
Abstract
Objective. To evaluate reliability of umbilical cord blood (UCB) for complete blood count (CBC) and blood cultures compared with the infant’s blood from peripheral site for group B streptococcal (GBS) sepsis screening. Methods. A total of 200 neonates, at risk for GBS infection, were studied prospectively. After birth, UCB sample was obtained for CBC and blood cultures from umbilical vein. Peripheral arterial/venous blood was obtained from the neonate. Results. In 200 neonates, CBC counts were similar for clinical significance except for leukopenia (6% in UCB vs 1.2% in peripheral blood, P = .02). One UCB sample grew GBS and another grew microaerophilic streptococcus, a contaminant. A neonatal sample grew Escherichia coli, a pathogen and another neonatal sample grew Staphylococcus auricularis, a contaminant. Conclusion. CBC results were similar from UCB and the infant for the purpose of GBS screening. Contamination of UCB sample for culture is uncommon. Hence, UCB may be used for GBS sepsis screen.
Group B streptococcus (GBS) is a major cause of early-onset neonatal sepsis. Infants born to mothers with GBS colonization are at increased risk of developing GBS sepsis. Before recommendations for prevention of early-onset GBS disease by maternal intrapartum antibiotics prophylaxis, the incidence of GBS sepsis was 1 to 4 cases per 1000 live births and approximately 1 per 23 to 225 GBS colonized women. Mortality rates range from 5% to 10% but are higher in preterm infants. 1 Studies have consistently shown reduction in the rate of GBS infection in neonates if mother is given intrapartum antibiotic prophylaxis.2-4 The Committee on Infectious Diseases in 1997 recommended intrapartum chemoprophylaxis to prevent GBS infections in neonates. Criteria for intrapartum chemoprophylaxis include (a) Screening-based strategy: All pregnant women at 35 to 37 weeks gestation are swabbed from the vagina and the rectum for GBS. If cultures are positive for GBS, intrapartum chemoprophylaxis should be provided; and (b) Risk factor-based strategy: In this method, no cultures are performed at 35 to 37 weeks, but the following risk factors are considered for prophylaxis—(1) previous infant with invasive GBS disease, (2) GBS bacteriuria during current pregnancy, (3) delivery at <37 weeks of gestation, (4) duration of rupture of membranes ≥18 hours, or (5) maternal temperature ≥100.4°F (38°C). 5
Standard intrapartum chemoprophylaxis is either intravenous penicillin G or ampicillin. Two or more doses of ampicillin or penicillin given 4 hours apart is considered as adequate prophylaxis. Infants born at <35 weeks gestation in spite of appropriate prophylaxis and ≥35 weeks gestation infants that received ≤2 doses of intrapartum antibiotics are considered “at-risk infants” for GBS sepsis. It is recommended that these “at-risk infants” should have complete blood count (CBC) with differential and a blood culture as a sepsis screen. 5 In our experience, nearly 10% or 200 to 300 mostly asymptomatic neonates undergo GBS sepsis screen (CBC and a blood culture) each year at our institution.
Often, it is difficult to obtain an adequate volume of blood from neonates with small and delicate veins. In 1986, Neal et al 6 revealed a wide range of blood quantities obtained from neonates to do blood cultures. The mean blood volume per aerobic bottle was 0.53 mL (range = 0.01-1.9 mL). An inadequate amount of blood inoculated in the blood culture bottle may yield a negative result or a delay in the interpretation of bacterial growth. 6 According to Schelonka et al, 7 1 to 2 mL of blood should increase microorganism recovery in the face of low-colony count sepsis. To obtain blood cultures, the neonate may require multiple venous or arterial sticks. Heel-stick capillary samples are of uncertain value because of contamination and other complications.8-10 Blood sampling from the neonate produces significant pain very early in life. Umbilical cord blood is a readily available and abundant source of blood that is derived from the infant. Umbilical cord blood can be obtained without pain or procedures to the neonate. In sick preterm infants with respiratory distress, it has been a standard of practice to obtain CBC and a blood culture after placement of indwelling umbilical vein or artery catheter in the infant. 11
Even though there are studies obtaining blood from an excised (detached from the infant) umbilical cord for blood cultures in 1960s and 1970s, these studies are not well controlled. Bacterial contamination has been an issue in these studies.12-14 A recent study showed some promise in terms of using cord blood for culture when the sample is obtained after meticulous cleaning. 15 Since GBS sepsis screen (CBC and a blood culture) has become a common practice, we decided to evaluate the reliability of umbilical cord blood sampling for CBC and blood culture and compare with the infant’s blood from a peripheral site for this purpose.
