
Abstract
Objective. To review the epidemiology and clinical course of invasive pneumococcal diseases of infants younger than 60 days. Study design. All Streptococcus pneumoniae strains isolated from blood and cerebrospinal fluid cultures of infants below the age of 60 days during the years 1999-2009 were included in this study. Demographic, clinical, and laboratory data were collected from medical records. Results. In all, 24 cases of pneumococcal invasive infections were identified. The primary diagnoses were bacteremia without a focus (n = 13), meningitis (n = 6), bacteremia with otitis media (n = 3), and joint infection with bacteremia (n = 2). Only one of the serotypes found is included in the heptavalent pneumococcal conjugated vaccine (PCV7). Conclusions. Streptococcus pneumoniae should be considered and treated empirically in infants with suspected invasive bacterial disease during the first 60 days of life. Routine vaccination with PCV7 in not expected to substantially reduce the incidence of invasive pneumococcal disease in Israeli infants of this age as a result of herd immunity.
Introduction
Streptococcus pneumoniae is considered an uncommon cause of invasive disease in neonates (1% to 11% of neonatal sepsis cases).1-5 Most of the literature concerning pneumococcal disease in this age group consists of case reports or small series describing fulminant early-onset sepsis associated with high morbidity and mortality.6-10 Factors associated with a high-risk for pneumococcal infection are prematurity, low birth weight, maternal pneumococcal infection, and prolonged rupture of membranes.6-11 However, a large case series and review of the literature did not find an association with these risk factors. 12
The heptavalent pneumococcal conjugate vaccine (PCV7) became part of the routine vaccination schedule in Israel from May 2009. PCV7 is recommended for all children aged 2 to 23 months or for children aged 24 to 59 months who are at increased risk for pneumococcal disease. Routine use of the vaccine has had a substantial impact on the incidence of pneumococcal disease in children in the United States, and disease burden has decreased in infants younger than 2 years.7,13,14 Infants younger than 2 months, who are below the age of vaccination with PCV7, may benefit from universal vaccination as a result of herd immunity. 15 However, it is yet to be shown whether routine use of PCV7 will decrease disease burden in this age-group as well. In Israel, the serotype coverage of PCV7 for invasive pneumococcal disease is expected to be about 50%, 16 but there is no published data regarding the serotypes causing invasive pneumococcal disease in young infants.
The aim of this study was to characterize the epidemiology and clinical course of invasive pneumococcal diseases in infants younger than 2 months in a single medical center in Israel.
Methods
The study was performed in Shaare Zedek Medical Center, a 550-bed university-affiliated general hospital. The pediatric department contains 40 beds, 3 of which are for intensive care patients. The annual pediatric admission rate ranged from approximately 3000 to more than 4000 patients per annum over the 10-year study period.
All S pneumoniae strains isolated from blood or cerebrospinal fluid cultures during the years from 1999 to 2009 were reviewed using the computerized database of our medical center. Demographic, clinical, and laboratory data were collected from the medical records of all infants younger than 60 days. Serotyping of all isolates was performed by the National Reference Laboratory of the Israeli Health Ministry using the Quellung reaction. Bacterial susceptibility testing for penicillin was performed at Shaare Zedek Medical Center’s microbiology laboratory using the AB Biodisk E-test (Bio-Merieux Sa, Marcy L’etoile, France) on Muller-Hinton plates with 5% sheep blood.
Statistical Methods
Statistical analysis was done using SPSS version 12. Qualitative variants were compared by Fisher’s exact test. Quantitative variables were compared by t test.
Results
Demographic Information
During the period 1999-2009 there were 24 cases of invasive pneumococcal disease in infants younger than 60 days. This number represented 6% (24/412) of total pneumococcal bacteremia and meningitis cases in children up to 16 years old during the study period. S pneumoniae accounted for 9% of all bacteremia and meningitis cases in infants up to 2 months old (Figure 1).
