
Abstract
Objective. To assess primary care pediatricians’ (PCPs’) perceptions of caring for children and youth with special health care needs (CYSHCN). Methods. Cross-sectional survey of Illinois pediatricians. Results. Thirty-five percent of surveys were returned and 26% were analyzed. The top 3 perceived barriers were insufficient time (72%), insufficient reimbursement (68%), and lack of support services (59%). Insufficient interest was the least cited barrier (19%). Preparedness to perform tasks related to care of CYSHCN ranged from 89% for accessing early intervention services to 24% for billing and coding. The percentage of PCPs somewhat or very comfortable providing primary care to patients with technology dependence ranged from 75% for blood glucose monitoring to 12% for dialysis. Conclusions. The issues of time, reimbursement, billing, and coding are perceived as significant barriers to the care CYSHCN. There is substantial variation in PCPs’ comfort in the care of CYSHCN who require the assistance of medical technologies.
Keywords
Introduction
Children and youth with special health care needs (CYSHCN) are described by the Maternal and Child Health Bureau (MCHB) as “those who have or are at increased risk for a chronic physical, development, behavioral, or emotional condition and who also require health and related services of a type or amount beyond that required by children generally.”1(pp 138) There are approximately 10.2 million such children in the United States today. These 14% of children disproportionately consume 40% to 80% of pediatric health care expenditures.2-8 CYSHCN and their families have high levels of unmet medical, financial, and emotional needs.3,9,15
In 2002, the American Academy of Pediatrics adopted a policy statement on the medical home, encouraging primary care practices to be accessible, continuous, comprehensive, family centered, coordinated, compassionate, and culturally effective for all children, especially CYSHCN.16,17 In several demonstration projects, the medical home has been shown to reduce emergency department utilization, delays in care, unmet health care needs, and overall costs for CYSHCN and others.18-22 However, implementation of the medical home for CYSHCN has been limited. Of all CYSHCN who required care coordination, only about 40% of families reported their care coordination as adequate. Furthermore, among those who received care coordination, only half of families considered communication among their physicians to be good or excellent. 20
There has been little examination of why implementation of the medical home for many CYSHCN has been incomplete. The limited literature cites factors such as lack of training on prescribing physical, occupational, and speech therapies; lack of knowledge; lack of family support services; and costs.16,20,23-25 However, there has been no systematic attempt to assess primary care pediatricians’ (PCPs’) perceptions of the relative importance of various barriers to caring for CYSHCN, nor has there been any attempt to determine relative PCPs’ comfort performing specific tasks associated with caring for these children or preparation to provide primary care to CYSHCN as compared with typically developing children who develop typically.
The purpose of this study, therefore, was to assess perceptions of PCPs in caring for CYSHCN. Specific objectives were to assess the barriers PCPs perceive in caring for this population, their preparation to perform various tasks associated with the care of CYSHCN, and to determine for which types of patients PCPs feel comfortable providing primary care.
Methods
This study was a cross-sectional descriptive study. A survey was mailed to all pediatricians listed as primary care physicians on the Illinois Chapter of American Academy of Pediatrics (ICAAP) address list. The survey was designed specifically for this study and was based on the New England SERVE Shared Responsibilities Primary Care Provider Survey, a survey designed to find PCPs’ experiences and satisfaction in providing care to CYSHCN, and the Illinois Medical Home Project, described later in this article.26-28 There were 2 paper mailings and 2 e-mail reminders. A $2 bill was included in the initial mailing as an incentive. The study was approved by the institutional review board at Children’s Memorial Hospital as an exempt protocol.
The survey results were recorded anonymously. ICAAP staff delinked the completed surveys from return envelopes before data entry. Data were entered by hired staff, cleaned, and then analyzed by the primary investigators.
The survey consisted of 20 primarily multipart questions. The survey reproduced the MCHB definition for CYSHCN and instructed participants to use this definition for the purposes of survey response. The first section surveyed provider characteristics including gender, year of residency graduation, type of residency program, participation in the state of Illinois’ Title V CYSHCN certified medical home provider program, as well as participation in the Illinois Medical Home Project, a multiyear, intensive, practice-level quality improvement initiative funded by the Maternal and Child Health Bureau. Practice characteristics examined included location (by zip code), setting of practice (ie, office based, hospital based), and number of providers. Respondents were also asked to estimate the number of children, number of CYSHCN, and percentages of various racial and payer classes served by their practices. Participants rated their perceptions of 16 barriers, 14 tasks, and 16 medical technologies related to caring for CYSHCN on 4- or 5-point Likert-type scales. CYSHCN were defined for participants on an attached cover letter using the MCHB definition. 1 The final survey took approximately 15 to 20 minutes to complete.