Methods
The study was approved by the institutional review board and was conducted from September 1998 to March 2000 (approximately 18 months). The term and preterm infants who met the study criteria and who were born at the institution were enrolled. These were the “at-risk infants” for GBS infection because of the maternal risk factors as described in the introduction and qualify for “intrapartum prophylaxis with antibiotics” as per Centers for Disease Control and Prevention (CDC) guidelines. 5 The infants with the following additional criteria were included in the study: Infants ≥36 weeks gestation and who received <2 doses of intrapartum antibiotics for prophylaxis and preterm infants ≤35 weeks gestation regardless of number of doses of intrapartum antibiotics.
The following tests were performed for the purpose of the study as a part of sepsis evaluation: (a) CBC and blood cultures from the neonate, and (b) CBC and blood cultures from the umbilical cord.
Blood Sample Collection
From the umbilical cord
After the neonate was enrolled, at delivery, a pair of sterile hemostat clamps was applied at the distal end of the cord near the neonate’s umbilicus and another pair of hemostat clamps was applied at the end of the cord near the placenta. The segment of the cord in between the clamps was excised and placed in a sterile container. The isolated cord segment was then swabbed 3 times along the surface with 10% povidone-iodine solution swabsticks. After allowing 30 to 60 seconds to allow for the povidone-iodine to dry, the site was cleansed off with sterile alcohol preps using a new prep each time. After the site was swabbed, blood was drawn from the umbilical vein using a sterile 23-gauge needle and syringe. One to two milliliters of blood was obtained from the umbilical cord. BacT/Alert PediBactT aerobic culture bottles (Organon Teknika Corporation, Durham, NC) were used. 16 The plastic flip-top was removed from the bottle and the top of the bottle was disinfected with an alcohol pad. The blood was then inoculated into the BacT/Alert PediBactT aerobic culture bottle. All blood culture bottles were labeled with the neonate name, medical record number, date, time, site of blood collection, and blood collector’s initials.
From the neonate
The enrolled neonate’s sites for blood collection were evaluated. Common peripheral sites for blood collection from neonates were the veins in antecubital area, hands, feet, and the radial artery. The chosen site was swabbed 3 times in a circular manner from the inside to the outside area with 10% povidine-iodine swabsticks. After allowing 30 to 60 seconds to dry, the site was cleansed with sterile alcohol preps using a new prep each time the site was swabbed. One to two milliliters of blood was drawn from the site using a sterile syringe and a 25- to 23-gauge needle.
Some neonates had blood cultures drawn in a sterile manner from a newly inserted umbilical arterial or venous catheter as this is a common and accepted practice in intensive care nurseries for neonates with respiratory distress that require monitoring arterial oxygen tension. 11 The umbilical cord was prepped 3 times with 10% povidone-iodine swabsticks. After the abdomen was draped with sterile towels and the betadine was allowed to dry, the umbilical artery or vein was visualized. A 5 French or 3.5 French umbilical catheter was inserted and when blood return was obtained, one to two milliliters of blood was withdrawn from the vessel. Umbilical arterial or venous catheters were inserted only as clinically indicated and not for the sole purpose of obtaining a blood culture. Obtained blood samples were placed in the blood culture bottles as described before. Blood was also obtained for a CBC from the umbilical cord and the neonatal sampling site for comparison.
