has been a rise in income levels, change in family structures, increase in life expectancies along with widening disparities and inequalities. The market reform policies had far-reaching impact on social and economic life in China. While the demographic transition was determined by the economic and social changes in any society, the transition itself has had profound social, economic, psychological and ideational implications for society. One of the consequences has been the increase in the proportion of older population and a significant number of whom need care.
Care in the Chinese context, as in other Asian countries, is based on support provided by family. Confucian beliefs of filial piety, love, support, duty and respect are integral values. These ‘values’ have weakened over the past few decades with smaller and fragmented families that are unable to support the elderly, as in any other Asian society. Family structures have witnessed rapid transitions in China due to the one-child policy and rural-to-urban migration. Many elderly now live alone, more women than men, as the former have higher life expectancies. In China, the 4:2:1 ratio is what defines the family structure—four grandparents, parents and the single child. The single child has to, in effect, take care of six elderly people. If the single child travels for education or work to some other province or country, then the elderly parents and grandparents are left to take care of themselves. On the other hand, in rural areas, the grandparents look after left-behind grandchildren, while the middle generation migrates to other provinces in search of work. In 2013, the CPC announced that it would prosecute children for neglecting their parents and re-emphasised traditions of ‘filial piety’ and ‘honour’ (Zevallos 2013). Policies for elderly emphasise on family values and stress on situating care within families, thereby placing the primary responsibility of caring on families.
State-driven programmes and interventions are a reflection of how the state perceives its citizens, especially those who are no longer perceived as a productive asset. The Chinese have a fairly robust pension scheme and health services that are premised on a universal insurance system. There are wide variations in social security measures and health services across rural, urban areas and provinces in China.
The role of the state in provisioning of healthcare services in China centres around a welfare model in the present times and is very different from what existed during the pre-reform period. With the onset of market socialism and decollectivisation in the 1980s, the comprehensive health service model that had emerged in the late 1970s collapsed (Baru and Nundy 2020). Inequitable access to healthcare services was of utmost concern for the CPC as well as out-of-pocket expenditures for care, which is still high despite universal insurance coverage. Planning for elderly care has been highlighted in the recent 19th Party Congress report (Nundy 2019). Epidemiologically, chronic and non-communicable diseases take the greater proportion of all illnesses, especially in the context of an increase in the percentage of older persons. The hukou (household registration) of an individual determines access to healthcare and, in general, access to welfare services. An individual with a Shanghai hukou is likely to have easier and better access to health and welfare service than the one who has a hukou for a province in central or western China, especially those in rural areas. A migrant in Shanghai will be outside the ambit of insured health services in the city. All these also determine access to services for older persons in China.
The role of markets for elderly care in China has been steadily increasing. According to a report in Financial Times:
China is home to just 30,000 elderly care institutions. Chinese seniors had potential demand for elderly care services worth Rmb500bn ($72bn) last year, but supply fell short of that demand, according to analysts at Chinese brokerage Everbright Securities. China’s senior care industry as a whole is still in its infancy, no replicable project models and large-scale market leaders have emerged. A falling birth rate in China means that by 2050 a quarter of China’s population is forecast to be over 65 years, a process that will challenge social norms in a society where aged care has typically been provided by family members. About 90 per cent of Chinese seniors rely mainly on family support, 7 per cent on residential community-based care services and 3 per cent on nursing homes. (Smyth, Wang and Hanock 2019)
Hence, the differential needs of the elderly present a challenge for the state to provide comprehensive services and social security in the form of pensions, healthcare (physical and psychological) and long-term care. Day-to-day care of old citizens, who do not have support and are unable to look after their needs, is of critical concern.
SHANGHAI AND CARE FOR ELDERLY
The administrative district of Shanghai had a total population of over 26 million in 2019 across 16 districts. The population of people above the age of 60 years is about 5 million. As per the World Health Organization (WHO), the number of people above the age of 65 is 2.8 million. Number of people above the age of 80 is 870,000 and number of people above the age of 100 is about 2,000. In Shanghai, 33.2 per cent of the household-registered population were elderly, out of which 16.7 per cent of the population were above 80 years old (Hu 2019).
