
Abstract

Introduction
Enteric fever is a very common childhood infection in tropical countries. Hematological derangements are common in enteric fever and include anemia, leukopenia, thrombocytopenia, and subclinical disseminated intravascular coagulation. 1 Although these changes are transient and respond favorably to the appropriate antimicrobial therapy, they can lead to potentially life threatening complications, as with our case who presented with intracranial hemorrhage.
Case Report
A 9-year-old boy presented with high-grade continuous fever of 10-days duration, generalized purpuric rash with oronasal mucosal bleeding for 3 to 4 days, and alteration of sensorium along with weakness of right side of the body since 2 days. The child initially had abnormal behavior with incoherent speech, which rapidly progressed to altered sensorium and a nonresponsive state. There was no history of headache, vomiting, seizures, jaundice, or similar illness in the past.
On examination, he was toxic looking, febrile, and tachypneic. His blood pressure was normal. He had severe pallor and a generalized petechial rash along with mucosal bleeding from oral and nasal cavities. There was no significant lymphadenopathy or icterus. Abdominal examination revealed splenomegaly (3 cm below costal margin) and hepatomegaly (4 cm below costal margin with a span of 14 cm). Skull examination revealed absence of any bruit. He was drowsy with incoherent speech, right-sided hypertonia, and hyperreflexia. There were no cranial nerve palsies, cerebellar signs, or signs of meningeal irritation. The pupils were bilaterally dilated with preserved reaction to light. Fundus examination revealed papilledema.
Laboratory examination revealed a hemoglobin of 5 g%, total leukocyte count of 3500/mm3, and platelet count of 3000/mm3. Liver and renal function tests along with electrolytes were normal.
There was prolongation of prothrombin time with international normalized ratio of 1.6.
Noncontrast computed tomographic scan of the brain revealed intraparenchymal hemorrhage in left frontal, parietal, and temporal lobes with marked perileisonal edema (Figure 1). Subsequently, magnetic resonance angiography was done to rule out any intracranial vascular malformation.
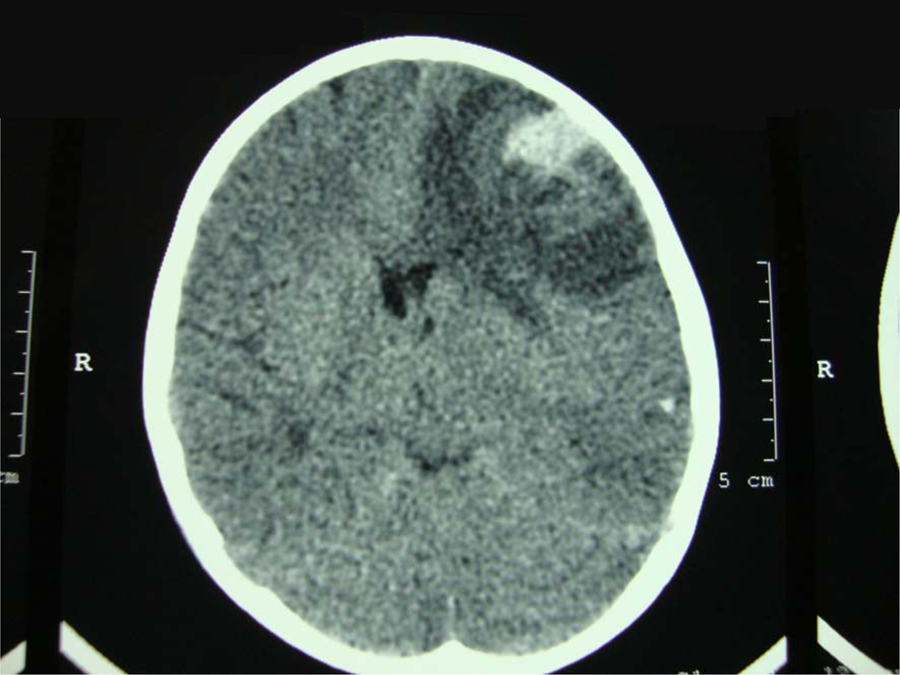
Intraparenchymal hemorrhage in left frontal lobe.
The patient was given blood, fresh frozen plasma and platelet transfusions, intravenous ceftriaxone, and injection vitamin K along with supportive management. The patient responded well clinically and became afebrile after 5 days. His total leukocyte and platelet counts progressively increased to 7600/mm3 and 80 000/mm3, respectively after 10 days of starting ceftriaxone. His neurological condition improved, and he regained full consciousness and speech. He started interacting and accepting orally during the course of admission. The intravenous antibiotic therapy was continued for 14 days. At the time of discharge, the patient was conscious and oriented with improving right hemiparesis. The blood counts and prothrombin time had normalized.
One month after discharge, the patient had recovered completely with resolution of intracranial bleed on repeat computed tomographic scan and no deficits on neurological examination.
Discussion
Neurological manifestations in enteric fever occur with a varying incidence of 5% to 35% and include delirium, aphasia, seizures, meningitis, encephalomyelitis, transverse myelitis with paraplegia, peripheral and cranial neuritis, optic neuritis, Guillain–Barré syndrome, psychotic syndromes, and hemiplegia. 2
Intracranial hemorrhage (ICH) as a manifestation of enteric fever is very rare. To the best of our knowledge, only 2 cases of enteric fever presenting with ICH have been reported in the literature.3,4
Anemia, leukopenia, thrombocytopenia, and coagulation abnormalities such as elevated prothrombin time, partial thromboplastin time, elevated fibrin degradation products, including
Bhatnagar et al 5 in their retrospective study of 109 children presenting with pancytopenia observed enteric fever as the underlying etiology in 30% of the cases. Prevalence of thrombocytopenia in enteric fever is about 10% to 15% 6 and is considered a marker of severe disease. 7 Malik and Malik 8 in their prospective study involving 102 children suffering from enteric fever inferred that the presence of thrombocytopenia increases the risk of developing complications, observed in 60% of the patients with thrombocytopenia. Approximately 10% patients with thrombocytopenia experience a hemorrhage. 9
Any condition causing severe thrombocytopenia (platelet count <20 000/mm3) predisposes a patient to bleeding disorder, including ICH. 10 Although ICH is unusual if the platelet count is more than 20 000/mm3, presence of associated subclinical coagulopathy can increase the predisposition to bleeding. 11
The hematological changes associated with enteric fever are thought to be secondary to bone marrow suppression and hemophagocytosis stimulated by Salmonella endotoxin. 9 Other probable mechanisms of thrombocytopenia in enteric fever include reduced production, immune mediated destruction, and platelet phagocytosis mediated by increased macrophage-colony stimulating factor. 12
Our case presented with ICH secondary to associated thrombocytopenia and partial coagulopathy. This case report highlights that although the hematological derangements associated with enteric fever are usually self-limited, they could lead to a potentially serious hemorrhage warranting appropriate replacement of blood, platelets, and clotting factors along with specific antimicrobial treatment.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.