Laboratory Testing of Blood Samples
Culture method
Blood culture samples from the umbilical cord and from the neonate were processed by the microbiology laboratory of the hospital. The tops of the culture bottles were cleansed with an alcohol pad and then vented with a vent needle in the microbiology laboratory. The bottles were then placed in the BacT/Alert automated Colorimetric System (Organon Teknika Corporation). 16 The cultures were kept in this system for 5 days when the cultures were negative. If the cultures become positive, an audible alarm is heard and the blood cultures are then transferred to 5 different media plates. The plates consist of blood, chocolate, MacConkey, CNA, and brucella agar. A gram stain was performed on positive bottles and if the gram stain was negative then the bottle was considered a false positive. A false positive may occur if the blood sample has an increased amount of protein or white blood cells (WBC) causing the BacT/Alert system to perceive a sample as positive. 11 Cultures were incubated at 37°C. The cultures were read daily by a laboratory technician. Positive specimens had the organisms identified and sensitivities recorded. The cultures were checked through the lab computer system for 5 days. If there was no growth on a blood culture at the end of 5 days, the cultures were classified as negative. 17
Complete blood count
The blood required for a CBC is 0.25 to 0.5 mL collected in a lavender top bullet. When the blood is drawn from the umbilical cord for blood culture, blood is also obtained for the CBC. Blood from the neonates for a CBC were obtained from peripheral vein or artery by a heel-stick. The CBC was sent to hematology laboratory and the bullet was checked for clots in the sample. If the sample did not have any clot formation, a drop of blood was placed on a slide for a differential smear. The bullet was then manually placed in the Coulter STKS automated complete blood cell count instrument (Beckman Coulter Inc, Brea, CA). This instrument calculated the white blood cell count, red blood cell count, and platelet count. Indices such as hematocrit, hemoglobin, mean corpuscular hemoglobin content, mean corpuscular volume, mean corpuscular hemoglobin, and red cell distribution width were calculated. A 7-part automated differential included polymorphonuclear leukocyte, lymphocyte, bands, basophil, monocyte, and eosinophil counts. If the results of the CBC from the Coulter STKS did not meet the parameters for normal values, the differential smear was evaluated manually. Verification of abnormal CBC values was performed by microscopic examination of the differential smear.
Data Collection
A data collection form was used. The data collected from the mother included details of the delivery such as maternal fever, evidence of chorioamnionitis, presence of risk factors for neonatal sepsis, and details of intrapartum antibiotic prophylaxis. Neonatal data collection included birth weight, gestational age, Apgar scores, any neonatal symptoms related to sepsis, CBC, and the results of blood cultures. Also, the difference in time from birth to the time blood samples were drawn was documented.
