
Abstract

Case Report
An 18-year-old previously healthy overweight Hispanic male was referred to our gastroenterology clinics in a Boston teaching hospital during the month of November with a 1-week history of fatigue and a 2-day history of high-grade fever, chills, malaise, jaundice, joint pain, loss of appetite, and noticeably darker urine. He denied abdominal pain, chest/retrosternal pain, vomiting or diarrhea, cough, rhinorrhea, or rash. Approximately 1 month prior to the visit, he went to a camp in New Hampshire with his friends and stayed in a cabin over the weekend. He could not recall any intakes of unusual food or drinking water. His past medical history was noncontributory—no history of liver, pancreas or gallbladder disease, liver failure, or liver transplant. He drank 2 to 3 cans of beer per month but recently binged. He denied illicit or intravenous drug use, tobacco smoking, or history of blood transfusions. He could not recall recent animal contacts or exposure to jaundiced persons. There was a family history of renal stones and hypertension in his father, otherwise unremarkable for liver diseases.
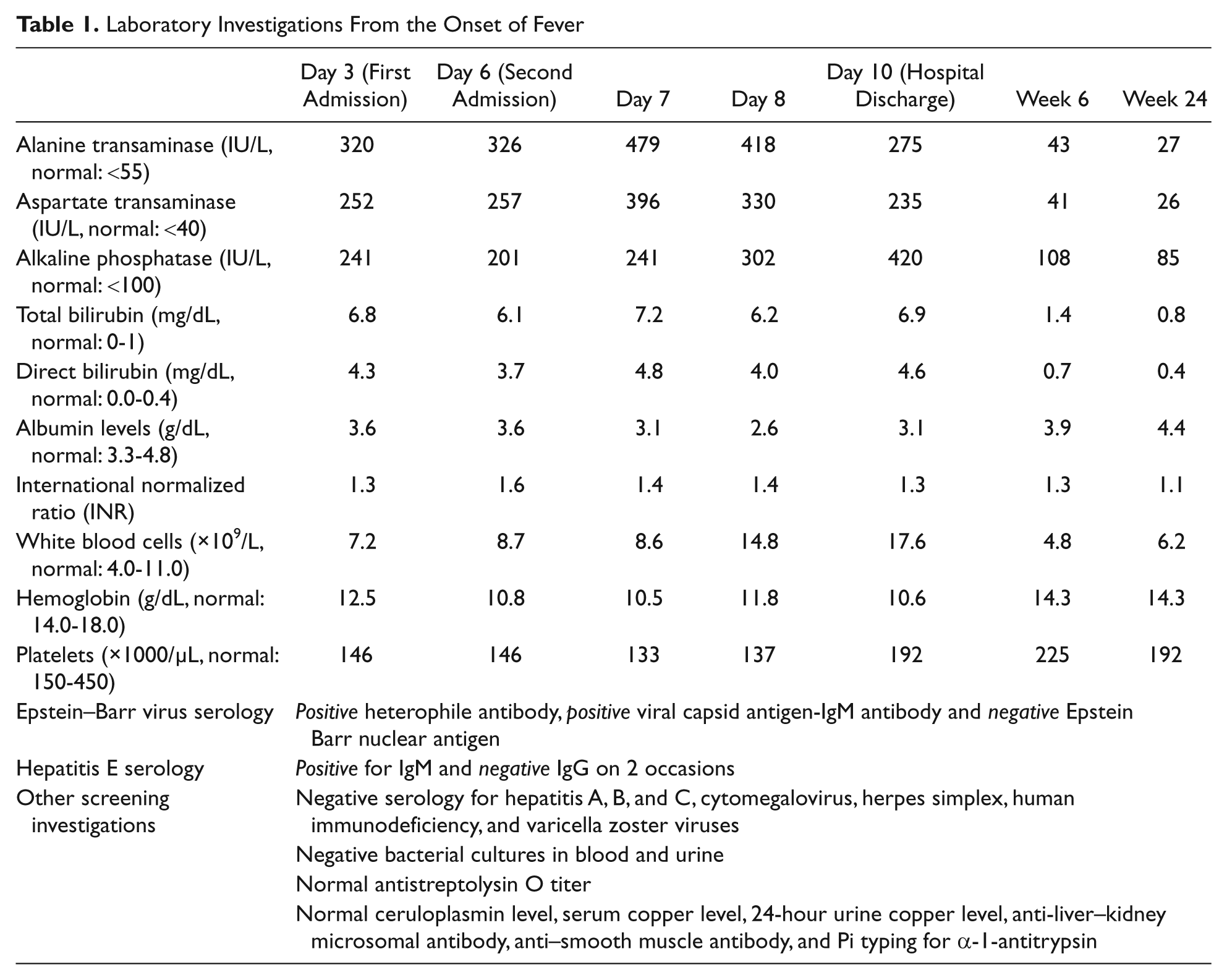
His physical examination showed a temperature of 100°F and orthostatic hypotension without apparent distress. His body mass index was 31.5. His skin was jaundiced and noted to have acanthosis nigrigans around his nuchal region. There was tonsillar hypertrophy without exudates. Cervical lymphadenopathy with mild tenderness was documented. His abdominal examination was significant for right upper quadrant tenderness and splenomegaly. No stigmata of chronic liver disease were noted on examination. There was no clubbing, bruising, or bleeding. Laboratory investigations during the course of illness are shown in the Table 1. Given the positive viral capsid antigen-IgM antibody and negative Epstein Barr nuclear antigen with elevated transaminases, our patient was initially diagnosed with Epstein–Barr virus (EBV)–associated hepatitis. His viral hepatitis A, hepatitis B, and hepatitis C serology were negative. Abdominal ultrasonography showed an enlarged spleen at 16 cm with a normal appearing liver, and there was no intrahepatic bile duct dilatation. Hepatic venous pressure gradient and common bile duct size were normal.
