
Abstract
Background. Food insecurity (FI) is common, but studies in families with infants are rare. Objectives. To determine prevalence of FI, assess the effect public benefits have on FI, assess strategies to stretch nutritional resources (eg, using generic formula), and investigate FI’s relationship to anthropometric measurements. Methods. A cross-sectional survey was completed. FI was classified using the US Department of Agriculture’s 6-item indicator set. Results. A convenience sample of 144 infant caregivers was surveyed. Thirty-one percent endorsed FI. FI was more common among those receiving WIC and SNAP (39% vs 22%; P < .05). Fifteen percent stretched infant formula (27% FI vs 9% food secure; P < .01), 58% would not use generic formula, and 50% believed that generic and brand name formulas were not equivalent. There was no significant association between FI and anthropometric measurements. Conclusions. FI and formula stretching were common, even among families receiving public benefits. Many families were cautious about using generic formula.
Background
Food insecurity (FI) is defined as “the lack of access to enough food to fully meet basic nutritional needs at all times due to lack of resources.”1-5 National data suggests that 16% to 22% of American households with children experience FI. 6 Infants are especially vulnerable to the negative effects of insufficient nutrition, which can result in negative psychological, behavioral, and cognitive outcomes. 7 Although no consistent associations have been found between household FI and abnormalities in anthropometric measurements, children who live in households that experience FI are at risk for micronutrient deficiencies. 8 Such deficiencies can contribute to anemia, developmental delay, increased hospitalizations and acute illnesses, and poor health outcomes.3-5,7,9-11 There is limited published information on the status of infants less than 12 months living in food-insecure households.
Families experiencing hunger often also experience other social and financial strains, forcing many to make difficult decisions between nutrition and other essential needs.7,12-14 The majority of low-income families receiving care at urban pediatric clinics report at least 1 unmet basic need (eg, food, housing, or employment), with many reporting more than 1 unmet need. 12 Recent data suggest that pediatricians should educate families on the importance of proper nutrition and screen, assess, and make appropriate referrals based on families’ social needs, particularly food insecurity.4,12,15-18
Rates of household FI at the end of 2009 were the highest since they were first measured in 1995 by the first national food security survey. 19 Food-insecure households rely on supplemental public and community-based programs such as the Supplemental Nutrition Assistance Program (SNAP); Special Supplement Nutrition Program for Women, Infants, and Children (WIC); school lunches; food banks; community organizations; and support from friends and family. SNAP, formerly known as the federal Food Stamp Program, provides resources to low-income families to assist with purchasing of food. WIC is the largest food supplement program in the country, serving 45% of low-income children born in the United States.3,20,21 In October 2009, WIC decreased the amount of formula provided to those infants over 6 months of age as part of a new food provision guideline, highlighting the supplemental nature of this program. 21
When parents or guardians are unable to purchase additional nutrition for their infant, some turn to potentially harmful strategies to stretch the formula they have. Such strategies include rationing or dilution of formula, use of water or juice as formula substitutes, feeding extra solid foods, or giving cow’s milk before 12 months of age, all of which can place infants at nutritional risk. 8 One potential strategy for decreasing the cost of additional infant formula by up to 40% is the use of generic formulas instead of brand name formula. 22 The US Food and Drug Administration (FDA) tightly regulates infant formula, so generic varieties are nutritionally equivalent. 23 To our knowledge, the use of generically branded formula has not been explored in the literature.
Given the underrepresentation of infants in previous studies on FI, little is known about the extent and characteristics of household FI experienced by infants who receive pediatric care in urban centers. This study therefore aimed to (1) examine the prevalence of household FI and participation in supplemental food programs in families with infants in 2 urban primary care centers; (2) determine if supplemental program participation was protective against FI; (3) describe strategies families implement to stretch their nutritional resources, including the use of generic formula; and (4) determine if there was a relationship between food insecurity and anthropometric measurements.
Methods
Study Design and Data Collection
A cross-sectional study was performed to assess household FI among infants receiving primary care at 2 urban health centers. The Pediatric Primary Care Center (PPCC) is a hospital-based, academic, urban outpatient primary care center and is the medical home for approximately 15 000 patients (35 000 visits annually). The Hopple Street Health Center (HSHC) is a community-based, urban outpatient pediatric primary care facility with nearly 10 000 visits per year.