Statistical Methods
The agreement between the umbilical cord blood sample and neonatal sample with respect to CBC was assessed by computing correlation coefficient for each component and by comparing means using the paired t test. The sensitivity and specificity of umbilical cord blood culture to predict neonatal blood culture results was estimated using exact 95% confidence intervals (CI). McNamara χ2 test was used to evaluate the positive and negative blood culture results. P < .5 indicates statistical significance. Type of bacteria isolated from blood samples of umbilical cord and neonate was compared.
Approximately 2500 infants are delivered at this institution each year. Review of nursery outcome database from 1989 to 1997 revealed that approximately 285 infants per year had sepsis evaluations. Hence, we estimated that approximately 200 infants would be available for study participation after exclusion criteria/families unwilling to participate in the study. It is estimated that a sample size of 200 cases should give 90% power if correlation between the cord blood and the neonatal blood for any component of the CBC is as large as 0.23. Assuming approximately 10% would have a positive culture for microorganisms; we anticipated 20 cases would be available to estimate sensitivity and 180 to estimate specificity. However, the study reflected a much lower incidence of culture positivity.
Results
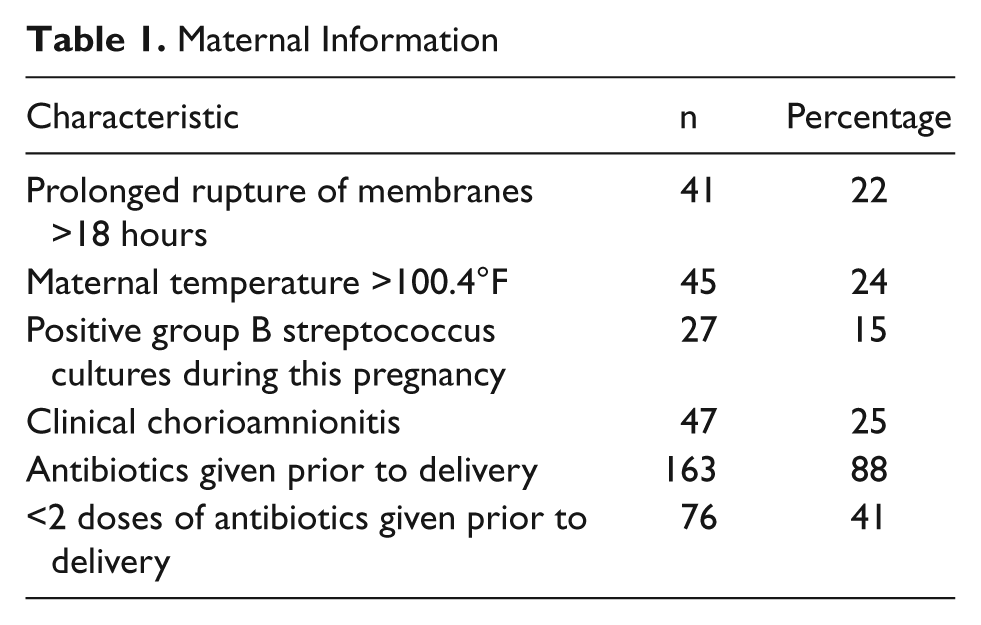
A total of 200 infants were recruited in the study as planned. Mean birth weight was 2346 g with SD of 948 g. Mean gestational was 34.4 weeks with SD of 4.4 weeks. One hundred (50%) of these infants were male. Maternal characteristics are shown in Table 1. Seventy-six patients did not receive adequate prophylaxis. However, 163 patients received antibiotics either because of chorioamnionitis or other reasons such as <35 weeks gestation, or because of inadequate number of doses and still required sepsis evaluation. Neonatal characteristics are shown in Table 2. The neonate’s blood sample was drawn at the age of 58.2 ± 36.9 (mean ± SD) minutes. The infant’s blood sample was obtained from the following sites: antecubital 79 (40%), dosum of the hand 39 (20%), dosum of the foot 2 (1%), radial artery 52 (26%), and umbilical artery/vein 26 (13%).
Maternal Information
Neonatal Characteristics
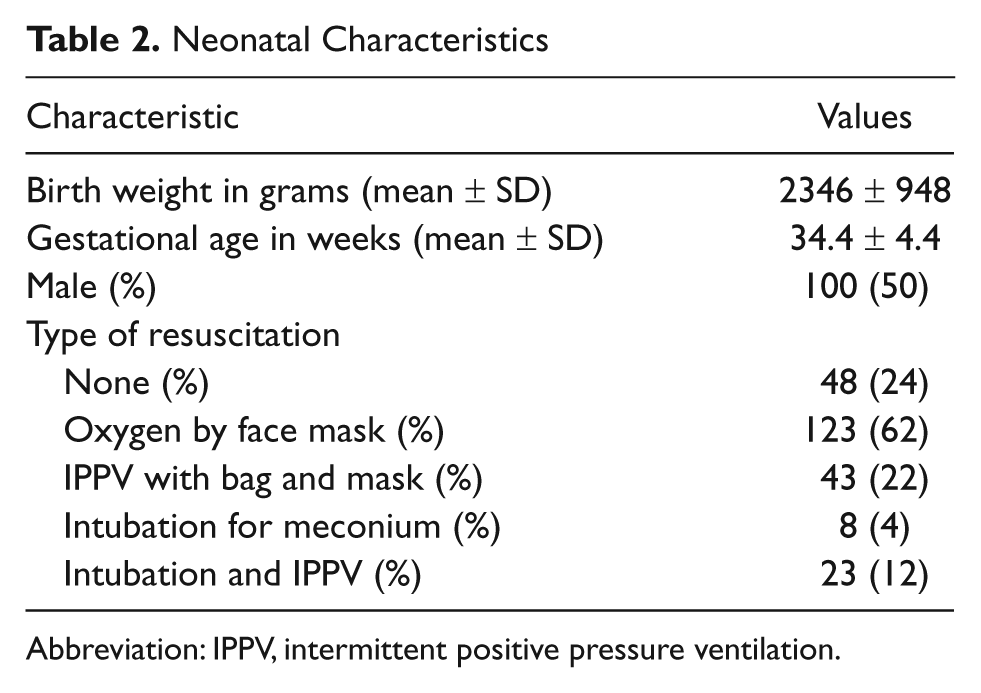
Abbreviation: IPPV, intermittent positive pressure ventilation.
Complete Blood Counts
There were 172 paired samples for CBC from the cord and from the neonates. Comparison results are shown in Table 3. Clinical significance of the blood counts is shown in Table 4.5,18,19 Hematocrit and platelet counts were similar for clinical significance in both samples. WBC counts >30 000/mm3, immature to total neutrophil ratios (I:T ratio) >0.2 and absolute neutrophil count <1500/mm3 were also similar for clinical significance. However, low WBC counts (<5000/mm3) were 10 (6%) in cord blood and 2 (1%) in the neonatal samples (P = .02).
