
Abstract

Case Presentation
A 5-year-old boy presented to the emergency room (ER) with pain in the left posterior knee and calf for 4 days. The pain was limiting his mobility, and he walked with a limp on day 1 following onset of symptoms. His leg pain resolved overnight, but on day 2, he began having pain in the right knee and ankle with associated edema. Around the same time, he developed right unilateral periorbital edema. This also resolved without treatment; however, he developed periorbital edema and rash over the contralateral eye on day 3 of symptom onset. Associated symptoms at presentation included transient abdominal pain and fever with an upper range of 102°F. The abdominal pain varied in intensity, and the patient had 2 episodes of nonbilious, nonbloody, vomiting without diarrhea or constipation. He had been seen at an outside ER and was sent home on ibuprofen without a diagnosis. His mother denied any new rashes, changes in bowel habits or urine output, recent illness, or any other complaints.
Physical exam in our ER revealed an uncomfortable boy with normal vital signs. Pertinent physical findings included moderate periorbital edema with an ecchymotic rash over the right eyelid. There was mild diffuse tenderness to palpation over the abdomen and mild left knee edema with tenderness to palpation. Of note, the patient refused to ambulate secondary to pain. Dermatological exam showed multiple insect bites on the lower extremities bilaterally without any rash other than over the eye.
A number of laboratory tests were ordered in the ER. Initial complete metabolic panel and complete blood count were normal. Urinalysis revealed trace protein, positive ketones, positive urobilinogen, and trace mucous. Chest X-ray, KUB (kidneys, ureters, bladder), and left leg radiograph were all normal. At this point, the ER physician ordered numerous laboratory tests, including a comprehensive metabolic panel, lyme antibody, C3, C4, CH50, rheumatoid factor, lactate dehydrogenase, ANA (antinuclear antibody) panel, lupus panel, scleroderma panel, and ASO (antistreptolysin O) titer. He was given ibuprofen and admitted to the pediatric floor.
The patient was treated with scheduled ibuprofen monitored overnight without complications. The following morning, his periorbital edema had decreased significantly. Throughout the day, his pain improved to the point where he ambulated without restriction. Initial labs demonstrated an increased ASO titer, and the patient was treated with the appropriate course of penicillin. He was discharged on hospital day 1 with complete resolution of physical signs and symptoms.
Discussion
Henoch–Schönlein purpura (HSP) is a common pediatric ailment that can present with a wide variety of complaints. HSP is an autoimmune disease resulting from nonthrombocytopenic IgA-mediated vasculitis. Known triggers of HSP episodes include infection, vaccinations, and insect bites, though often there is no identifiable inciting source.1,2 Patients can present with a wide range of signs and symptoms, with every organ system potentially affected by the disease. Clinical manifestations can occur over the course of days to weeks and vary in the order of symptom presentation. Although HSP itself is typically benign, serious and life-threatening complications can occur.1,2 This case and review of the literature highlights the difficulty in diagnosing HSP and explores the etiology, diagnosis, inpatient criteria, and treatment modalities for pediatricians caring for patients with the disease.
In the above case, a 5-year-old boy presented with an unusual set of symptoms: migratory polyarthritis, fever, abdominal pain, and periorbital edema. At this point, a wide range of diseases should be considered, including infectious, autoimmune, rheumatologic, and malignant etiologies. Migratory polyarthritis is a relatively uncommon complaint caused by only a handful of childhood diseases. Lyme disease, poststreptococcal arthritis, juvenile idiopathic arthritis, HSP, and reactive arthritis are common etiologies of pediatric migratory polyarthritis. Lyme disease is not endemic to Louisiana, and the time course of hourly migration of pain did not correlate with Lyme disease, which has more prolonged relapsing arthralgic episodes. 3 The patient did not have conjunctivitis or respiratory complaints and no recent history of upper respiratory symptoms, making reactive arthritis and poststreptococcal arthritis less likely.
