
Abstract
The authors assessed the ongoing needs of 34 pediatric dog bite victims and their families 1 month after receiving care in a pediatric emergency department. More than 70% of the parents noted at least 1 new concerning behavior in their children, and more than 85% of the parents also endorsed concerns about their own reactions. Half of the parents believed that children, in general, might benefit from interventions to help with postbite fears and nearly three quarters felt that families would benefit from education regarding dog bite prevention. The majority (85%) of the parents believed that additional supportive services could be offered effectively at emergency department or pediatric office/clinic visits. A template for a dog bite information card is presented.
Introduction
People in the United States own nearly 77.5 million dogs, 1 and each year approximately 4.5 million people are bitten by dogs. 2 Children are often the victims of these dog bites and frequently sustain significant injuries needing emergency care. The highest rates of dog bite–related emergency department (ED) visits in 2008 were for children aged 10 years and younger. 3
Although injuries such as laceration and tearing wounds from dog bites are often apparent, less noticeable are the psychological ramifications for bite victims and their families. Such consequences can include post traumatic stress or the more severe, posttraumatic stress disorder (PTSD). Unrecognized and untreated symptoms of PTSD in children can lead to impairment in brain development and cognitive, behavioral, and social skills.4-6 One survey of pediatric dog bite victims found that more than 50% had PTSD symptoms for more than 1 month and more than a quarter met all DSM-IV criteria for PTSD. None of these children had received psychological support. 7
In addition to the physical and emotional/behavioral consequences of dog bites to children, other sequelae, including financial and legal issues, may be experienced by family members. In 2008, the average cost of a dog bite–related hospital stay was $18 200, approximately 50% higher than the average injury-related hospital stay. 3 In the legal arena, there are claims that both the insurance industry and the legal system respond ineffectively, leaving plaintiffs without deserved compensation. 8
Most dog bite programs target prevention education (American Veterinary Medical Association, The Humane Society of the United States, Doggone Safe) because children’s knowledge of appropriate dog bite prevention is lacking. 4 We know of no studies or pediatric programs, however, that assess for ongoing needs of dog bite victims and their families or offer a continuum of care after the acute management of the dog bite. The goals of this study were to (a) estimate the need for supportive services including medical, mental health, and prevention interventions for children who were victims of dog bites and their families and (b) gather input on types and timing of delivery of supportive services that could be offered in a continuum of care (including behavioral and medical symptoms; relevant legal, insurance, and animal control issues; and dog safety training).
Methods
Design and Setting
With approval from the hospital institutional review board, this descriptive study of pediatric dog bite victims and their parents was conducted in the ED of an urban, pediatric trauma center that sees more than 300 dog bite victims each year.
Participants
Participants were identified by a live computer tracking system and enrolled by a trained clinical research coordinator. Inclusion criteria were age (0 months to 16 years) and a presenting complaint of “dog bite.” Exclusion criteria were being previously enrolled in this study or having a non-English speaking parent as the informant. Consent for study participation was obtained from parents and assent was obtained from children ages 11 and older.
Data Collection
After enrollment, the parent completed a brief questionnaire that included follow-up contact information, parent and patient demographics, details of the bite incident, and characteristics of the biting dog. On completion of the questionnaire, participants were given a book Good Dog! Kids Teach Kids About Dog Behavior and Training, 9 in which an affixed note identified investigators’ contact information and the parent-selected preferred date/time for a follow-up phone call.
Approximately 4 weeks after the initial ED visit, parents were contacted by investigators for a phone interview lasting about 30 minutes. Information obtained during the interview included (a) bite incident specifics, (b) further medical/psychological care needed by the child related to the dog bite, (c) contact with additional agencies (eg, health department, insurance, legal, police, animal control), (d) changes in the child’s behavior after dog bite, (e) changes in parental concerns about themselves and their children since the dog bite, and (f) parent feedback on the value of having additional services and information available in pediatric practices related to care of the dog bite victim and prevention of future dog bites.
Data Analysis
Descriptive statistics of the data included means, standard deviations, minimums, maximums, medians, and percentages.
Results
Fifty participants were enrolled and 34 (68%) completed the follow-up interviews. The mean age of the children was 8.0 years (standard deviation = 3.94) and 62% (21/34) were male. The mother was the parent participant in 82% (24/34) of the interviews. The majority (79%; 27/34) of adult participants reported having a high school education or greater.