Personal and practice characteristics were recoded into categories meaningful for analysis. Stata 9.0 (College Station, TX) was used to derive basic descriptive data for the Likert-type scale questions.
Results
Of the 1441 surveys mailed, 501 (35%) were returned and 376 (26%) were eligible for analyses. The other 125 respondents returned blank surveys or noted they were not PCPs. The characteristics of the final sample are shown in Table 1, and the similarity of our sample to available state and national comparison data are reflected in Table 2. The eligible sample included approximately 80% of all practicing PCPs in Illinois, which is based on ICAAP membership statistics of practicing pediatricians in Illinois.29,30 Our sample had a higher proportion of Title V medical home certified providers (14%) than Illinois pediatricians as a whole (4%).
Sample Characteristics
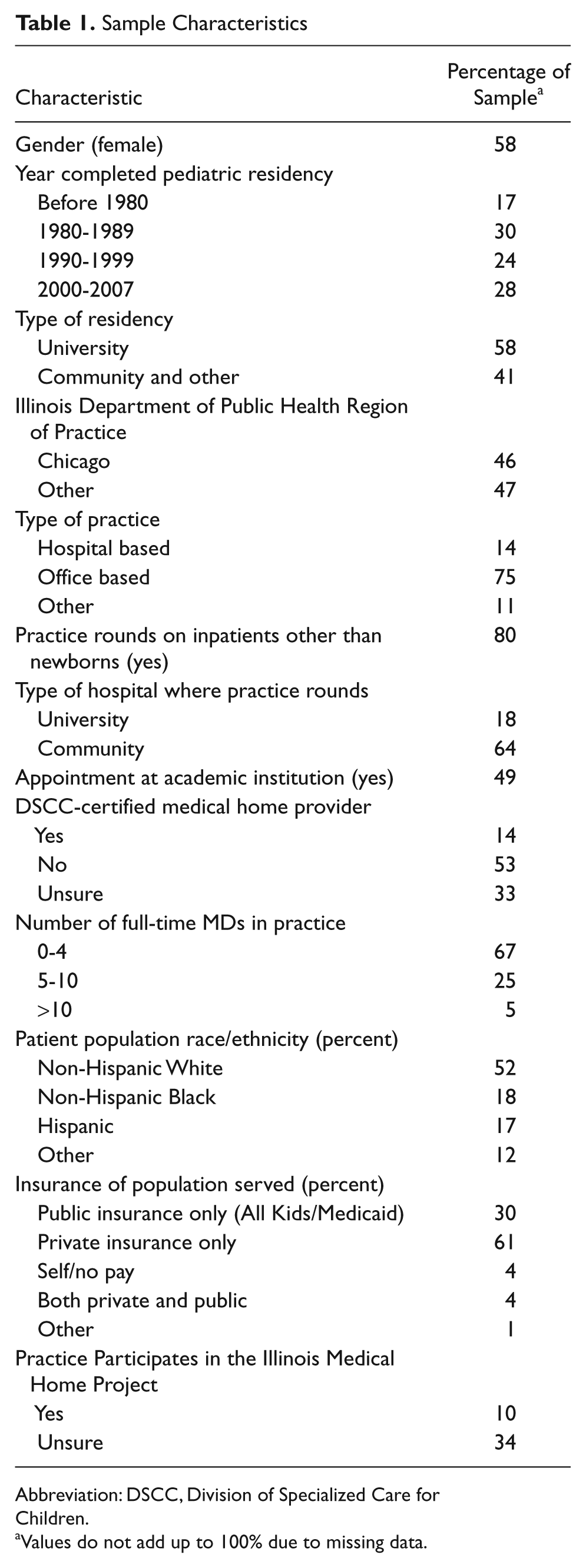
Abbreviation: DSCC, Division of Specialized Care for Children.
Values do not add up to 100% due to missing data.