Complete Blood Count Comparison
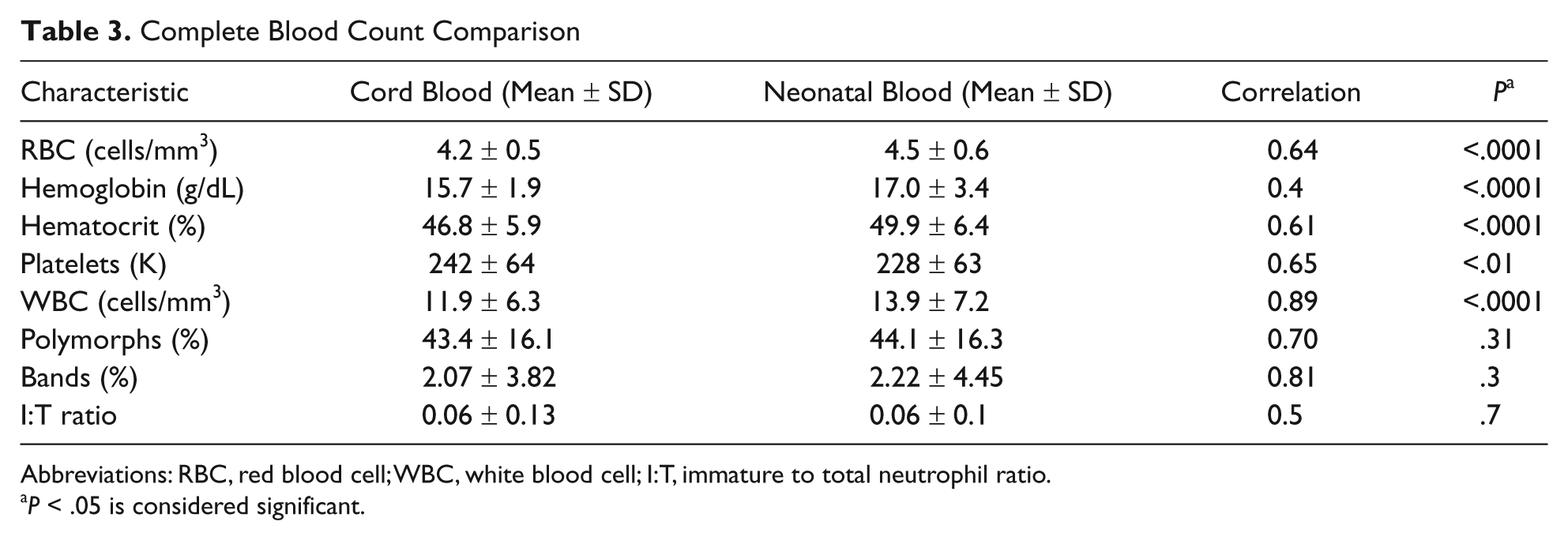
Abbreviations: RBC, red blood cell; WBC, white blood cell; I:T, immature to total neutrophil ratio.
P < .05 is considered significant.
Complete Blood Count and Clinical Significance
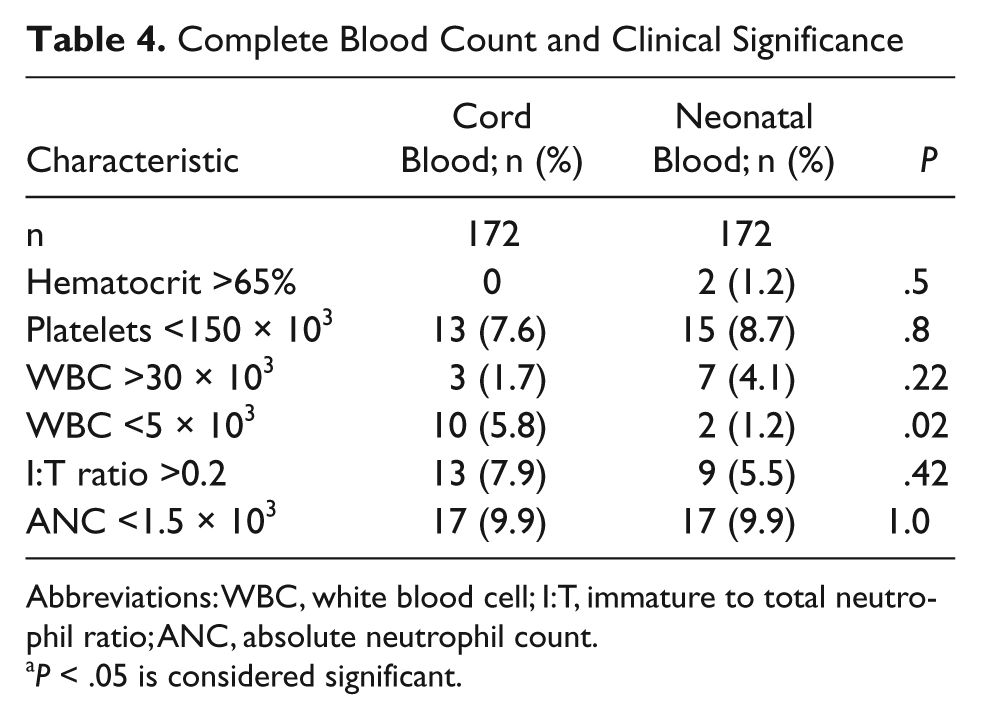
Abbreviations: WBC, white blood cell; I:T, immature to total neutrophil ratio; ANC, absolute neutrophil count.