Seventy-four percent of the participants (25/34) stated that they knew the biting dog, and nearly half (41%; 14/34) identified the dog as their own or their family’s dog. More than half (56%; 19/34) of the dog bite incidents occurred while the child and dog were outside, and the majority of bites (80%; 27/34) were not witnessed by the parent. Location of the bite injuries on the children is noted in Figure 1. None of the participants were hospitalized; 53% (18/34) received follow-up medical care, with about half (55%) seen in the ED and the others seen in pediatric practice settings. Only 1 parent stated that her child might need further medical care “possibly for cosmetic surgery.”
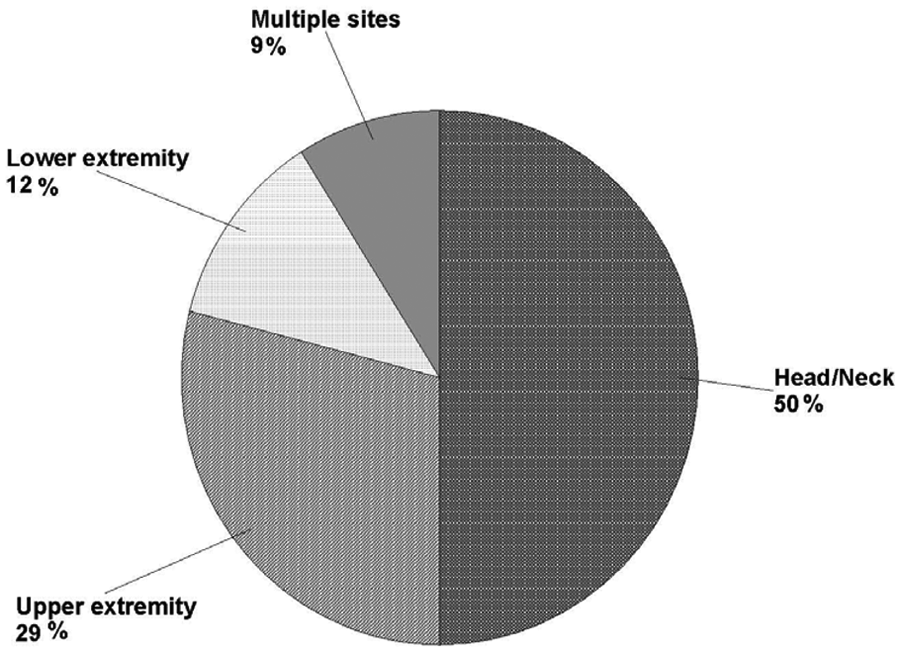
Location of dog bite injuries on child’s body (N = 34)
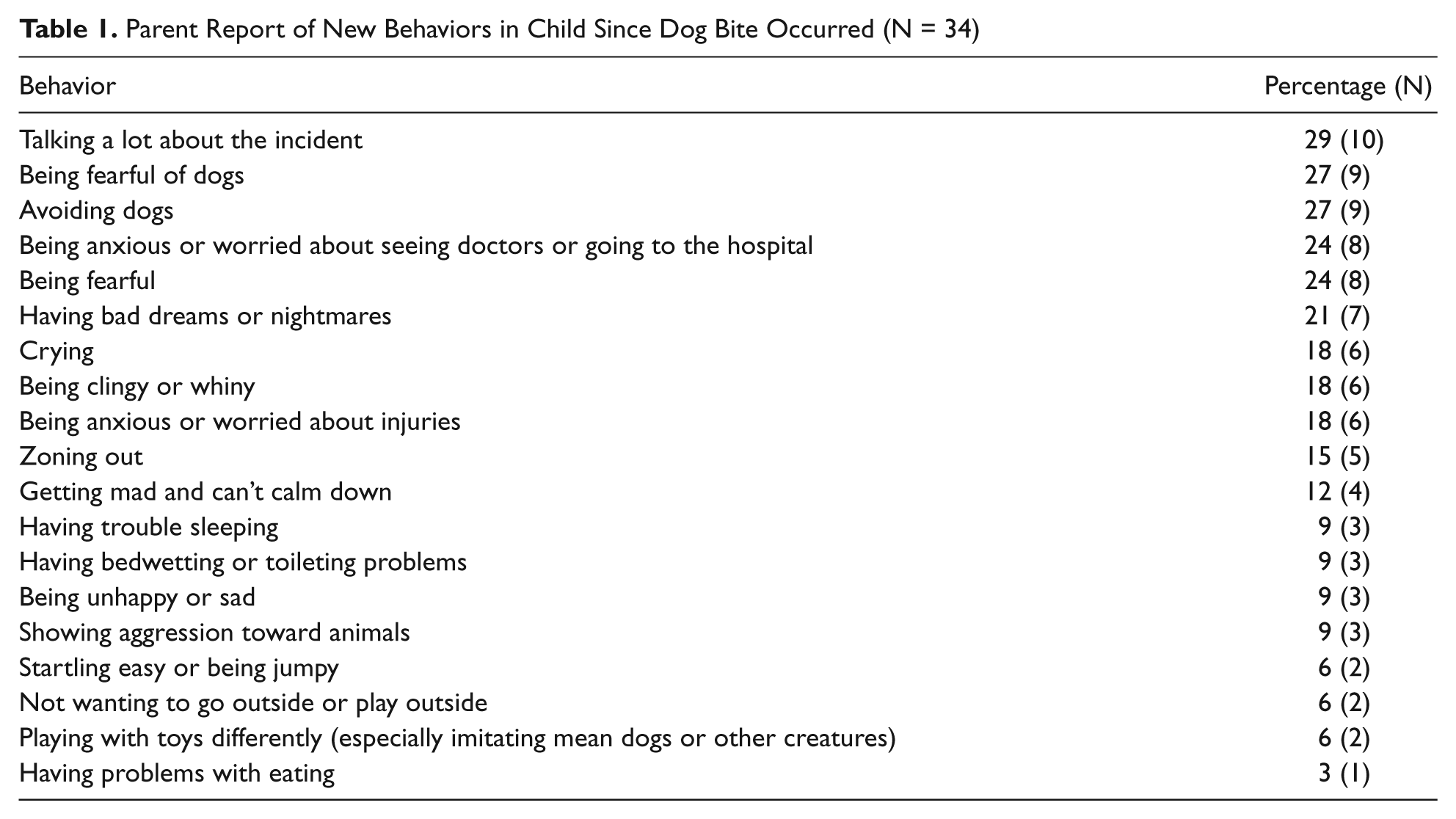
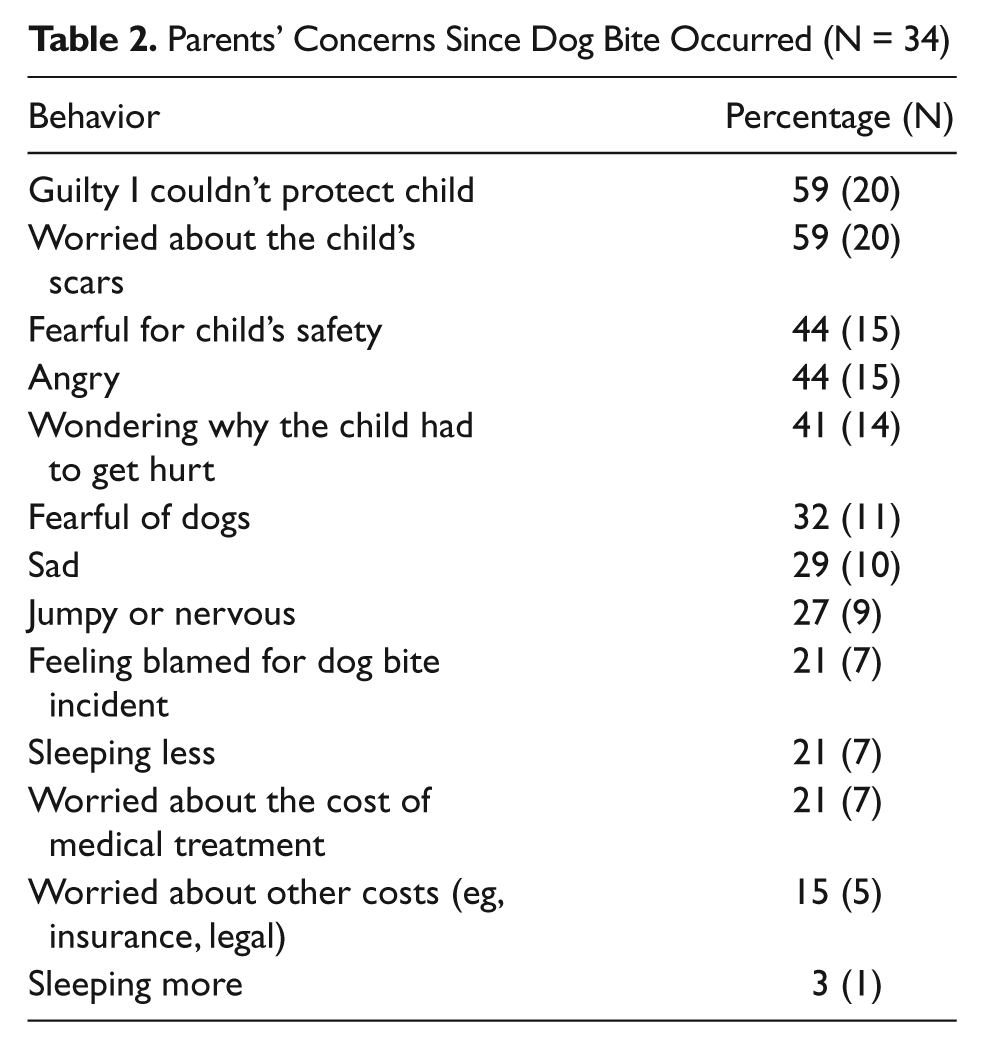
According to the parents, more than 70% of the child victims demonstrated at least 1 new concerning behavior since the dog bite. Breakdown of these behaviors by frequency are shown in Table 1. More than 85% of the parents also endorsed changes in their own concerns and feelings about themselves and their children since the dog bite (see Table 2). No children in this study received any psychological services. However, 50% of the parents endorsed the belief that children, in general, might benefit from interventions “to help my child with his/her fears.” In response to the question “When a child has been bitten, what are important times for families to get extra help?” 85% (29/34) said an important time would be “in the emergency department or doctor’s office,” 82% (28/34) said “when they get home and the child is starting to heal,” and 91% (31/34) said “after the child has healed but still has scars and fears.”