Sample Characteristics and State and National Data
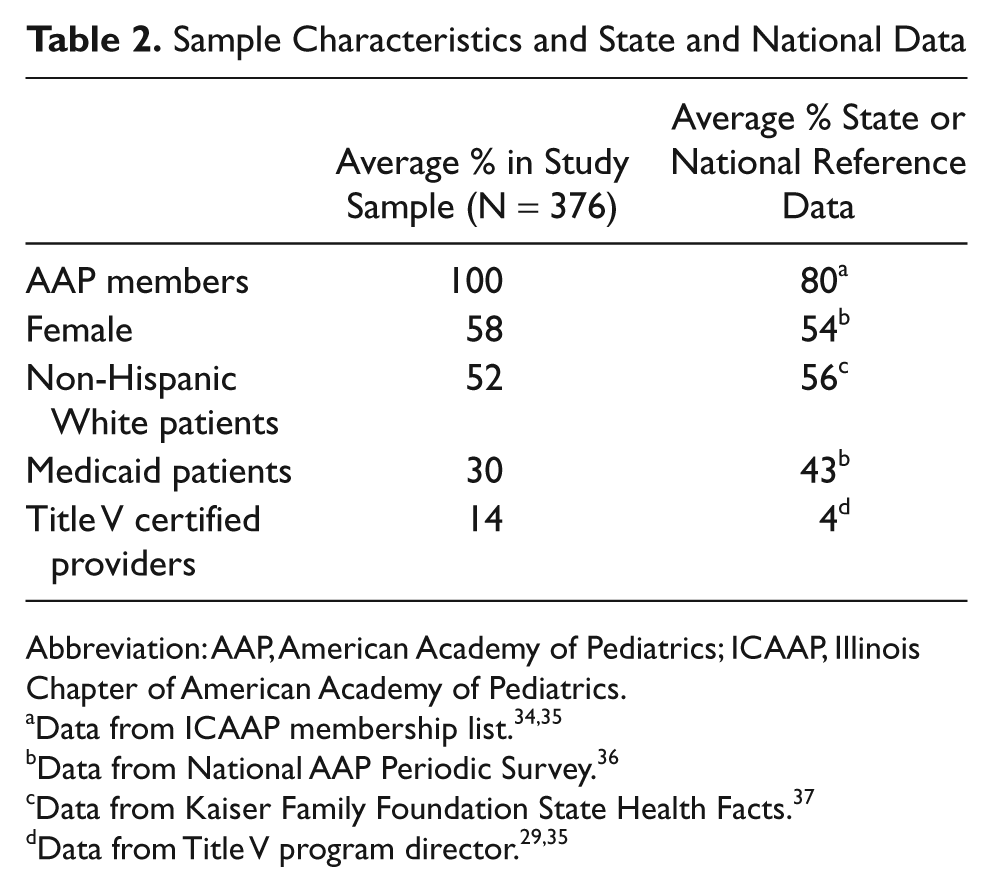
Abbreviation: AAP, American Academy of Pediatrics; ICAAP, Illinois Chapter of American Academy of Pediatrics.
Data from National AAP Periodic Survey. 36
Data from Kaiser Family Foundation State Health Facts. 37
Table 3 presents the percentage of respondents who perceived stated barriers “somewhat or very significant.” The top 5 barriers were insufficient time to care for patients’ needs (72%), insufficient reimbursement for time (68%), lack of support services such as case management and social work (59%), lack of knowledge about services available (55%), and lack of understanding of coding/billing (53%). “Insufficient interest in CYSHCN” was the least frequently chosen barrier (19%).