P < .05 is considered significant.
Blood Cultures
Blood culture results are shown in Table 5. There were 198 infants who had cord blood samples out of 200 infants recruited. Two infants had no cord blood sample available because of inadequate volume but had enough sample for CBC. There were 305 blood culture samples directly obtained from infants. In all, 105 infants had 2 cultures obtained. 20 From the cord, 1.96 ± 2.44 mL (mean ± SD) of blood was obtained for each culture compared with 1.05 ± 0.23 mL (mean ± SD) for each blood culture from the neonate (P < .0001). Out of 198 cord blood samples, 196 (99%) samples grew no bacteria compared to 303 (99%) out of 305 neonatal samples. There was one (1 in 198; 0.5%) possible contamination in cord blood sample. The 95% CI for contamination of cord blood samples is 0.01% to 2.8%. The organism was microaerophilic streptococcus. The infant was asymptomatic with normal CBC. One (1 in 305; 0.3%) neonatal sample grew possible contaminant (Staphylococcus auricularis). The infant was asymptomatic and CBC was normal. There was one sample in cord blood (1 in 198; 0.5%) that grew GBS whereas the infant’s sample was negative and infant was symptomatic with tachypnea (38 weeks gestation, required positive pressure ventilation with bag and mask at delivery, abnormal I:T ratio = 0.23, infant’s samples were drawn at 33 and 42 minutes, umbilical volume 0.8 cm3, infant’s volume 0.7 and 0.8 cm3). In neonatal samples, one (1 out of 305; 0.3%) grew Escherichia coli whereas cord blood was negative and infant was symptomatic with respiratory distress (normal WBC and normal I:T ratio, 34 weeks gestation infant with grunting and respiratory distress, infant’s sample obtained at 58 minutes of age, umbilical volume 3.0 mL, neonatal volume 1.0 mL).
Comparison of Blood Culture Results
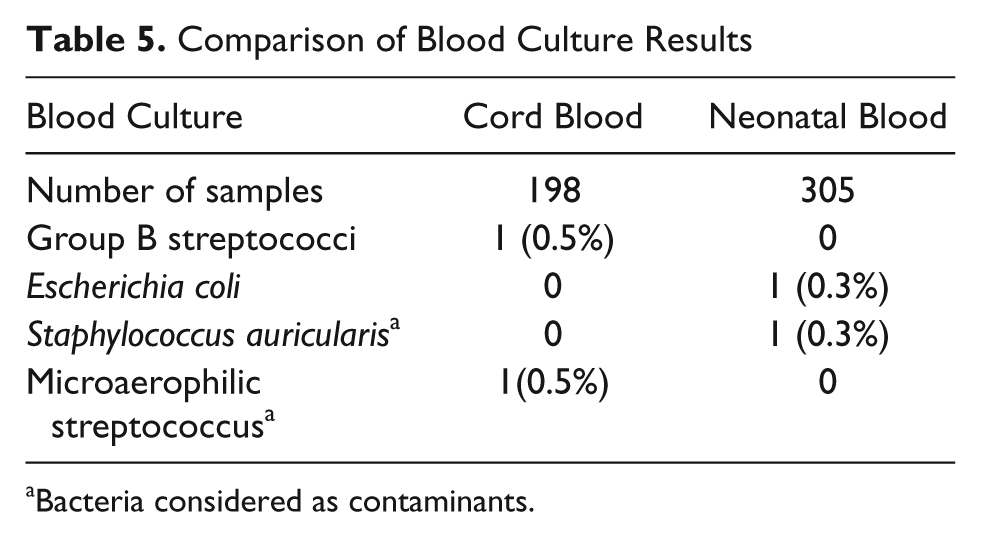
Bacteria considered as contaminants.