THE CARE DIAMOND
There is plurality of actors and institutional forms in providing care for the elderly in Shanghai at all levels. The constituents of the ‘care diamond’ include the municipality or the local government that provides healthcare services at all levels—primary, secondary and tertiary. At the primary level, there are services provided by the municipality, for-profit and non-profit organisations, and the family. The community health centres (CHCs) provide preventive, promotive, curative and rehabilitative services. There are for-profit providers who offer services for home-based care. In addition, there are a few non-profit organisations that engage with the elderly in the assisted living centres, community and the home. And finally, there are caregivers within the family and community. At the secondary level, there are elderly care homes and nursing homes managed by the municipality, for-profit, non-profits and also public-private partnerships in all districts. Health service institutions at the secondary and tertiary levels include hospitals and specialist centres. These are all the institutions and actors that constitute the care diamond in Shanghai.
In terms of health services, the role of the municipality is critical, and it also gives some basic security to the elderly by providing a minimum allowance and food. Although the goal of the municipality is to achieve continuum of care, there are many barriers in achieving it. Some of these constraints will be discussed in the following sections.
HEALTH AND SOCIAL CARE FOR THE ELDERLY
Every aged person in Shanghai is given a monthly allowance by the local government. From ages 65–69 years, people are given an allowance of RMB 75. From 70–79 years of age, the allowance is RMB 150. From age groups 80–89, 90–99 and for people over 99 years of age, the allowance amounts to RMB 180, 350 and 600, respectively. The minimum standard of living security for the elderly more than or equal to 60 years of age is RMB 1,400 per person per month. Other in-kind support includes ‘grain and oil help card’, which includes 10 kg of rice, 900 ml oil and l5 kg of sugar. The poor can have ‘food and oil voucher’ every month. For permanent residents who are over 65 years of age, facilities are provided for free physical examination and inoculation of 23-valent pneumonia vaccines (Hu 2019).
In terms of health services, prevention and control of chronic diseases and risk factors are the top priority of disease prevention in the elderly. Regular health check-ups are conducted at the community level to facilitate early detection, diagnosis and treatment. The elderly who are above 65 years of age receive a health management service once a year. This includes lifestyle and health status assessment; physical examination; management or referring of patients suffering from hypertension and diabetes for treatment; and encouraging health education, vaccination, osteoporosis prevention, fall prevention, health guidance, Chinese medicine guidance and self-care service.
NEED ASSESSMENT OF THE ELDERLY FOR LONG-TERM CARE: INITIATIVE BY THE MUNICIPALITY
In 2005, Shanghai put forward an old-age long-term care (LTC) system, which has been incorporated in the existing health insurance schemes for employees and residents. There is an epidemiological approach to planning for long-term care for the elderly in Shanghai. The elderly are divided into six categories, depending on their medical and care needs. The sixth category includes those elderly who need the maximum care and support. There are evaluation tools that have been developed to assess needs of those elderly who desire long-term care. Two evaluators are assigned to do the need assessment, who conduct home visits. One of them is a doctor. The second evaluation can be conducted by a doctor but is often conducted by a nurse or community health worker. The physical capability, the cognitive ability and the disease condition of the applicant are taken into consideration during the process of evaluation. After evaluation, the data is digitally processed. The computer gives a score to the applicant. The grade of the applicant is divided into seven levels (see Table 1). Each level indicates what kind of service will actually be given to the applicant. If the score of the applicant falls in level 0, it indicates that the elderly person does not need the services of long-term care. In the other six categories, there will be a standard service package made available for each category. This includes providing them with support in carrying out day-to-day activities and also medical services. There are a total of 42 services that are provided for helping the elderly. Of these, 24 services pertain to daily life support provided to them, including giving them bath, feeding them, helping them to go to the washroom, changing their clothes, banking assistance, agency services and so on. Adding a few more services like cooking for them in case they live alone is also being considered. Seventeen of the services are medical services like giving injection, regular medicines and so on. When the elderly receive these services, they need to pay 10 per cent out of their pocket. The rest of the amount is paid by the LTC insurance fund. For those living below the poverty line can apply for exemption for out-of-pocket payments (Interview with Ding Hansheng, Deputy Director, Shanghai Health Development Research Centre, Shanghai, 16 March 2018; Ding 2019).