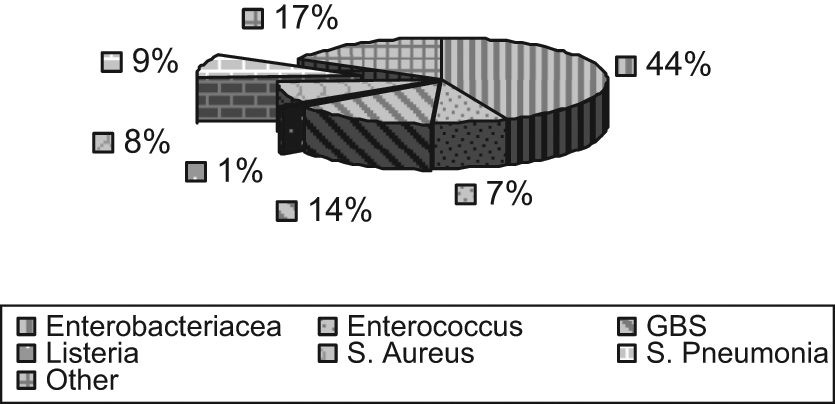
Bacteremia and meningitis etiology in infants younger than 60 days
The number of invasive pneumococcal infections in infants younger than 2 months per year during 1999-2007 ranged from 1 to 3 cases. In 2008 and 2009 there were 4 and 5 cases of pneumococcal invasive disease, respectively. The median age of infected infants was 38.5 days (±18.5 days). Onset of symptoms before 72 hours of life (“early onset”) occurred in only 4 cases (17% of study cases). In all, 63% of the patients were male. A total of 87% of the infants were born at gestational age of ≥38 weeks. The mean birth weight was 3.210 kg (±426 g). In total, 21 of the infants had at least one older sibling (range 1-11), and we cannot account for siblings regarding the other 3 infants. Four of the infants were delivered by cesarean section, all of whom had late-onset disease and were older than 30 days at disease onset.
Demographic and clinical data of the 24 infants with pneumococcal bacteremia are presented in Table 1.
Demographic, Clinical, and Laboratory Data of Infants <60 Days With Infection Caused by Streptococcus pneumoniae
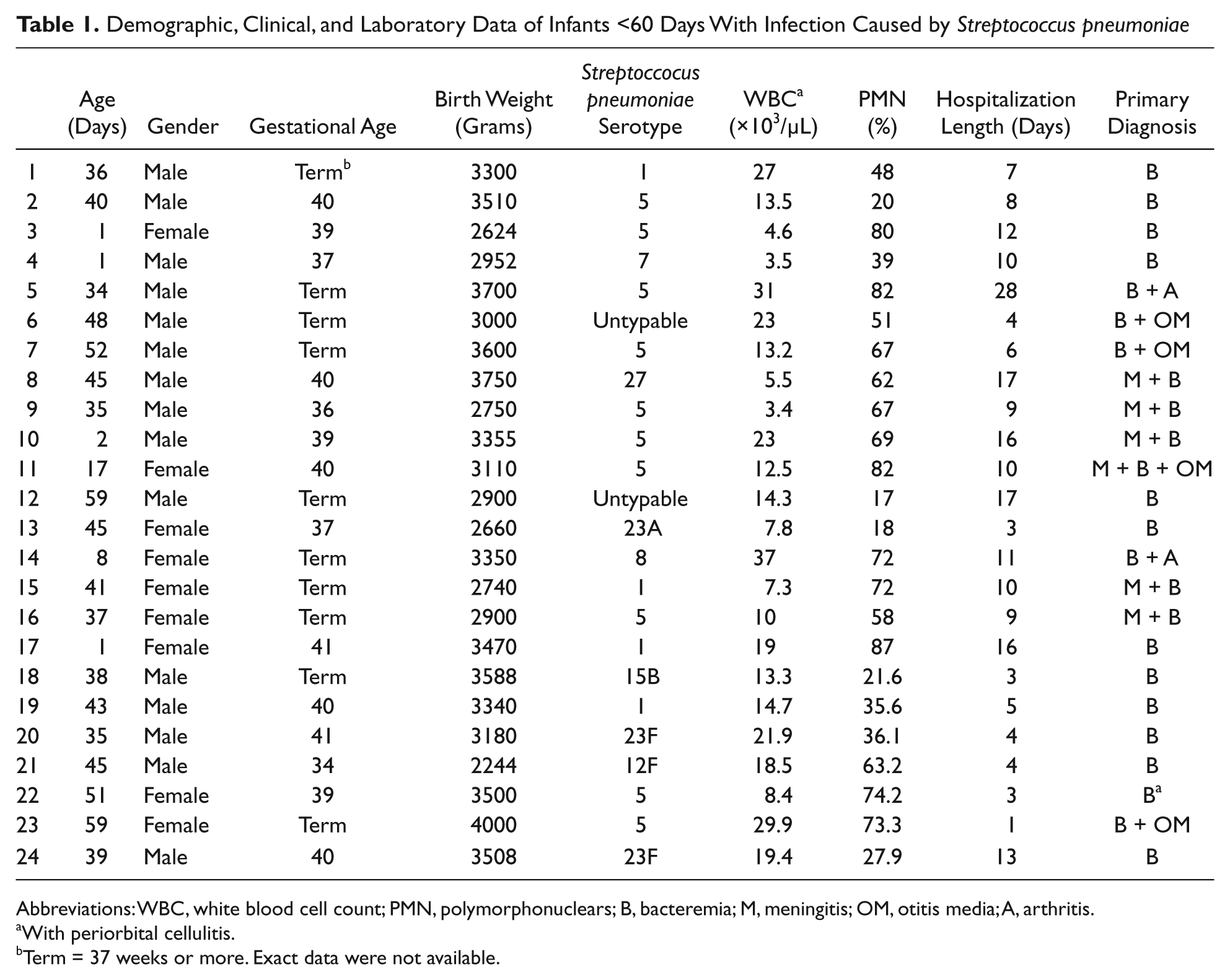
Abbreviations: WBC, white blood cell count; PMN, polymorphonuclears; B, bacteremia; M, meningitis; OM, otitis media; A, arthritis.
With periorbital cellulitis.
Term = 37 weeks or more. Exact data were not available.
Clinical Presentation and Outcome
Bacteremia without focus (n = 13) and meningitis (n = 6) were the most common diagnoses. All cases of otitis media were bilateral. There was only 1 fatal case in a term infant with trisomy 21 that was hospitalized in the neonatal intensive care unit after birth for respiratory distress. Pneumococcal sepsis and meningitis was diagnosed during the second day of life. Thereafter, the infant deteriorated to multiorgan failure with mortality on the 16th day post birth. Eight infants were admitted to the intensive care units, 6 of whom needed mechanical ventilation and 2 required treatment with inotropic agents.