Discussion
This is a unique study that sought to evaluate utilization of blood samples obtained from excised umbilical cord for GBS sepsis screening. It evaluated both components (CBC and blood cultures) of sepsis screen as required by the CDC protocol. It showed that cord blood sample is similar to the infants’ sample for sepsis screening purpose in both CBC and blood culture result. This method potentially saves pain, suffering, and other disadvantages of obtaining a blood sample from several hundred thousand babies a year as GBS screening is a very common clinical situation. Studying the possibility of using umbilical cord blood as a source of blood for culture is not an original idea.
In 1963, Pryles et al 12 in an attempt to evaluate prolonged rupture of membranes in the pathogenesis of infection in the newborn studies 358 parturient mothers. The study group comprised of 179 mother/infant pairs with rupture of fetal membranes >6 hours duration and a control group with 179 mother/infant pairs with rupture of membranes <6 hours duration. Positive cord blood cultures were noted in 47% of the study group and in 37% of the control group. The organisms isolated from these cultures were found in the maternal vaginal and urine cultures. 5 The purpose of this study was not to compare specifically umbilical samples to the infant’s samples and this is only small part of a bigger study evaluating pathogenesis of neonatal sepsis. Umbilical blood was drained into a flask for cultures. Hence this cannot be compared with recent studies. Of the 150 neonates with positive cord blood cultures, 24% or 11% showed signs and symptoms of infection. Contamination appears to play a major role in the high incidence of positive cord blood culture in this study. No simultaneous control samples were obtained from the infants.
Tyler and Alberts 13 in 1966 obtained blood cultures from the umbilical cord of neonates between 28 and 42 weeks of gestation, and all women were in active labor. Rupture of membranes >24 hours were associated with higher incidence of umbilical cord bacteremia. The method of blood collection is documented in this study and the umbilical cord was prepped with iodine, pHisoHex and ethanol. The results revealed 30 positive umbilical cord blood cultures out of 319 infants (9.4%). Of the 30 positive cord blood cultures, 10 neonates showed signs of illness. Among the bacteria found in the cord blood cultures were E coli, enterococcus, anaerobic and viridians group, GBS, and Staphylococcus aureus. Staphylococcus epidermidis, which is often nonpathogenic, was isolated from 10 (33%) cultures; 2 of the 10 neonates had clinical illness. This investigation sought mainly to describe some of the perinatal factors associated with umbilical cord bacteremia/neonatal bacteremia and simultaneous blood cultures were not obtained from infants.
In 1979, Salem and Thadepalli 14 studied microbial invasion of the placenta, cord and membranes during active labor. They investigated 51 consecutive full-term deliveries. The authors prepared the cord with iodine. Maternal cervical cultures were obtained and peripheral venous cultures were obtained from the neonates when infection was suspected. Fifteen of the 51 cord blood samples (29.4%) grew out bacterial. Only 1 newborn infant developed clinically recognized sepsis. Staphylococcus epidermidis was isolated from the cord blood and the peripheral venous blood. The other 9 neonates with positive cord blood cultures did not have peripheral blood cultures obtained from the infant. Five of the 15 cord cultures had the same organisms as was isolated from the maternal cervix. The primary purpose of this study is not utilization of cord blood in place of peripheral blood sample but to elucidate invasion of bacteria on cord, placenta, and the membranes.
Herson et al 21 obtained large volume of placental blood sample from fetal side of placenta (not from excised umbilical cord) after delivery in 81 patients and compared with neonatal blood cultures in 35 high risk neonates. Ten out of 81 placental samples grew bacteria whereas 2 out of 35 neonatal samples were positive. The authors felt that only 3 out of 81 (3.7%) were due to contaminants. These are large volumes (>5 mL) of blood drawn for cultures only from placenta, not from umbilical cord.