A convenience sample of English-speaking caregivers of infants aged 0 to 12 months presenting for primary care visits completed a self-administered survey. Between March and April 2010, caregivers were approached by study personnel while waiting for their health care provider. Participation in the study was voluntary, anonymous, and caregivers were not compensated. The study was approved by the institutional review board at Cincinnati Children’s Hospital Medical Center.
Study Measures
Participants completed a self-administered 37-question survey. The survey first assessed key family sociodemographic characteristics including patient age, race, parental age and education, ethnicity, and source of insurance. Our primary outcome measure, household FI, was defined using the US Department of Agriculture’s (USDA) validated 6-item indicator set for classifying household food security. The USDA defines food security as having no problems or limitations with food access. FI is divided into 2 categories: food insecure with and without hunger. FI with hunger requires a disruption of eating patterns, as well as reduced food intake. 2 FI without hunger is a reduction of food quality, variety, and desirability, without reduced food intake. The items in the 6-item indicator set include an assessment of whether families did not have enough money for food, bought food that did not last, lacked resources to afford to eat balanced meals, skipped meals, ate less than they should, or felt hungry. 2 The survey also assessed participation in supplemental food programs and strategies for stretching limited food resources for infants (eg, diluting formula, substituting solid foods, buying generic formula). The questions were developed after consultation with on-site registered dieticians, social workers, and legal advocates. Anthropomorphic measurements were collected via a review of the electronic medical record and added to the data from completed surveys.
Analysis