Pneumococcal Serotypes and Antibiotic Susceptibility
The most common serotypes causing invasive disease were 5 (n = 10) and 1 (n = 4) as shown in Table 1. There was no correlation between the primary diagnosis and the infecting serotype. In all, 87% of pneumococcal isolates in our study were fully penicillin susceptible (minimum inhibitory concentration [MIC] < 0.1), and the rest had intermediate susceptibility (1 ≥ MIC > 0.1). All isolates were ceftriaxone susceptible (MIC < 0.5).
Discussion
To the best of our knowledge, this study presents the largest series of infantile invasive pneumococcal infections in a single medical center. We found that S pneumoniae is not an uncommon pathogen in this age-group and accounted for 9% of bacteremia and meningitis cases.
A large case series was published by Hoffman et al 17 using data from the US Pediatric Multicenter Pneumococcal Surveillance Group. They described 21 children, most of whom were full-term babies without known risk factors. In contrast with older studies that found mortality rate of up to 60% and high rate of early-onset pneumococcal sepsis,11,12,18,19 Hoffman et al found a relatively low mortality rate (14.3%), and only 14% of early-onset disease, similar to the results of our study. We found an even lower mortality rate, and the only fatal case occurred in early-onset disease. Of note, 74% of the pneumococcal serotypes causing invasive disease in the series of Hoffman et al are included in the PCV7, whereas in our study only one of the infecting strains causing 2 invasive cases (8%) would be covered by the heptavalent vaccine.