Laboratory Investigations From the Onset of Fever
Hospital Course
Given his fever, extreme fatigue, malaise, jaundice, and orthostatic hypotension, he was admitted for an overnight observation and an intravenous hydration. He was discharged the next day with improving clinical status. Approximately 48 hours since discharge, he became more fatigued and lethargic with altered mental status necessitating readmission to the pediatric intensive care unit for the management of acute liver failure. He had an albumin of 3.1 mg/dL with an elevated prothrombin time. During this hospital admission, he had worsening mental status, cholestasis, and anemia with a reticulocyte count of 4.2% and a positive Coombs’ test suggestive of immune-mediated hemolysis. Differential diagnosis was broadened given his aforementioned rapidly worsening clinical and laboratory features (see laboratory results during the illness in Table 1) in particular, the aggressive hemolysis. Hepatitis E IgM and IgG serology were sent. Subsequently, a positive hepatitis E IgM with a negative hepatitis E IgG serology suggested an acute HEV infection.
He was conservatively managed; and at discharge, 5 days later, he had improved clinical status and liver function. Six months later, his liver enzymes, billirubin and liver function returned to normal with complete recovery from his symptoms. He was enrolled in a weight loss and exercise program for obesity to prevent further liver injury.
Final Diagnosis
Concomitant infections with hepatitis E and EBVs causing acute liver failure.
Discussion
We reported a previously healthy overweight adolescent male with concomitant infections with hepatitis E and EBVs causing acute cholestatic hepatitis, significant hemolysis, and subsequent liver failure. The purpose of this report is to highlight the importance of considering hepatitis E virus (HEV) as a possible pathogen when evaluating acute liver failure in children and adolescents even in developed countries such as the United States.