Categories for determining LTC
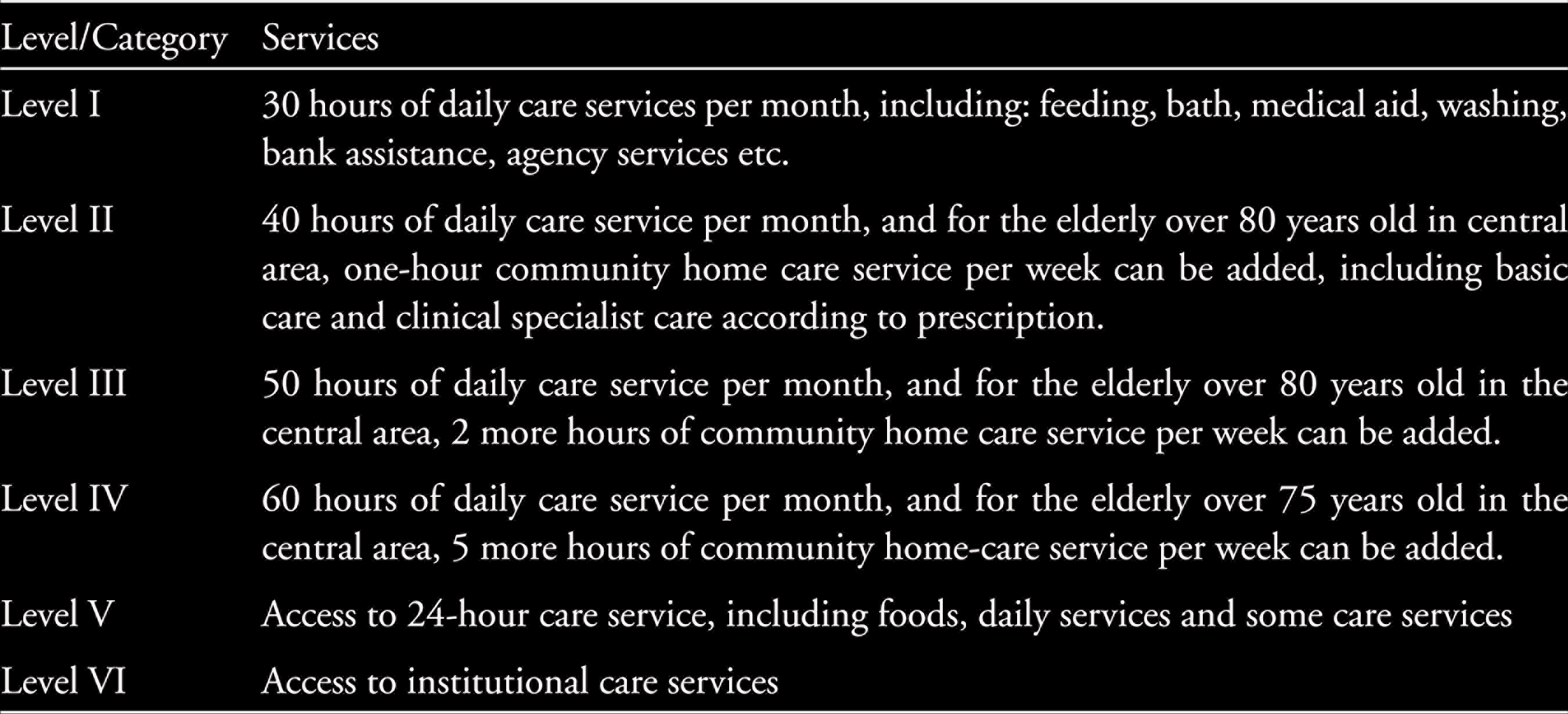
Through this need assessment, 20,000 residents have been included for LTC since 2013. Of these, 10,000 older persons are looked after in their homes and communities, 5,000 live in nursing homes and the remaining 5,000 are in CHCs or hospitals. There is a broad consensus among planners about the need to develop a unified assessment tool to categorise the differential needs of the elderly. This tool has taken seven years of research, to identify daily life capabilities and the development of disability among the elderly. The six categories have been determined in this process. Currently, this need assessment tool is being utilised to assess the 5 million elderly people in Shanghai. This need assessment tool that is unique to Shanghai has now been extended to Jiangsu, Zhejiang, Jiangxi and many other provinces and cities (Ding 2019).
Given the fact that a substantial percentage of the elderly stay in their homes, there is a growing need for home-based care. The municipality is unable to meet this need since caregiving requires a trained workforce. This shortage of home-based care has created the potential for markets to enter these services, and this has been on the rise in China, especially in first-tier cities like Shanghai. The government insurance schemes cover expenditure incurred for home-based care, so there is a market for such services.