Descriptive statistics were used to report baseline sample characteristics as well as prevalence of household FI, strategies used to stretch nutrition, participation in supplemental food programs, and attitudes toward generic brand formula. Food-insecure households (hungry and not hungry) were combined to assess bivariate associations between household food insecurity and (a) participation in supplemental food programs, (b) strategies used to stretch formula, and (c) attitudes toward generic brand formula using χ2 statistics. Associations between participation in supplemental food programs and strategies used to stretch nutritional resources were assessed. Relationships between household FI and anthropometric measurements were assessed using the t test. All analyses were performed using SAS statistical software (version 9.2; Sas Inc, Cary, NC).
Results
There were 144 infants in our sample. Demographic characteristics of the sample population are described in Table 1 and are similar to the demographics of families seen in the primary care centers. Of caregivers, 79% had a least a high school or general educational development (GED) certificate. Sixty-five percent of families receiving infant formula from WIC report running out each month.
Patient Demographics of Surveyed PPCC/HSHC Families (N = 144)
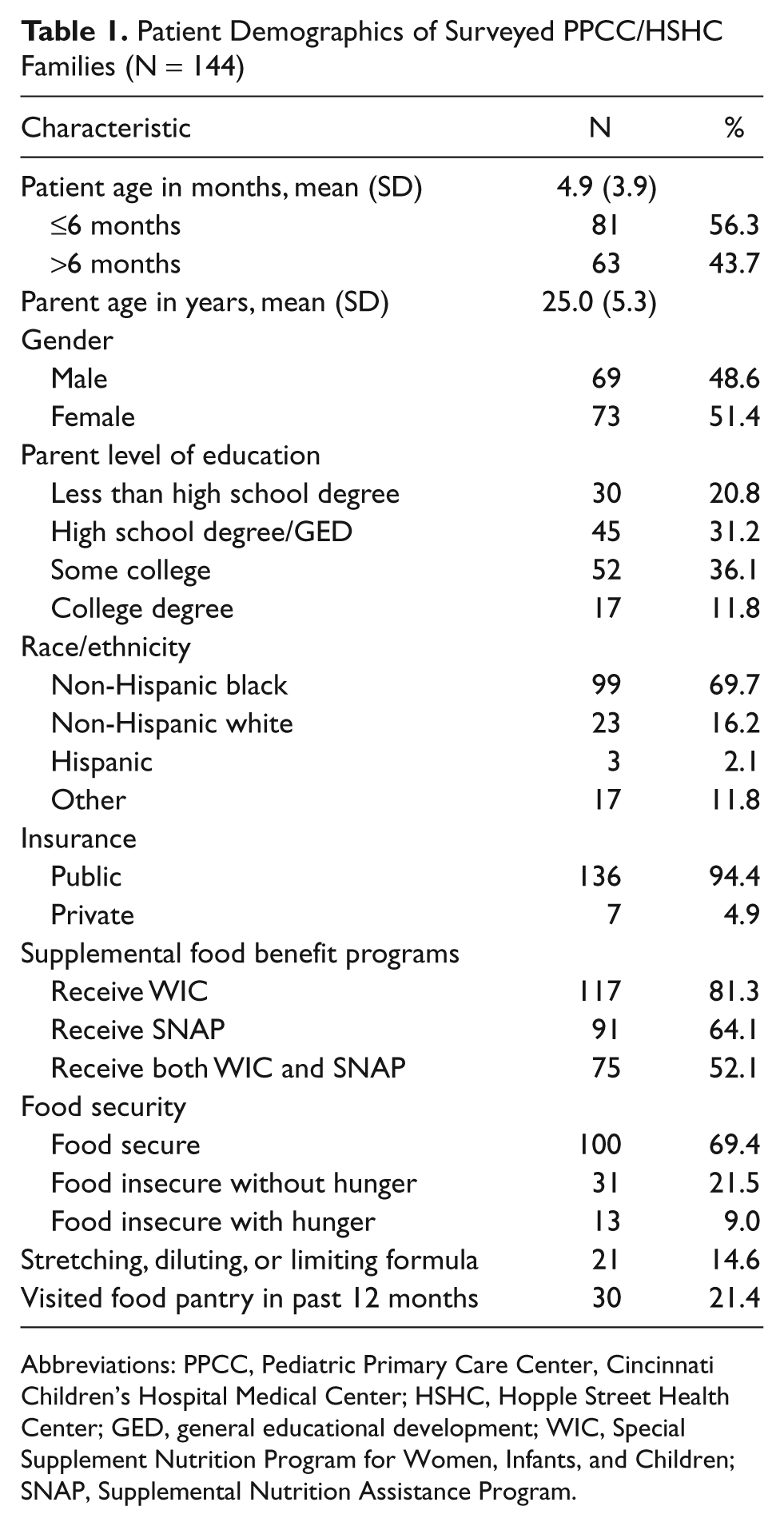
Abbreviations: PPCC, Pediatric Primary Care Center, Cincinnati Children’s Hospital Medical Center; HSHC, Hopple Street Health Center; GED, general educational development; WIC, Special Supplement Nutrition Program for Women, Infants, and Children; SNAP, Supplemental Nutrition Assistance Program.
Using the USDA 6-item indicator set for classifying household food security, 2 we found that 9% of families were classified as food insecure and hungry and 22% were food insecure but not hungry. There was no significant difference in food security status between infants less than 6 months and those 6 months to 12 months of age (P = .3).