Hepatitis E virus is an enterically transmitted hepatotropic single-stranded RNA virus that was first described during an outbreak in New Delhi, India, in 1955 but formally recognized 4 decades later. HEV is a common cause of acute hepatitis in endemic areas such as Africa, Asia, and Mexico. 1 Until recently, HEV has been recognized as a cause of viral hepatitis among travelers to endemic countries. 2 Infectious outbreaks can be either epidemic or sporadic. To date, 4 genotypes have been commonly described with different geographic distributions, patterns of outbreak, and potential reservoirs. Genotype 1 and 2 strains mainly infect humans, are associated with a waterborne transmission, and cause epidemics especially in the aforementioned hyperendemic areas; whereas genotype 3 and 4 strains sporadically infect humans worldwide, including those in developed countries, and are thought to be transmitted zoonotically. These 2 genotypes also infect other animals (eg, swine, boars, and deer).3,4 Ingestion of contaminated water or raw and undercooked foods while travelling to endemic areas remains the most common mode of transmission. HEV may also be transmitted by blood transfusions or person-to-person contacts.1,2 The incubation period ranges from 15 to 40 days. 5 Therefore, a detailed history regarding sources of drinking water, intake of uncooked food, previous history of blood transfusion, and contact with jaundiced persons should be carefully obtained to aid in a diagnosis. However, more than half of the HEV-infected patients may be nontravelers who are not exposed to the aforesaid risk factors. 6 Additionally, the National Health and Nutrition Examination Survey (1988-1994) also found that exposure to HEV is rather common in the United States, with an asymptomatic anti-HEV IgG seroprevalence of 21%, suggestive of potential autochthonous infections. 7
Generally, infected patients remain asymptomatic or mildly symptomatic with low-grade fever and mild jaundice that spontaneously resolves with a mortality rate <3% in the general population.3,5 Clinical attack rates are highest among persons aged 10 to 40 years. Symptomatic cases are uncommonly reported in developed countries, especially among the pediatric population. Furthermore, limited data are available in children and adolescents with HEV-caused acute liver failure. Cases of hepatitis E are also clinically indistinguishable from other hepatotropic viruses, which manifest with malaise, anorexia, fever, icterus, hepatomegaly, pruritus with elevated bilirubin, and markedly elevated liver enzymes. Hepatomegaly is common with occasional painless lymphadenopathy. Spontaneous resolution of the abnormal liver enzymes usually occurs within 6 weeks after the onset of illness, 5 however, severe hepatitis leading to fulminant liver failure occurs. Diagnosis can be confirmed by testing for an antibody to hepatitis E or the presence of HEV RNA. 4 More than 90% of HEV-infected patients have detectable HEV IgM in the first 2 weeks after the disease onset, which makes serology suitable for the diagnosis of acute infection. 8
Extrahepatic manifestations, such as thrombocytopenia, hemolysis, glomerulonephritis, or pancreatitis, have been published in case reports and small case series. 5 Our patient developed thrombocytopenia and immune-mediate (ie, Coombs positive) hemolysis during the course of illness along with hepatic decompensation, which led to further investigations including HEV serology. As the disease is self-limited, the current treatment for acute HEV hepatitis is essentially supportive. Moreover, even with tremendous efforts on HEV vaccine development, no vaccine is currently approved for preventing HEV.
Our patient also tested positive for EBV at the initial presentation. In most adolescents, EBV-associated hepatitis commonly presents (~80% to 90%) with asymptomatic mild elevation of liver enzymes up to 2 to 3 times the upper limit of normal and usually resolves in 3 months. 9 Cholestatic hepatitis with mildly elevated bilirubin levels may occur but acute liver failure has been rarely described. Therefore, broadening the differential diagnosis is crucial in patients with acute liver failure with unclear etiology or patients who present with atypical clinical presentations.
We would like to emphasize the potential need to evaluate for HEV in the setting of rapidly progressive acute liver failure and hemolysis, even in the United States. In addition, concomitant multiple hepatotropic infections causing acute hepatitis have been reported in children. 10 Therefore, an evaluation for multiple pathogens or etiologies may be warranted in patients with rapid hepatic decompensation.
Conclusion
In summary, given the high seroprevalence of HEV infection but infrequently reported symptomatic patients or liver failure in the US children and adolescents, we suggest the importance of considering HEV as a possible pathogen, even in the developed countries without pertinent travel history to an endemic area, when evaluating a child with rapid hepatic decompensation. Furthermore, given that this virus may produce disease as either a single or concomitant infection, HEV should be considered in the evaluation for acute liver failure when the etiology remains unclear.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.