The conjugated pneumococcal vaccine PCV7 includes the following serotypes: 4, 6B, 9V, 14, 18C, 19F, and 23F and the vaccine-related serotypes are 6A, 9A, 9L, 9N, 18A, 18B, 18F, 19B, 19C, 23A, and 23B. Therefore, only serotype 23F found in 2 of our patients is included in PCV7 or the related serotypes. Serotypes 1 and 5 were the most common serotypes causing disease in our study. An Israeli study that was done before the introduction of the PCV7 anticipated that the addition of serotypes 1 and 5, included in both PCV10 and PCV13, will increase the PCV7 overall serotype coverage for invasive pneumococcal disease by 29% and 11% in Bedouin and Jewish children, respectively. 19
Based on a review of 13 studies, as early as 1995, the global serotype distribution was categorized into “developed” and “developing” country patterns, with serotypes 1 and 5 proposed to reflect “developing” country serotypes. However, a major factor influencing the perceived importance of serotypes 1 and 5 is the precise pediatric age group studied. For example, a German study revealed that the serotypes represented in the heptavalent vaccine accounted for 70% of invasive pneumococcal disease in the 6- to 24-month age range, but only for 30% to 40% of invasive serotypes causing disease in <6-month-olds or >5-year-olds. In contrast, serotypes represented in a hypothetical 9-valent vaccine (also containing serotypes 1 and 5) increased vaccine coverage to 70% to 80% in those age ranges. 20
Another German study from 2010, 21 found similarly, that the serotype coverage for the PCV7 to be only 36.8% for infants younger than 60 days with the new conjugate vaccines (10- and 13-valent) increasing the coverage up to 80%. Their leading serotypes were 7F, 1, and 14. The serotype distribution in this age-group differed considerably from that of older infants who were vaccinated with the PCV7. In contrast to our study, in which all strains were susceptible to penicillin, Imohl et al 21 found resistance in 3.1% of pneumococcal meningitis cases.
In our medical center, even with the introduction of the 13-valent pneumococcal conjugated vaccine, which includes the most common serotypes found in our study,1,5 the vaccine coverage will still be only 67% for invasive pneumococcal infections in infants younger than 2 months. Several other studies found that neonatal disease tends to occur with nonvaccine serotypes.11,12,16
We found no case of pneumonia, but it is possible that neonatal pneumonia was underdiagnosed, as chest X-ray is not performed routinely in febrile infants in our medical center, unless respiratory signs or symptoms are present.
Neonatal pneumococcal early onset disease (≤72 hours after birth) is thought to be due to maternal vertical transmission. S pneumoniae is uncommon in the vaginal flora6,10,22 but rarely can even cause puerperal sepsis. The rarity of vaginal carriage suggests a high invasion to colonization ratio. Most of our cases occurred later than 72 hours post birth, as has been previously described. 16 The mechanism of late-onset infection can be either related to colonization occurring in the passage through the maternal birth canal, or to acquisition of the bacteria from older siblings. In all cases where data were available in this study, the patients had older siblings. This fact supports the theory that, as in older infants, the mechanism of disease beyond the first week of life is horizontal acquisition of the pathogen followed by colonization in the nasopharynx or middle ear fluid, and secondary bacteremia or meningitis as a later event. Moreover, it is interesting to note that all 4 infants who were delivered by caesarian section had late-onset disease occurring more than 30 days after birth. This too is in agreement with the assumption that the mode of transmission could not be vertical in these cases.
In total, 87% of the pneumococcal isolates in our study were fully susceptible to penicillin (MIC < 0.1). The rest had intermediate susceptibility. The empiric antibiotic regimen for suspected neonatal sepsis in our hospital includes administration of high-dose ampicillin and gentamicin, or ampicillin and cefotaxime if meningitis is suspected. This regimen is adequate for pneumococcal invasive infections in our medical center but may not be adequate in centers where penicillin resistance rates are higher.
Conclusions
Pneumococcal infection should be considered for and treated empirically in every infant with a suspected invasive bacterial infection. In medical centers with a high percentage of penicillin nonsusceptible pneumococcal strains, the empiric antibiotic regimen for neonatal sepsis should be modified to cover those strains. Routine vaccination with PCV7 might not substantially reduce pneumococcal morbidity in infants younger than 60 days, in Israel.
Footnotes
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author received no financial support for the research, authorship, and/or publication of this article.