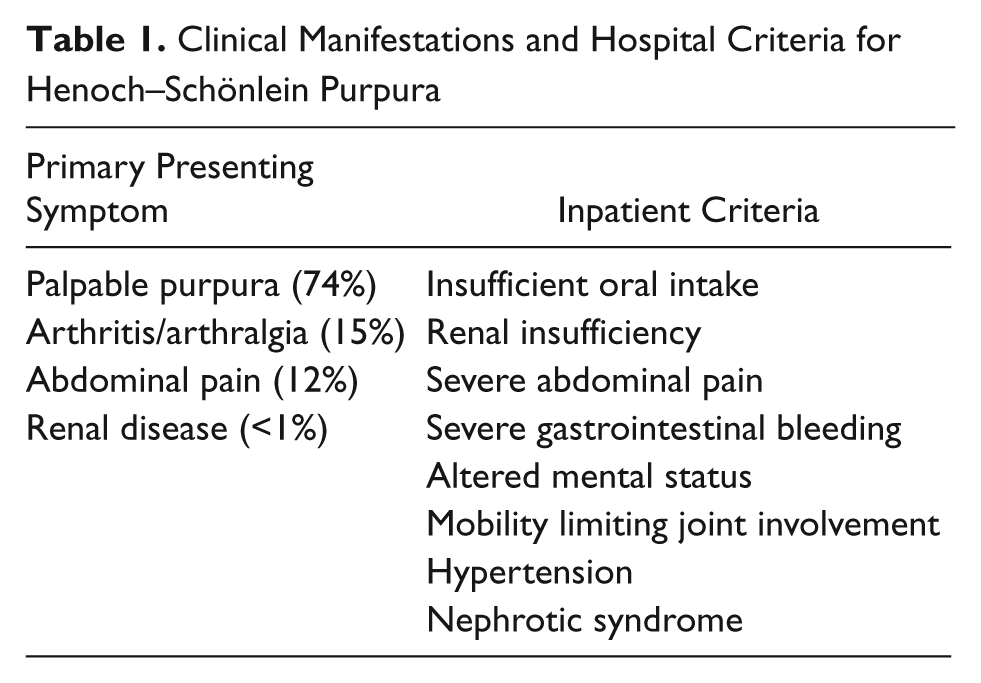
Henoch–Schönlein purpura classically presents with a tetrad of symptoms: purpuric rash, abdominal pain, arthralgia, and renal dysfunction (Table 1). 4 These symptoms vary widely in both the timing and severity of their presentation. HSP, as the name implies, classically presents with a purpuric rash in gravity-dependent areas such as the buttocks, legs, and arms. The rash is not associated with thrombocytopenia or coagulopathy. 3 While purpura is the most common presenting symptom, approximately one fourth of HSP patients do not have a rash at initial presentation. 2 In fact, the classic HSP can occur days or weeks prior to, or following, other presenting symptoms. Therefore, pediatricians should set a low threshold for HSP diagnosis if other associated HSP signs and symptoms are present. 5
Clinical Manifestations and Hospital Criteria for Henoch–Schönlein Purpura
Approximately 63% of HSP patients in the United States present with a gastrointestinal (GI) symptom, most commonly abdominal pain. 5 GI symptoms generally present within 8 days of rash appearance and can last weeks to months following the disappearance of purpura. 5 As mentioned above, abdominal symptoms can occur prior to purpura formation in up to 35% of patients, often making the disease difficult to diagnose.5,6 Abdominal pain associated with HSP is generally diffuse and can be transient, constant, colicky, or waxing and waning in presentation. Furthermore, it is not uncommon for a HSP patient to have GI bleeding associated with their abdominal pain.