Expenditure for medical care is reimbursed by the universal medical insurance system. Shanghai is attempting to establish a comprehensive system to subsidise the elderly and disabled elderly by combining various dimensions of medical care and preventive services.
ROLE OF THE COMMUNITY HEALTH CENTRE
The CHC by the municipality plays a central role in the lives of the elderly in Shanghai. There are 330 CHCs at the primary level, each CHC is for an average of 80,000 people, and many of these CHCs also provide outreach services, including home-based care for the elderly. A CHC is available at a 15-min walking distance for all citizens. Every CHC has an elderly ward and some among these have end-of-life care wards as well.
The CHC is integral to the lives of the people, but human resources are skewed towards the secondary and tertiary hospitals. Above the CHC, there are the district hospitals and city-level hospitals that provide specialised health services. The health resource distribution is skewed towards higher level of facilities. In Shanghai, about 84 per cent beds are in the hospitals, whereas the number of beds in the CHCs accounted for only 14 per cent of the total. The case is similar with the distribution of health professionals, where about 75 per cent of them are in hospitals, and 17 per cent work at the primary level (Zhu 2019).
The researchers visited a CHC in Minhang, which is a suburban district of Shanghai. There are many factories in the district, and the residents are mostly workers employed in these factories. The district provides an interesting case study of continuum of care. There are four survey stations that are located inside the communities and are linked to the CHC for referrals. The survey stations are mainly for preventive services. There is a General Practitioner (GP) at each survey station who provides basic curative services. They have a nurse who maintains data for all patients. There are basic surveys on blood pressure, cancer screening and the rest. GPs are available everyday in survey stations. They even go once a week to the communities and the patients’ homes if required. The difficult cases that the survey station is unable to handle are referred to the CHC. There are a total of 13 CHCs in Minhang district, and all CHCs have end-of-life care. There are a total of 150 beds for the end-of-life care in the entire district. In Shanghai, not all CHCs have end-of-life care wards. There is a waiting list, and beds are not enough. Therefore, professional nurses provide home care through these institutions. Based on the need assessment conducted at the district level for long-term care, patients who have maximum 3 months to live are referred to the end-of-life care unit. These are mostly those suffering from cancers. As with other services, 90 per cent of these expenses are covered by social insurance and 10 per cent is out of pocket.
PALLIATIVE AND END-OF-LIFE CARE AT THE COMMUNITY HEALTH CENTRE IN SHANGHAI
Palliative, end-of-life and hospice care originated in the West sometime in the middle of the twentieth century by the nursing profession. WHO defines palliative care as
an approach that improves the quality of life of patients and their families facing the problems associated with life-threatening illness, through the prevention and relief of suffering by means of early identification and impeccable assessment and treatment of pain and other problems, physical, psychosocial and spiritual. (WHO, 2020)
Palliative care can be given at any point in time for chronic, life-threatening illnesses and also during end-of-life in the case of terminally ill patients. Palliative care during end-of-life includes easing pain, providing comfort to the patient and also psychological support to patients and their families. The team for palliative care draws expertise from multidimensional fields with an interdisciplinary approach. The team consists of doctors, nurses, counsellors, social workers, psychologists and volunteers.
The cultural meaning of dying and death had an influence in the end-of-life services that eventually developed in China and is still in the process of defining itself. For China, developing palliative, and especially hospice, care was a gradual process that took over 24 years. Traditionally, talking about death of a family member was seen as a taboo that would bring bad luck. There were resistances from within the profession itself apart from resistances from the society. In the beginning, several models were studied from the West as well as other East Asian countries, on the basis of which China developed its own model. During the field visit, we were informed about the development of palliative care in China. At the national level, there is a continuous education programme on palliative care where physicians and nurses receive training. There is acknowledgement among the professionals that hospice approach does not have only a medical role, but humanities plays an important role in understanding the needs, emotions of patients, family and the community. Palliative care has developed into a discipline, but, in hospitals, some groups of doctors still prefer treating and looking for cure. The tension between those who feel there should be supportive services for people who are terminally ill and those who feel that trying to cure till the end is necessary is still prevalent. The professionals feel that it is important to educate the next generation of doctors, of the philosophy of palliative care, especially with respect to end-of-life care so as to influence their colleagues when they start working as doctors.