PCP Perception of Barriers to Providing Effective Primary Care to CYSHCN a
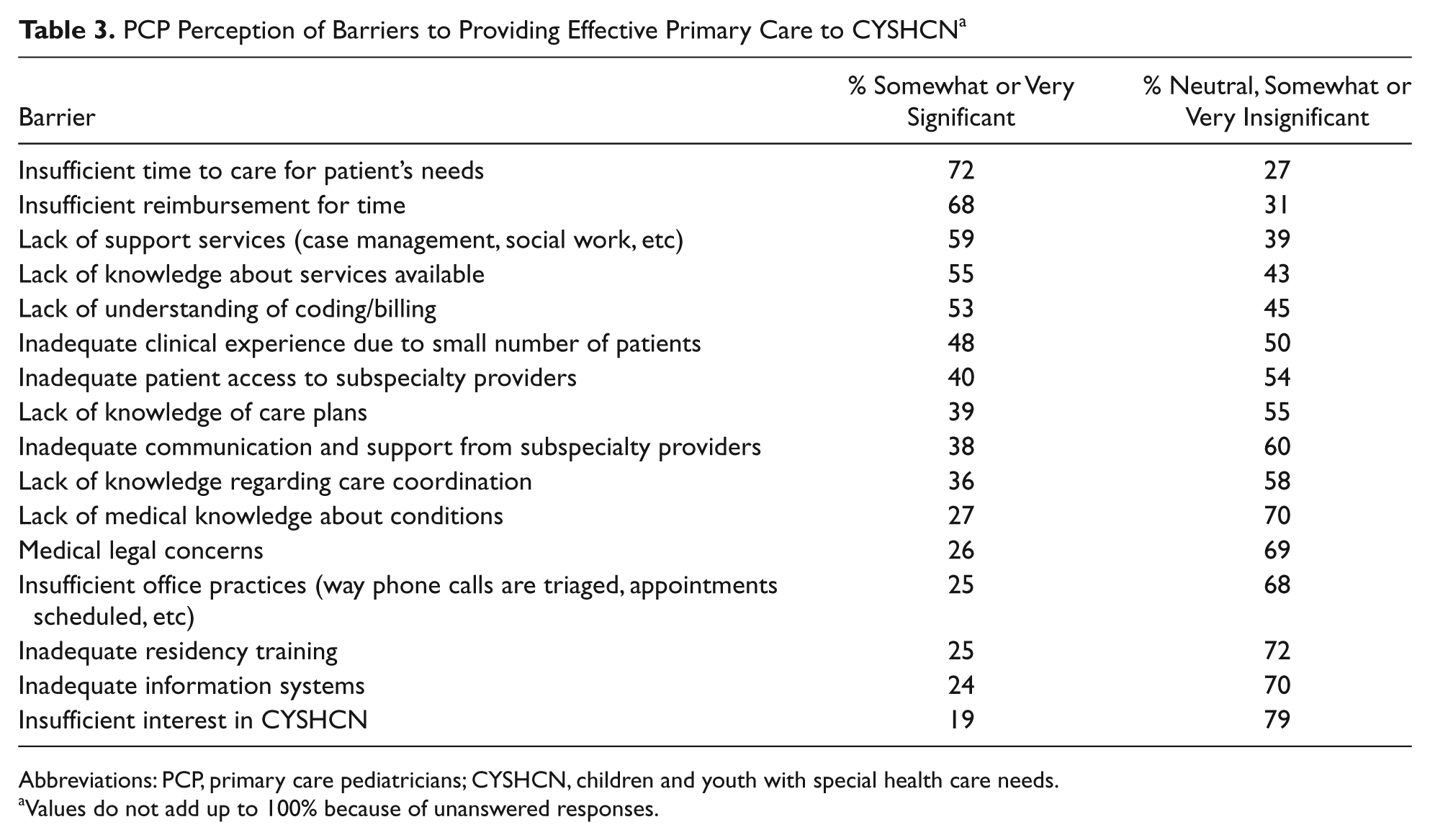
Abbreviations: PCP, primary care pediatricians; CYSHCN, children and youth with special health care needs.
Values do not add up to 100% because of unanswered responses.
The percentage of respondents who felt somewhat or very prepared to perform various tasks related to caring for CYSHCN is presented in Table 4. PCPs felt most prepared to access early intervention services (89%), prescribe physical/occupational/speech therapies (80%), and coordinate care among subspecialists (78%). They felt least prepared to adequately bill and code for their services (24%).
