
Abstract

Case
An 8-year-old boy with a history of repaired tetrology of Fallot, and failure to thrive status post gastrostomy tube (G-tube) for the first year of life, presented to the Pediatric Emergency Department complaining of bilateral hand and foot swelling. Approximately 2 weeks prior to presentation, he had noticed leakage from his prior G-tube site that had fully closed 7 years ago after removal when no longer needed. Over the past 2 weeks, the patient experienced increased leakage from the G-tube site, occurring primarily with movement and oral intake, and associated with mild crampy abdominal pain.
Three days prior to presentation to the Pediatric Emergency Department, the patient began to complain of lower extremity pruritis, bilateral swelling of his ankles, pain when walking, and mild swelling of both hands; these had been gradually increasing over the past three days. Review of systems was notable only for clear rhinorrhea, sore throat, and cough. He had no fever, urinary symptoms, periorbital or scrotal swelling. The patient was afebrile with vital signs within normal limits and examination at the time revealed marked edema of the lower extremties bilaterally up to the level of his knees and mild edema of the dorsal surface of his hands and wrists. He had pain with active and passive movement of his feet and wrists and had a noticeable limp while walking. On dermatological examination, he had raised purpuric papules of 1 to 2 cm over his ankles, feet, and the lateral aspects of his lower legs, as well as flesh-colored raised papules over his medial upper legs. His perineum and buttocks were not involved. Over the course of his emergency department visit, he developed 1-cm purpuric lesions over the dorsal aspect of his hands bilaterally. There was yellow drainage from the former G-tube site with no visible opening. The surrounding skin was without erythema or induration. His abdomen was nontender, nondistended, with normal bowel sounds. Neurologic exam was within normal limits.
A complete blood count was obtained that showed a white blood count of 6410/mm3, hemoglobin of 12.4 g/dL, and platelets of 329 000/mm3. His C-reactive protein was 1.7 mg/dL and erythrocyte sedimentation rate was 10 mm/h. His complete metabolic panel was unremarkable, including a serum creatinine of 0.6 mg/dL, total protein of 7.3 g/dL, and albumin of 4.3 g/dL. The prothrombin time and activated partial thromboplastin time were within normal limits. His urinary analysis was notable for an absence of proteinuria or hematuria. Occult blood was not found in the stool. A bacterial surface culture of the fluid from the G-tube site showed light skin flora and group B Streptococcus. A throat culture was positive for group A Streptococcus.
An abdominal ultrasound of the former G-tube site demonstrated no abscess or visible fistula. A lower extremity ultrasound ruled out deep vein thromboses. The pediatric dermatology service was consulted and thought his skin findings to be most consistent with acute hemorrhagic edema of childhood, although Henoch–Schönlein purpura (HSP) could not be excluded. He was discharged home with a prescription for penicillin to treat streptococcal pharyngitis and antihistamines with topical steroid cream for the pruritis. At this time there was no explanation for his new onset of leakage from his former gastrostomy site.
The patient presented to an outpatient pediatric clinic 5 days later with increasing drainage of yellow fluid from his former G-tube site and worsening rash. Examination of his skin revealed bilateral deep purple palpable purpura extending from his feet to upper thighs on the anterior, lateral, and posterior aspects, with sparing of his buttocks. He had been compliant with the medication prescribed during his emergency room visit. With the progression of his rash, pediatric dermatology was reconsulted and both the dermatology team and the primary care team agreed that his presentation was consistent with HSP. Urinalysis at the time was unremarkable.
Because of the continued drainage from his former G-tube site, an upper gastrointestinal series was performed. No definite fistula was seen on imaging; however, the swallowed barium was seen leaking from his former G-tube site at the end of the study consistent with an enterocutaneous fistula. The remainder of the study was unremarkable. He was taken to the operating room for laparoscopic evaluation at which time a gastrocutaneous fistula tract to his former G-tube site was isolated and corrected without complication. Pathology of the specimen showed both squamous epithelium and gastric mucosa, as well as evidence of transmural acute and chronic inflammation, consistent with a gastrocutaneous fistula and inflammation that can be seen in HSP (Figures 1 and 2).