During the field visit to Shanghai, the researchers got the opportunity to see the model of palliative care in the context of end-of-life care being implemented by the local government. They visited an end-of-life care department at a CHC in one of the central districts. There is a separate ward for end-of-life care, for patients who have 3 months or less to live. There are 26 beds in the ward, which gets 200 patients annually. Most patients in the ward are suffering from cancer. This programme was introduced in China in the 1990s. The ward that we visited was one of the first ones that was started in 1995 by the municipality as a pilot.
The overall programme objective is to ease pain, maintain dignity in death and to provide with positive physical and psychological assistance for the dying. Psychological assistance and support are extended to the family too. The personnel include GPs who have a training in dealing with cancers; specialty nurses; medical social workers who mobilise resources and provide counselling; consultant psychologists for patients and family members; nutritionist; rehabilitation specialist; and volunteers from the student community, mainly from primary and middle schools and also consulting lawyers who provide special legal services.
Prioritising patients who need entry into the palliative ward depends on the assessment of the patient condition that is conducted by the team. There are three levels of categorisiation—people in Level I are advised to make outpatient visits; those in Level II are requested to stay at home and are provided with home care services; and, in Level III, if the score estimates less than 3 months of life, the patient is admitted in the ward till death. If during the stay at the ward, some patients tend to improve with treatment, they are referred to a tertiary public hospital for further treatment. After admission, case-by-case assessments are made for care support. Nurses decide if social workers are necessary for intervention. The estimated time left for the patient is conveyed to the family members and the patient to help them prepare.
Most of the activities of the staff are focused on easing symptoms and attempt to control pain related to cancers. These are mainly related to vomiting, breathing and pain, and the latter also includes administering morphine along with support of traditional Chinese medicine (TCM), hydration therapy and continuous psychological support. Nurses take care of original site of cancer and wounds associated with it. Social workers along with psychologists assist in dealing with different emotions and anxieties linked to impending death. Social workers help patients to decide things they wish to complete before they die and assist patients in completing these tasks—these include legal and financial help among other things. Family is provided with continuous support, if they require, even after the death of their family member. The idea is to keep the ethos of the traditional Chinese culture that is followed at home so that the patients do not feel alienated at the time of death. Social workers also encourage patients to recall their lives and write stories with photos as memories. There is celebration of birthdays and anniversaries with photos that depict the full life of the patient. This helps the patients to express their emotions and also develop their will to fight pain and accept death. It is also a way to reconcile with life and unlock lost relationships with friends and relatives. The idea that patients are able to pass through life peacefully without regrets is taken seriously, and efforts are made towards this. Patients could also express their desire to donate to the community.
There are classes that are structured to handle difficult issues with patients and family members. The first session is to understand themselves and to realise the need for self-help and accept assistance. The second session involves talking with family members about unmet needs with patients and helping them in not holding back or harbouring any regrets. It is a way of seeing that there is positive communication between patients and their families. The third session is for family members so as to help them to say goodbye and deal with the grief after the death of the family member. These services can continue from 1 to 12 months, depending on the need of the family. The fourth session is for relatives to reconstruct life after death of the patient and rebuild themselves to cope and get back to life.
There are trained social workers, and there are many volunteers who come from the community; some of the volunteers are also those who have lost a family member. Children from welfare institutions and orphanages also visit the CHC and work as volunteers. There are special programmes that they organise during the spring festival for the patients. This programme also incorporates sociocultural education base for young children so as to teach them about life and death, and that death is an integral part of life and the impact one’s life has on others. This provides an opportunity for the old and young to communicate with each other.
In the final few days of their lives, the patients are shifted to another exclusive room where the family members can also stay. Social workers accompany the family here. After death, many family members continue to be in touch with social workers, and there are special sessions held to help them get through the difficult period of loss. There is a support group where families, social workers and volunteers meet regularly. For caregivers in a hospital setting, there is fatigue that sets in after taking care of patients. There is an emotional burn out—in such cases, social workers have to counsel medical professionals too. The palliative care professionals are guaranteed respectable income and are sent abroad for training and are given breaks to travel.
The overall philosophy of the institute includes care, improving quality of end-of-life and dignity in death being a right of everybody. The idea is to deal with the life cycle, from birth to death. Long-term care at home or home care of terminally ill patients has been a bottleneck. Home settings have several challenges, and there are municipal standards for home care that not many are able to achieve. There are several services such as nursing, diagnosis, electrocardiogram (ECG), TCM and others for home care, but it is difficult to control risks at home. Regular morphine administration for pain relief has its risks and cannot be given at home. Family members are sometimes allowed to, but there are strict regulations, where caregivers get the morphine from the hospital and have to deposit the vial back to the hospital once administered.