Associations between presence of FI and patients participating in supplemental public assistance programs are illustrated in Table 2. Patients receiving SNAP still had greater than 3-fold increased risk of living in a food-insecure household when compared with those not receiving SNAP (P < .01). Also, families enrolled in both WIC and SNAP were more likely to be food insecure than those not enrolled in both programs (39% vs 22%, P < .05). Households that used a food bank in the previous 12 months were more likely to be food insecure (43% vs 24%, P = .07).
Bivariate Relationships Between Supplemental Food Assistance and Household Food Insecurity a
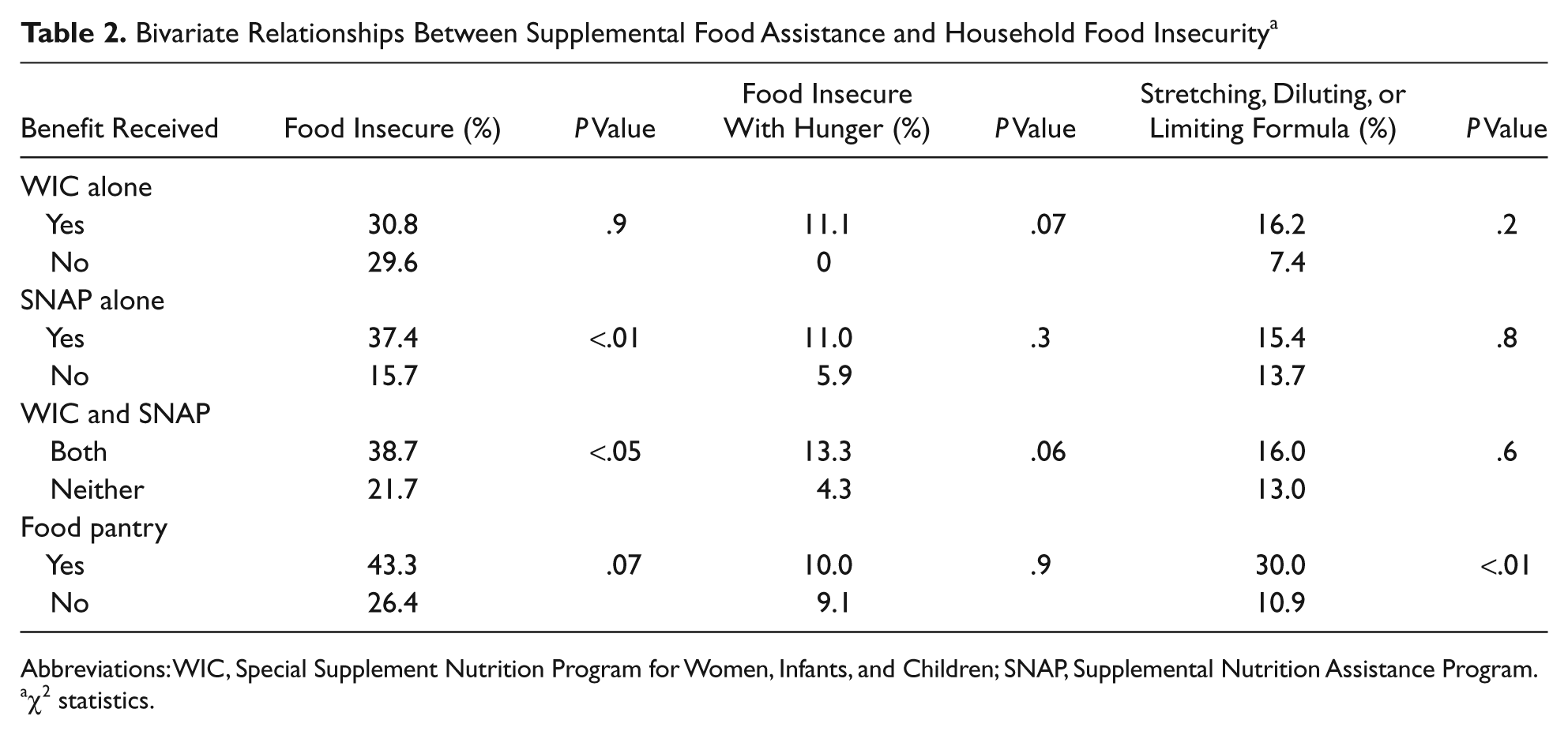
Abbreviations: WIC, Special Supplement Nutrition Program for Women, Infants, and Children; SNAP, Supplemental Nutrition Assistance Program.
χ2 statistics.
Families reported multiple strategies to avoid hunger for infants: 15% reported stretching formula through dilution, by feeding smaller volumes, or increasing time intervals between feeds. Stretching, diluting, or limiting formula was reported in 27% of food-insecure families compared with 9% of food-secure families (P < .01).
Families’ opinions about generic formula usage are depicted in Figure 1. Only 24% said they would buy generic infant formula, and 58% reported that they would not use generic infant formula even if it were provided free. Fifty percent of caregivers believed that generic and brand name formula did not have equal nutritional value. Food security status was not associated with attitudes toward generic formula (P = .5), nor was level of caregiver education.
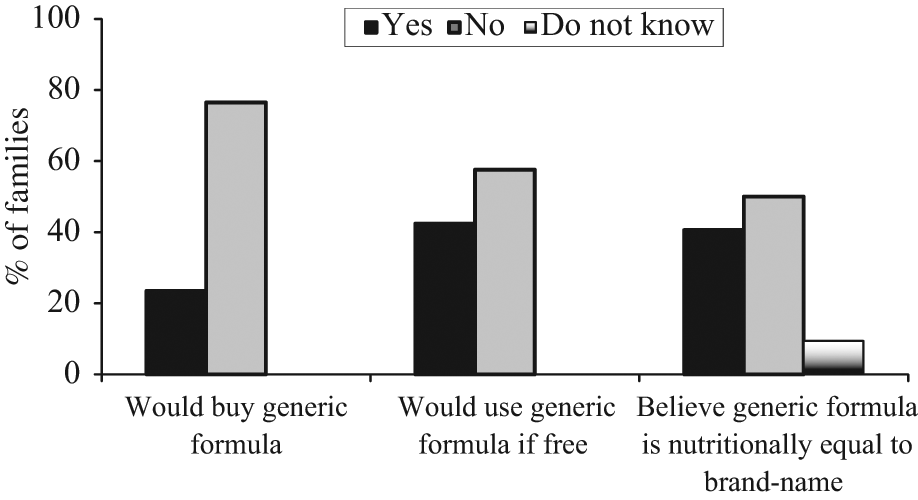
Attitudes toward generic formula
Finally, anthropomorphic measures including weight, height, and head circumference in infants from food-insecure (both hungry and not hungry) households were not significantly different from those infants in food-secure households (all P > .5).