PCP Preparedness to Performing the Following Tasks for CYSHCN a
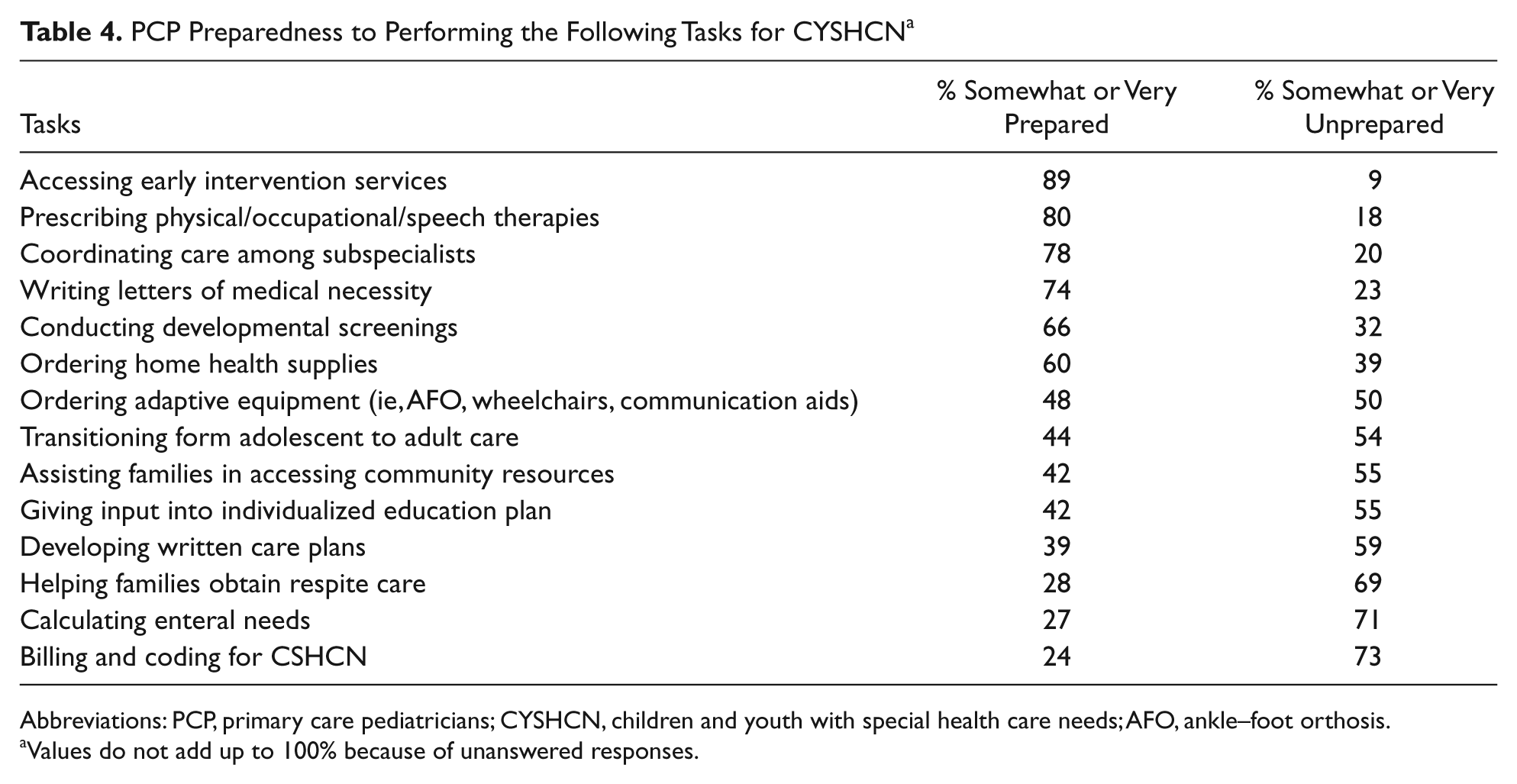
Abbreviations: PCP, primary care pediatricians; CYSHCN, children and youth with special health care needs; AFO, ankle–foot orthosis.
Values do not add up to 100% because of unanswered responses.
Table 5 presents the percentage of respondents who were somewhat or very comfortable providing primary care to children dependent on various technologies. PCPs felt most comfortable providing primary care to children requiring blood glucose monitoring (75%), home apnea monitoring (72%), and feeding tubes (68%) and least comfortable providing care to children requiring dialysis (12%).