The caveat here is that this is one of the economically well-off districts, and such wards are still not universal across Shanghai. There are long queues, as many elderly are in need of end-of-life care.
FOR-PROFIT HOME-BASED CARE MODEL
A field visit to a private home-based care company gave insights into the development of a home-based care business model in Hongkuo district in Shanghai. The promoter of this enterprise had a Master’s in Business Administration from Japan. He subsequently worked in a logistics and home care company in Japan. The home care companies in China are modelled on the Japanese care models. While discussing the motivations for starting such a company, Mr Li (name changed) said that,
in our generation we are all single children—so was the case of Japan. Our parents were left alone. Many families were like us and it was a social problem. Society in China needs private services, since there are not much efficient public services. My mother died of cancer when I was 20 yrs. That time we were caring for her but could not care properly—she had bed sores and we didn’t know what to do. I wanted to do something for the elderly. (Interview with Mr Li, private investor, 13 March 2018, Shanghai)
Mr Li started the company in 2011 when he realised there would be a demand for the care of elderly. According to him, the caring for the elderly was not only a social problem, but it also presented a business opportunity. In Japan, medical care for older people became costly, and public medical insurance could not keep up with addressing medical care needs. So, there was a conscious effort to develop efficient systems for home-based care, in order to save hospital costs and provide comfort at home, for older people. There were no private entrepreneurs providing home-based services in China. His company is among the first in Shanghai to provide home-based services. Initially, he started with his own investments and now he has a domestic investor. Japanese investors were also willing to invest, but the Sino-Japanese relations were not conducive for investments in this sector. The company has 34 branches across 15 districts of Shanghai. The business model is simple. They hire people and train them and send them to homes where the elderly require care. The financing of these services is 80 per cent by the government and 20 per cent is out-of-pocket. Overall, 90 per cent of visiting nursing charges are covered by government insurance schemes and 10 per cent out-of-pocket. Staff of the home-based care include nurses, who are professional with 5 years training (3 years of experience in hospitals); physiotherapists; doctors of general medicine; social workers; paid volunteers; 700 helpers or assistant nursing staff; and some health workers trained in TCM.
This company provided home-based services to 7,000 elderly in 2018. The plan is to increase the coverage to a population of 20,000 and have 50 branches all over Shanghai. Mr Li said that this venture is not very profitable with profit margins of around 10–13 per cent. This is because home-based care is labour intensive and around 60–62 per cent of the company’s expenditure went on staff salaries. Availability and quality of human resources are two of the major challenges facing the business. Since majority of caregivers are from Shanghai, higher salaries need to be paid to the workers. There is also a problem of high turnover of caregivers and other categories of professionals. The company invests in training them on the job but has difficulty retaining them. 1
ASSISTED LIVING RESIDENTIAL FACILITIES
Shanghai municipality has entered into joint ventures with private real estate companies to build homes for the elderly.
The services of these companies are targeted towards middle and upper middle classes. Needs of the clients include medical nurse, physical therapy, body care and providing cooked food. The company has eight day-care centres where they conduct medical check-ups, activities, therapy, training for brain/memory, body care and Tai-Chi. The day-care centre also contracts a food company to provide cooked food to the elderly and also reach out to the elderly who need cooked food in their homes.
These services and support structures that reach out to help the elderly at home are, indeed, critical but are still limited in Shanghai and are gradually expanding. There are many elderly care homes in Shanghai that fulfil the need for long-term care.
ELDERLY CARE HOMES IN THE DISTRICTS: PRIVATE AND PARTNERSHIPS FOR LONG-TERM CARE
The Shanghai municipality is attempting to provide continuity of care from home care to institutional support as seen in the previous sections, but, clearly, the demand for long-term care of older persons exceeds what the government is able to supply. To lessen this gap, all districts have nursing homes and elderly care homes run by the private as well as those set up as partnerships between the public and private. In terms of care institutions, by the end of 2017, there were 703 old-age institutions (public, private and those in partnerships), 127 nursing homes and 140,400 old-age beds across levels of care.