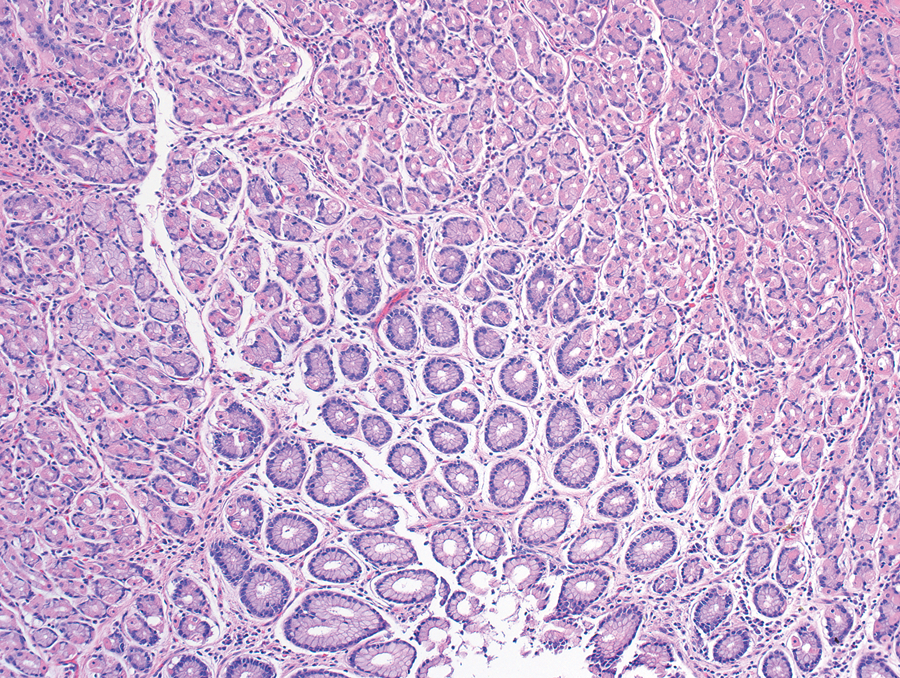
Fistula pathology specimen at 40× magnification, notable for presence of gastric mucosal cells
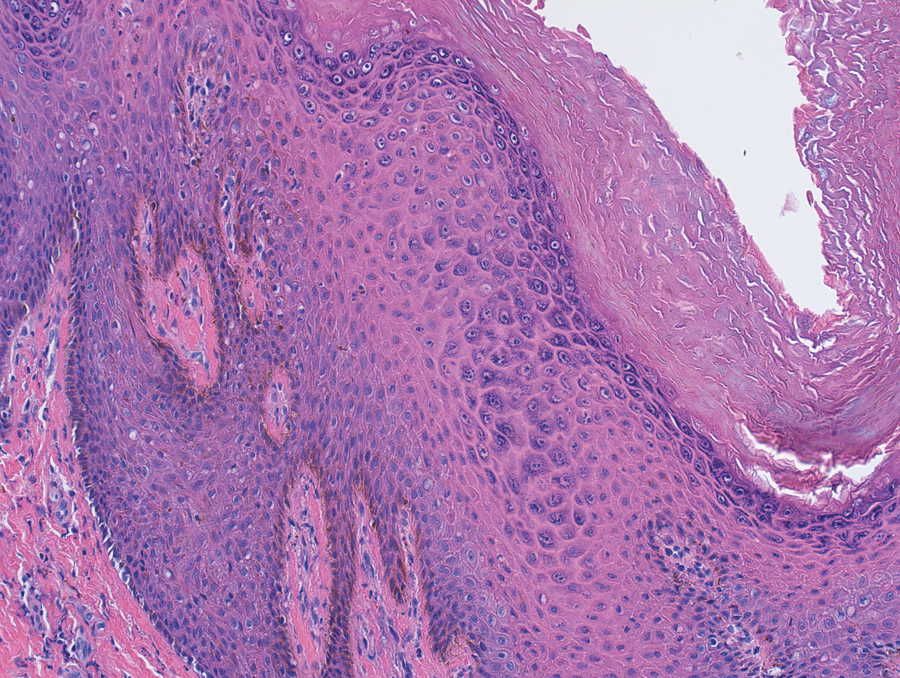
Fistula pathology specimen at 64× magnification, notable for presence of squamous epithelial cells.
The patient went on to recover fully from his HSP over the next few months, currently without recurrence or development of any renal consequences. The drainage from the G-tube site did not recur. A gastrocutaneous fistula was the first presentation of HSP, with classical symptoms subsequently developing.
Discussion
Henoch–Schönlein purpura is a small vessel vasculitis that often presents with the triad of arthritis, abdominal pain, and and palpable purpura. Although all patients will have cutaneous purpura, the other symptoms of arthritis, abdominal pain, and renal involvement do not occur in all patients, making the diagnosis of HSP more challenging. 1
Although palpable purpura are often considered the hallmark of HSP, skin findings are not the presenting feature in nearly 25% of patients. Furthermore, early skin findings may not resemble the classic purpuric rash. The rash may evolve from urticarial wheals to crops of purpura more than 10 mm in diameter, also changing in color from red to purple before fading without intervention. 2 The rash usually appears on dependent portions, such as the lower extremities and buttocks; however, as seen in our patient, the buttocks can be spared.
Gastrointestinal findings are present in 45% to 75% patients with HSP, 3 with 14% to 36% of patients developing these symptoms prior to the appearance of purpura. 4 Patients most commonly develop abdominal pain without surgical complications. The most common surgical complication reported is intussusception,5,6 but bowel ischemia and infarction, perforation, strictures, fistulas, hemorrhage, pancreatitis, and appendicitis are infrequently seen.
In this case, the patient had minimal abdominal symptoms, presenting with leakage from his former gastrostomy site. To date, there have only been 2 reported cases of entero–entero fistulae formation,7,8 and no reported cases of enterocutaneous fistulae. Furthermore, both reported cases involved the small bowel. A gastric fistula in HSP has not been previously reported. It is thought that there may be underdiagnosis of internal fistulae because they often do not cause symptoms, nutritional deficiencies, electrolyte imbalances, or fluid losses. Furthermore, administered steroids may mask symptoms. 7 Intra-abdominal manifestations are thought to be a result of submucosal and subserosal edema and hemorrhage.4,6,7 We theorize that the presence of a prior gastrostomy site in our patient represented a predisposed area of weakness in the gastric wall and soft tissue, and that gastric vasculitis with edema caused by HSP resulted in a fistula tract.
Here, we present the case of an 8-year-old boy with HSP whose presenting symptom was leakage from a former G-tube site, later found to be an enterocutaneous fistula. This case represents an important addition to our understanding of gastrointestinal involvement in HSP.
Footnotes
Acknowledgements
Special thanks to Dr Michael O’Malley of the Johns Hopkins Surgical Pathology Department for his guidance in this case.
The author(s) declared no potential conflicts of interests with respect to the authorship and/or publication of this article.
The author(s) received no financial support for the research and/or authorship of this article.