PCP Comfort Level Providing Effective Primary Care to CYSHCN Dependent on the Technologies Listed Below
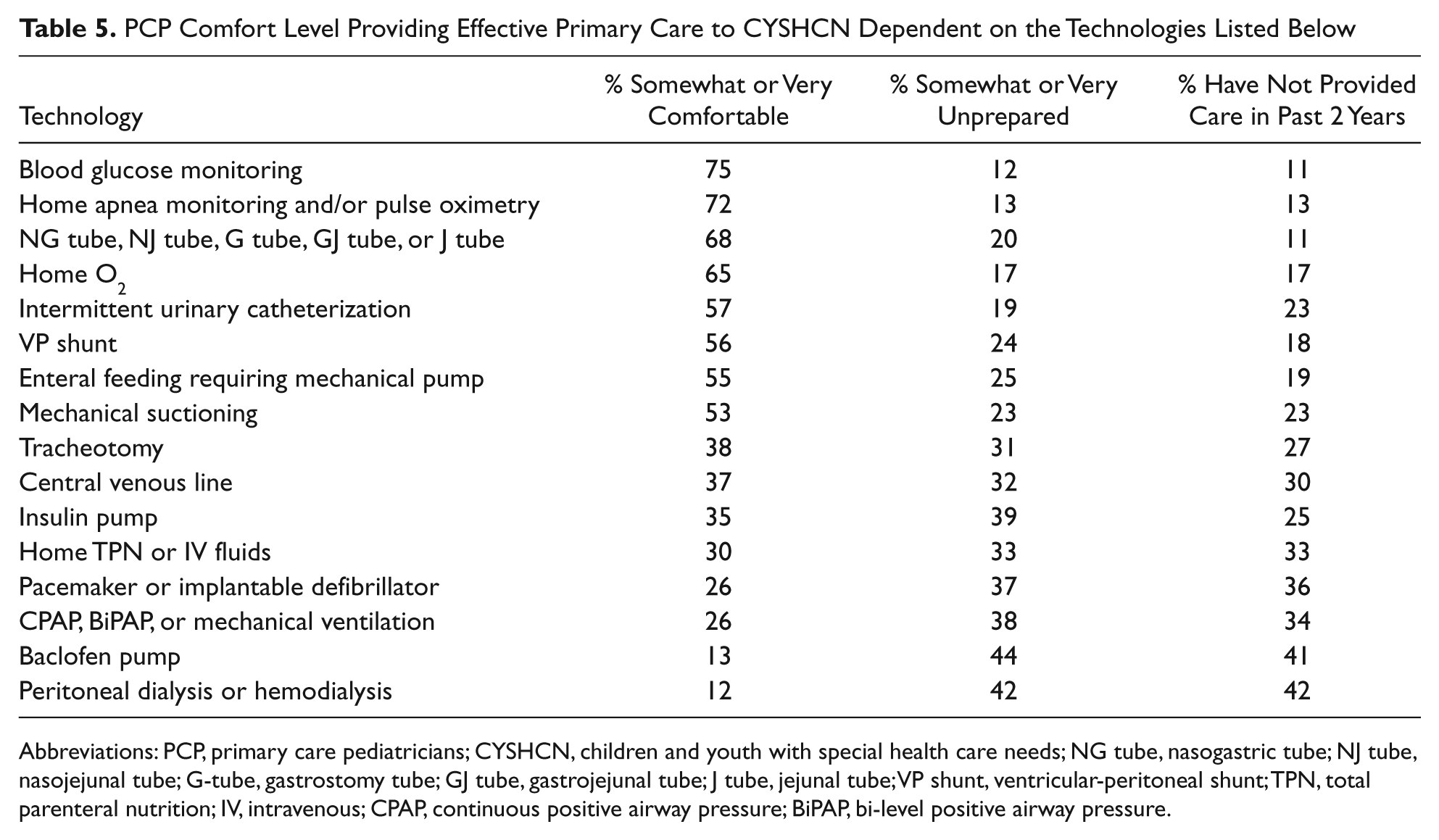
Abbreviations: PCP, primary care pediatricians; CYSHCN, children and youth with special health care needs; NG tube, nasogastric tube; NJ tube, nasojejunal tube; G-tube, gastrostomy tube; GJ tube, gastrojejunal tube; J tube, jejunal tube; VP shunt, ventricular-peritoneal shunt; TPN, total parenteral nutrition; IV, intravenous; CPAP, continuous positive airway pressure; BiPAP, bi-level positive airway pressure.
Discussion
This exploratory survey of Illinois PCPs’ perceptions has several findings that warrant further exploration and research. The finding that survey respondents do not cite lack of interest in CYSHCN as a barrier suggests that systemic factors are perceived as much more salient than individual preferences. For example, insufficient reimbursement and time were recurring themes in survey responses. Providers ranked these as the most important barriers, and they reported billing and coding to be the task with which they felt the least comfort. This is not surprising given the lack of reimbursement for non-face-to-face time and prior literature showing that placement of care coordinators in practices has been shown to decrease ER utilization and costs to payers, but to increase costs to practices.21-23,31-33 Education around billing and coding has been undertaken by the AAP to help improve reimbursement on a practice level. 34 Our data suggest that these efforts are critical as PCPs report struggling with reimbursement.