There are three types of elderly care homes in each district of Shanghai—municipal homes that are few, non-profit institutions and those that are public–private partnership (PPP) models, where the private sector (non-profit in most cases) partners with the district municipality, and invests at various levels, mostly management of the home and contracting-in of human resources.
The researchers visited two elderly care homes in two districts—Xuhui and Jing’an, which are the well-off districts of Shanghai. The welfare houses mostly take in elderly who fall in the last three categories after the need assessment is done, where the sixth category would include those elderly who need the maximum care and support. In many cases, the very old are unable to live alone or their children who are ‘young-old’ are unable to take care of them. They are moved to a care home within their home district. Many are unable to go to the privately run homes that are expensive and are mushrooming. In these instances, the elderly either go to municipal homes at the district level, which are few in number or to the non-profit homes that have emerged in partnership with the municipality. These homes can be seen as extensions of the community.
Both the old-age homes in the Jing’an and Xuihui districts are PPPs, where the building and the land are owned by the Shanghai municipality, while the private agency manages the institution and its regular operations. The care services include medical services, rehabilitation centre, TCM healthcare, geriatrics research base and other services.
In the Jing’an care home, the private company employs the doctors and other staff—80 in all. They have a pharmacy. Similar to other institutions, 90 per cent of the long-term care services is paid by government and 10 per cent is out-of-pocket. They have both inpatient and outpatient services. At present, there are 216 patients in the home—90 are men and rest women. The age of the elderly ranges from 80 years to over 90 years.
Each floor is categorised in terms of the needs of the elderly. For instance, the second floor has the elderly who cannot take care of themselves at all. There are separate wards for very ill patients. On the third floor are the elderly who are mobile and can take care of themselves. Every room has one nurse. There are volunteers from the community. There is a separate day-care centre where the elderly from the community come during the day and spend their time there. They can eat one meal and pay RMB 15. They go home by evening. On a given day, there are 4–5 older people in the day care. There is a daily activity chart and food chart for all days. In case they do not like the food, they can buy separately and eat. The old-age home is quite large with 5–6 floors with a rooftop where vegetables are grown. It is located in one of the central districts of Shanghai. It is very well-lit and bright, and the architecture is suited to the requirement of more natural light. The elderly in these homes have to pay for the bed themselves—RMB 6,000–7,000/month, which is very expensive. Many of these homes are thus accessible to very few elderly residents in the districts who can afford the costs.
There are many foreign and domestic investors who are keen to invest in services for the elderly. This is due to the large number of the elderly population, which is a potential for profits. For instance, Australian operators, Lendlease, a Sydney-based property group will launch four senior housing projects in China, starting with Shanghai which is estimated to be a AUD 28 million project. Beijing opened the elderly care sector to foreign investors in 2014, including wholly-owned by foreign investors. Many of these investors had little understanding of what senior living would be like in China. Their main focus has been to understand the market and expectations of the government and the society (Smyth et al. 2019).
CONTINUUM OF CARE FOR OLDER PERSONS IN SHANGHAI: GAPS AND CHALLENGES
To sum up, majority of the elderly residents of Shanghai live in their homes and are covered by a variety of insurance schemes and services. Medical care is provided by the CHC, which happens to be the closest to the community, and hospitals which are financed by the universal health insurance scheme, and additional coverage is provided for long-term care. There is still considerable out-of-pocket expenditure. The gaps that arise out of public financing and provisioning are addressed by commercial enterprises, given the class dimensions that determine differential needs. Markets have emerged in all levels of care for the elderly and cover pensions, medical insurance, healthcare, home-based care, assisted living, hospice services and old-age institutions. Given the fact that Shanghai municipality is among the richest in terms of standard of living and revenues earned, it is a hub for the emerging markets.
There is clearly a fragmented system of financing and care for the elderly in Shanghai, with varied actors and institutions across sectors, providing services that constitute the care diamond. These services are not integrated or comprehensive, and there are multiple authorities and governance structures. Therefore, this falls short of a continuum of care for the elderly. No doubt the Shanghai municipality is building towards reaching this continuum through integration of services from addressing primary needs to tertiary-level needs of the elderly, but there is a lot yet to be achieved. The Shanghai model of care for the elderly is important to understand, especially for Asian cities in the present context. There are lessons for what continuum of care should entail in the context of an ageing population.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The field study was part of a larger project titled ‘Commercialisation of Elderly Care in India and China: Case of Delhi and Shanghai’, funded by the Indian Council for Social Science Research, New Delhi (2017-19).