Parent Report of New Behaviors in Child Since Dog Bite Occurred (N = 34)
Parents’ Concerns Since Dog Bite Occurred (N = 34)
Forty-one percent of parent participants had at least 1 contact with other service agencies following the dog bite (Figure 2). Respondents identified the following as agencies that could offer additional assistance to families of dog bite victims: medical system (29%; 10/34), legal system (29%; 10/34), insurance companies (27%; 9/34), and animal control (18%; 6/34). Nearly three quarters of the parents (25/34) endorsed that families would benefit from education regarding dog bite prevention and how to be safe around dogs.
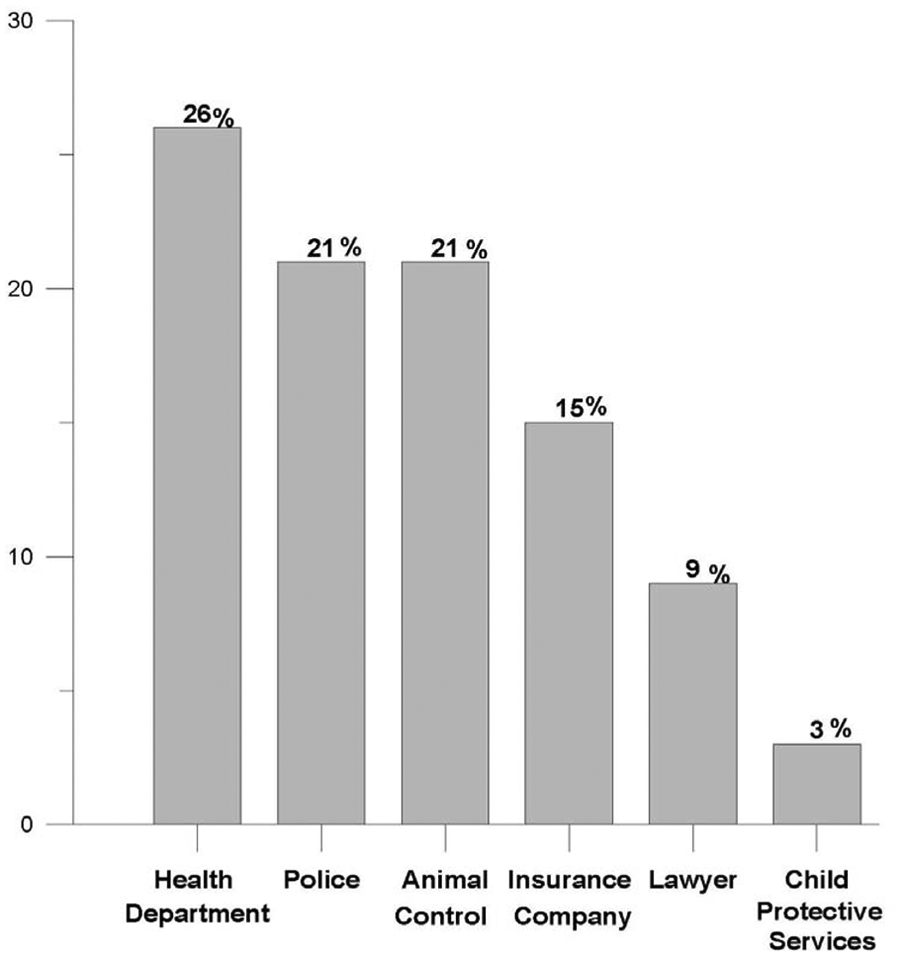
Contacts with other agencies after dog bite (N = 34)
Discussion
Typical treatment of dog bites focuses on wound care and preventive infectious measures. Parents in this study, however, reported that providing additional supportive care to dog bite victims and their families could be helpful. At least half of all parents identified psychological services as an important adjunct to the typical dog bite medical treatment. Although children enrolled did not have bite injuries that were severe enough to warrant hospitalization, the vast majority of parents endorsed concerning changes in their children’s behaviors and additional stress in their own lives since experiencing the dog bite. Specifically, more than a quarter of the parents described their children as avoiding dogs, being more fearful of dogs, and talking more about the incident; and nearly 60% of parents felt guilty about the dog bite and/or worried about their children’s scars.