The findings that PCPs do not rate inadequate insufficient office practices and inadequate information systems as significant barriers contrasts with evidence that enhancement in these areas improve efficiency. A variety of medical home demonstration projects have successfully demonstrated improvements with modification of office practices such as phone triaging and appointment scheduling21,31,35; however, many Illinois PCPs appear not to perceive a problem with their current practices, suggesting limitations in getting buy-in for medical home quality improvement initiatives among PCPs. Similarly, few PCPs cite inadequate information systems as a barrier despite the current focus on electronic health record adoption funded by the American Recovery and Reinvestment Act. Attempts to make PCPs meaningful users of such systems may be limited by perceptions that they are not necessary.
Generally, Illinois PCPs perceive little difficulty navigating the medical and therapy system. Most feel prepared to access early intervention, prescribe therapies, order home health supplies, and coordinate care among subspecialists, and less than half cite access or communication with subspecialists as a barrier. Almost half of the PCPs feel prepared to order adaptive equipment. In contrast, respondents cite interfaces outside of the medical system as more challenging. Lack of support services and knowledge of available services were rated highly as barriers and assisting families’ access to community resources, giving input into an individualized education plan and helping families obtain respite care were cited as tasks for which respondents felt relatively unprepared. Given the importance of school and community services for CYSHCN, PCPs may require enhanced education on navigating such systems.
While only one quarter of respondents cited inadequate residency training as a barrier, nearly twice as many cited inadequate clinical experience due to small numbers of patients. This is corroborated by the data on PCPs’ comfort levels providing primary care to children dependent on a variety of medical technologies. The findings that most PCPs state they feel unprepared to provide primary care to (or have not seen such a patient in the past 2 years) children with tracheostomies, central lines, home ventilation, and other invasive technologies suggests that our existing primary care system may have limitations in providing care to CYSHCN with the most complexity. Indeed, a variety of tertiary care center-based programs have been developed to serve as bridges between tertiary care centers and community PCPs with positive outcomes.21,31,36,37 In the aftermath of health care reform and the possible implementation of accountable care organizations looming, it will be important for policy makers to consider potential novel systems of care for children with medical complexity who challenge our systems of care.
Study Limitations
This study is exploratory and has several limitations. The sample was derived from 1 state and responses may not be generalizable to different parts of the country. The response rate was 26%, similar to that in other studies that attempt to catch a large population of providers38,39; however, we did not have comparison data for nonresponders. While the racial mix of responders’ patients was similar to the state as a whole and the gender mix of responders was similar to pediatricians nationally, the payer mix of responder practices included more private insurance than national averages. Dues-paying AAP members and Title V program participants are oversampled; however, this may suggest that the perception of barriers among all Illinois PCPs may be underestimated by our sample. The study is subjective in nature, relies on PCP perceptions, and there was no formal validation process for the survey. Finally, the data rely on self-report of key variables such as payer mix, number of CYSHCN, and so on and thus are subject to recall bias.
Implications
This study raises questions about the optimal method to ensure that CYSHCN have access to primary care that meets their needs. While health care reform proposals to improve reimbursement for care coordination are encouraging, it is important to make sure that such reimbursement adequately pays for services that are known to improve care for CYSHCN and whose insufficiency impedes physicians from caring for CYSHCN. Strategies to help PCPs access community resources for their patients should be explored. Medical home quality improvement initiatives and electronic health record implementation efforts will need to overcome many PCPs’ perceptions that information systems and office practices are not barriers to caring for CYSHCN. Given the high degree of PCP discomfort with children dependent on certain medical technologies, targeted educational initiatives and the development and study of novel clinical models to care for children with complex, chronic conditions and technology dependence should be encouraged.
Footnotes
Acknowledgements
We would like to thank Jim Harisiades and the Children’s Memorial Office of Child Advocacy for generous funding support; the Illinois chapter of the American Academy of Pediatrics for logistical and clerical support in survey administration; Paul Wise, MD, Eyal Cohen, MD, and Joel Frader, MD, for their review of this article.
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article:This project was funded by a grant by the Children’s Memorial Hospital Office of Child Advocacy.