In 1981, Polin et al 15 reported on using umbilical cord blood culture for the detection of neonatal bacteremia. The study enrolled patients with rupture of membranes before the onset of labor, prolonged rupture of membranes >24 hours before delivery, intrapartum fever of an oral temperature >38°C during labor, and patients without complications. Two hundred umbilical cord blood cultures were obtained during the study. This study was specific with regard to blood collection. Peripheral blood cultures were obtained from 29 infants in the study compared to 200 cord blood samples. Seventeen cultures were performed because of premature rupture of membranes/intrapartum fever. The remaining 12 cultures were done because of clinical signs of sepsis observed in the neonate. Six umbilical cord blood cultures were positive (3%). Three cultures (1.5%) exhibited delayed growth at more than 48 hours (considered not clinically significant), 2 cultures (1%) were positive with organisms considered contaminants, and the 1 culture (0.5%) correlated to the neonate’s peripheral venous blood culture which grew out beta-hemolytic streptococcus (GBS). The authors concluded that umbilical cord blood cultures may prove to be a satisfactory alternative to postnatal peripheral blood culture for the evaluation of neonatal bacteremia.
More recently, Hansen et al 22 reported in 2005 of the possibility of using umbilical cord blood in place of infant blood when studying neonatal sepsis. Of note, this study only included term infants in their evaluation. Although a small study, their results strongly support our findings. One hundred and thirteen paired samples of cord and infant venous blood samples were compared with blood cultures, I:T granulocyte ratio, and CBC with differential counts to determine the accuracy of cord versus infant blood results. This study concluded that cord blood could safely replace infant blood for evaluation of sepsis as demonstrated by negative findings in all 113 cord and infant blood cultures. Also, the CBC results of WBC, hematocrit, and platelet counts from cord and infant blood showed moderate to high association. As the authors suggest, a lack of positive findings was a limitation to their study, as it did not provide data to extrapolate sensitivity characteristics according to source.
Our study was designed to improve on the deficiencies of previous studies and also sought to evaluate CBC, which is usually a part of sepsis evaluation. Since initiation of intrapartum GBS prophylaxis protocols, nearly 10% to 15% of infants are being screened for sepsis. Obtaining a proper blood sample from an infant is painful as it requires multiple needle sticks and uses significant skilled man power and to some extent separates the infant from mother for a significant amount of time when bonding is critical. It is also difficult to obtain the proper amount of blood sample from the infant, unlike obtaining a sample from the cord.
This study revealed statistical differences in CBC between cord blood samples and the infant’s samples in terms of RBC, hemoglobin, hematocrit, and WBC. These values were higher in cord blood samples. Platelet counts are slightly higher in cord blood for similar reason. Differential counts were similar in both cord blood and peripheral samples. However, for clinical significance the values are similar. We speculate that the differences were probably because of central nature of umbilical cord blood sample versus peripheral vessels from the infant. Time lag of approximately an hour between time of birth and obtaining neonatal samples may account for some of the differences. Leukopenia was noted more often in cord blood samples (5.8% vs 1.2%) hence we did not miss the opportunity to identify an infant with potential sepsis.
Higher blood volumes and ease of drawing blood without inflicting pain on the infant are the main advantages. Proper preparation of the umbilical cord eliminated the issue of contamination as the infant’s samples and cord blood sample had a very low rate of contamination (0.5%). Only one positive culture for GBS was noted in 1 cord blood sample and the infant’s sample (one sample) was negative. This may be because of good sample volume from the cord versus the infant or probably because of transient bacteremia described in neonates. It is a concern as one infant grew E coli on 1 blood culture from the infant and the cord blood culture was negative. The infant’s culture was drawn nearly an hour after delivery. It is possible that continued multiplication of organisms during that period in the infant is possible cause. Strengths of the study are that this is a well-controlled study with 198 blood cultures form the cord blood compared with 305 neonatal blood culture samples from same infants ie, 105 infants had 2 peripheral blood cultures drawn. All infants are at high risk for GBS infection as per CDC protocol.
In conclusion, CBC and blood cultures obtained from umbilical cord are reliable for clinical purpose of GBS infection screening with very little contamination. However, it is advised that one obtains additional blood culture sample from the infant if the infant is symptomatic and if one intends to start antibiotics for clinical sepsis for additional assurance. Because of low yield of blood cultures in this population, the policy of obtaining routine blood cultures in this population needs reconsideration.
Footnotes
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The authors received no financial support for the research, authorship, and/or publication of this article.