In addition to psychological services, parents identified help with other services (such as the medical system and legal system) as an important part of the dog bite continuum of care. This need for assistance is not surprising, noting nearly half of all victims and parents had contact with at least one of these service agencies after the initial ED visit. Parents also recognized the need for increased prevention education to avoid these types of injuries in the first place, with nearly 75% stating this type of education would be beneficial.
The “appropriate times” to receive additional information about these services were reported consistently among parents as the ED or doctor’s office and/or when the child was home and starting to heal. Thus, we propose that the initial visit to a medical facility (ED or other care setting) for a dog bite injury can be an opportune time to address a range of potential parental concerns related to the event. One possible resource is to have a “Dog Bite Information Card” available to victims and families. This informational card could list facts about dog bite injuries and recovery, possible behavioral responses in both the child and parent, and contacts to obtain information on being safe around dogs (see sample template in the appendix). The card could be tailored to specific settings and include local resources for contacting mental health and other professionals. For children whose dog bite injuries are severe, however, it is important to consider making a referral to a qualified mental health professional to assess and treat possible posttraumatic stress responses that may significantly impair future functioning.
There were several limitations in this descriptive study. All reporting was obtained from victims’ caregivers and may not reflect the accuracy of actual events and behaviors. However, our goal was to report the parents’ perceptions of events and behaviors so we do not believe the data were compromised. Using a convenience sample limited our ability to capture all the victims of dog bites during this time period, and we were unable to enroll at least 1 victim whom we know was more severely injured. Yet a severely injured child would most likely have greater needs for ongoing supportive services. Finally, despite several attempts, we were unable to reach 32% of those who enrolled for follow-up as many of the phone numbers were no longer working, possibly skewing our sample toward a less mobile, more stable population. Nevertheless, it is impressive that in our sample, stressors and behavioral changes related to dog bites to children were a concern for most parents.
In conclusion, the majority of child dog bite victims and their parents in our study experienced changes in behavior and additional stress in their lives after the incident. Furthermore, these parents expressed a need for additional supportive services and a desire for prevention education related to this topic. Thus, we advocate that child dog bite victims and their parents may benefit from a continuum of care after these injuries and that dog bite prevention education should be an integral part of any child safety discussion with families.
Footnotes
Appendix
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The authors received no financial support for the research, authorship, and/or publication of this article.