Discussion
Nearly one third of families in this sample reported household FI, a rate higher than the national average, but not uncommon for urban populations. Since infants are subject to their family’s circumstances, these results imply that infants living in these strained households are at high risk for FI and its associated complications. We believe that screening and intervening early in infancy has the potential to alter the nutritional trajectory for children. Given the associations between FI and adverse health outcomes, assessing for FI early may have a profound and lasting effect.5,6,10
Despite having a majority of the PPCC and HSHC population receiving supplemental food benefits such as WIC and SNAP, many remain at high risk for experiencing FI. Indeed, nearly 40% of those receiving both WIC and SNAP live in food-insecure households. While public assistance programs such as WIC and SNAP are critical to many families, it remains unclear how many clinicians and families know that these programs are supplemental and not meant to support the entire nutritional needs of children. In this sample, 65% of families run out of WIC-supplied infant formula most months, so it is not surprising that many of these families fit criteria for FI, despite their participation in WIC. Though WIC decreases the amount of formula given to infants after age 6 months, results did not show significant differences in FI between the 2 groups. While these programs are supplemental, they clearly reach families in great need.
Approximately 1 in 6 families reported stretching, diluting, or limiting infant nutrition to make it last. Although the literature has shown that formula preparation is not done accurately by a portion of the general population, regardless of education level, 24 intentional dilution to stretch inadequate resources is a significant but often underrecognized issue. Potential impediments to identification of stretching, diluting, or limiting of infant nutrition include the lack of direct correlation with anthropometric measurements, provider discomfort, and hesitance by the parents to report this strategy as they struggle to meet their children’s basic needs. 16
Only 24% of caregivers in this study would buy generic infant formula, and 50% believed that generic and brand name formulas were not nutritionally equivalent. There was not a significant association between attitudes toward generic formula and FI. This distrust of generic products is unfortunate since generic formula offers families a nutritionally acceptable option to decrease out-of-pocket expense for infant formula. The literature has not, to our knowledge, explored beliefs surrounding generic formula. One could hypothesize that since many families receive WIC, which provides brand name formula, these families continue to buy the brand name products that they are familiar with. If caregivers do not know that generic formulas are nutritionally equivalent and regulated by the FDA, they may feel compelled to buy the option perceived to be most nutritious, despite the increased cost.
There was no significant correlation between household FI and anthropometric measurements. The lack of such an association is consistent with prior literature. Previous studies focusing on infant and child nutrition consistently showed that hunger cannot be identified by using such objective measures.11,25 Others have suggested that children aged 0 to 5 years enrolled in WIC are more likely to suffer from overweight or obesity than failure to thrive. 26 These findings suggest that focusing on infants with delayed growth may miss a sizable number of vulnerable infants that fall within normal or overweight growth distributions. Though FI is often a physically invisible problem among young children, the long-term health implications are pronounced.
This study has several limitations. The cross-sectional nature of this study limits the ability to assess changes over time. Though this was a convenience sample, the demographic makeup of this population is similar to that of PPCC and HSHC, suggesting that the surveyed sample was representative of the overall population seen at these 2 primary care sites. The findings of FI and stretching formula may be subject to social desirability bias, with potential for underreporting of FI and formula stretching. Finally, this study only included families from 2 urban primary care centers and excluded families without English proficiency, thus these findings may not be generalizable to infant populations in other regions or with different demographic characteristics.
Future studies should assess the barriers to feeding generic infant formula, as well as practical strategies for families to use when food resources are limited. Education of health providers to accurately screen for FI during routine well child care is another area that should be further explored. Developing interventions, in collaboration with community agencies, for families experiencing household FI is critical.
Conclusions
Household FI among families with infants is common among this patient population. Families receiving WIC and SNAP remained at high risk for FI despite receiving these supplemental benefits. Food-insecure families were more likely to dilute or stretch infant formula. Despite its lower cost, many families remain cautious about using generic formula regardless of food security status or level of education. FI did not correlate to anthropometric measurements.
Footnotes
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The authors received no financial support for the research, authorship, and/or publication of this article.