Arthralgia occurs in up to 84% of patients and tends to be oligoarticular, transient, or migratory and affect the large joints of the lower extremity. 5 HSP arthralgias can be associated with tender, swollen joints and can be difficult to differentiate from other causes of pediatric arthralgia. Effusion and erythema are notably absent, and no long-term deformation sequela occurs. 7
The final symptom of the tetrad is renal disease, which usually occurs within 4 weeks of diagnosis. In the United States, approximately 40% of HSP patients manifest a sign or symptom of renal disease such as microscopic or gross hematuria, proteinuria, nephritic syndrome, and glomerulonephritis. 8 Less common symptoms involving other organs can also occur, including periorbital edema, scrotal edema and torsion, keratitis, uveitis, headache, neuropathy, and interstitial pulmonary disease.4,5
Many of the tests ordered in the above case were not necessary in the workup of HSP. The diagnosis of HSP may be made clinically when the classic signs and symptoms are present. However, diagnosis can oftentimes be difficult when the classic purpuric rash is absent. 4 There is currently no diagnostic laboratory test for HSP. Interestingly, up to 50% to 70% will have increased serum IgA, though this test is neither sensitive nor specific for the disease. 9 Certain laboratory tests can help differentiate HSP from other potential etiologies in the differential diagnosis. For example, antibodies such as ANA and ANCA (antineutrophil cytoplasmic antibody) can help rule out other vasculitidies. Serum complement, rheumatoid factor, and anti-dsDNA may help distinguish HSP from systemic lupus erythematous or juvenile idiopathic arthritis. ASO titers are often used to differentiate acute rheumatic fever from HSP. However, this test should be used with caution given that streptococcal infection is a common inciting event in the progression of HSP. Definitive diagnosis is determined using either skin or renal biopsies. Skin biopsy demonstrates leukocytoclastic vasculitis with IgA deposition. Renal biopsy typically shows mesangial IgA deposition, mesangial proliferation or, in severe cases, crescentic glomerulonephritis. 10
Although most cases of HSP resolve without acute disease or long-term sequela, there are uncommon, yet serious, associated conditions that require close observation. Intussusception, typically ileocolic, occurs in approximately 0.4% to 3.5% of patients and can be difficult to distinguish from the typical waxing and waning HSP abdominal pain. 11 Patients with severe disease can also progress to nephrotic syndrome and acute renal failure with concomitant hypertension.7,12 Inpatient criteria for HSP are designed to limit and treat these serious conditions (Table 1), including GI bleedings, acute abdominal pain, and signs of renal failure (hypertension, increased creatinine, etc).3,4
Management of HSP is typically supportive. The mainstay of pharmacologic intervention is nonsteroidal anti-inflammatory agents (NSAIDs). Patients tend to respond clinically to agents such as ibuprofen and naproxen, and these drugs are generally well tolerated by patients.4,5 NSAIDs are recommended for symptomatic relief of both joint and abdominal pain. In cases of acute GI bleed or glomerulonephritis, NSAIDs should be used with caution because of their effects on platelets and renal function.
The use of corticosteroids in the treatment of HSP is somewhat controversial, with few studies demonstrating changes in the disease course or progression. A recent systemic review of 201 published studies found that corticosteroids did not decrease the median time to resolution of abdominal pain in patients with HSP. 13 As a result, corticosteroids are generally used only in cases of severe, persistent, or recurrent disease. However, the review did find that steroid treatment is associated with a decreased incidence of persistent renal disease in severe cases. Furthermore, steroids may reduce the need for overall surgical intervention in complicated HSP, though this trend was not statistically significant. To date, there is no long-term study detailing the benefits of corticosteroid administration, and their use is not recommended in mild to moderate disease.
The prognosis of HSP is excellent, with most cases resolving within 1 month of diagnosis.12,14 Approximately one third of patients will have a recurrent episode within 3 months and subsequent episodes tend to be less severe and of shorter duration than the initial event. Furthermore, rates of serious complications such as renal failure and intussusception are decreased in recurrent episodes compared with initial diagnosis. Morbidity resulting from HSP is typically due to complications of intussusception, bowel ischemia/perforation, and renal disease. 5 Renal prognosis, even in severe disease, is generally favorable. Long-term renal disease is less common in children than in adults, with only 0.01% of children having microscopic signs of renal disease 2 years after presentation.2,14 Overall, most pediatric patients respond well to supportive treatment and do not have long-term sequela resulting from HSP.
Footnotes
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The authors received no financial support for the research, authorship, and/or publication of this article.