
Abstract

Patient Report
This 9-day-old African American female was brought to the emergency department by her mother and father with complaints of constipation for 1 day and decreased wet diapers. Bowel movements and urinary habits prior to this were normal. The parents also noted that the baby was irritable and felt warm the prior evening. She had her first well baby checkup the day before and was noted to be afebrile with a normal physical exam.
The patient was born at term via normal spontaneous vaginal delivery weighing 3.03 kg (6 lbs 11 oz) and was discharged home the day after delivery. There was no meconium staining at birth. The maternal labs were negative, including group B streptococcus cultures.
On physical exam, she was judged to have no acute distress. Her rectal temperature was 102.0°F, heart rate 195 beats/min, respiratory rate 55 breaths/min, and oxygen saturation 99% on room air. She weighed 3.7 kg (50th percentile), was 53.3 cm in length (90th percentile), and had a head circumference of 34 cm (35th percentile). She was noted to have positive Brudzinski and Kernig signs. The anterior fontanel was slightly convex and pulsating. The remainder of the physical exam was unremarkable.
Initial laboratory studies included a WBC (white blood cells) count of 7560/mm3 (normal 5000-21 000) with a differential of 45% neutrophils (50% to 70%), 20% bands (0% to 6%), and 33% lymphocytes (25% to 40%). She had a hemoglobin and hematocrit of 15.2 g/dL (11.0-18.0 g/dL) and 42.3% (31.0% to 55.0%), respectively. Her platelet count was 201 000/mm3 (150-350 000).
A lumbar puncture was performed, which produced xanthochromic cerebrospinal fluid (CSF) with a WBC count of 301 cells/mm3 (0-30) and RBC (red blood cells) count of 780 cells/mm3. The Gram stain showed many polymorphonuclear leukocytes and many Gram-positive cocci in pairs.
Blood, urine, and CSF cultures were obtained, and the patient was placed on ampicillin, cefotaxime, and vancomycin. A cranial ultrasound showed evidence of neither hemorrhage nor hydrocephalus. The next day CSF cultures were reported to contain alpha-hemolytic streptococci subsequently identified as Streptococcus bovis susceptible to numerous antibiotics with an minimum inhibitory concentration for penicillin <0.01 µg/mL. Antibiotics were deescalated to monotherapy with penicillin G, which was continued to complete 21 days of antimicrobial therapy. She was afebrile and feeding normally after 72 hours of antibiotics but the Kernig sign remained positive for 4 days and the Brudzinski sign for 6 days. Physical exam, head ultrasound, and hearing testing were normal at 21 days when she was discharged to outpatient follow-up.
Diagnosis
Meningitis in a neonate caused by Streptococcus bovis.
Discussion
The incidence of bacterial meningitis is highest during the first month of life, 1 reported between 0.25 and 0.32 cases per 1000 live births, depending on inclusion criteria.2-4 Worldwide, acute bacterial meningitis is 1 of the 10 leading causes of infection-related death. Morbidity is high, with 30% to 50% of survivors having some form of permanent neurological disability.5,6 Risk factors for neonatal meningitis include low birth weight (<2500 g), preterm birth (<37 weeks gestation), maternal colonization with group B Streptococcus, premature rupture of membranes, septic or traumatic delivery, fetal hypoxia, maternal peripartum infection, galactosemia, and urinary tract abnormalities. Mortality rates are highest following infection with enteric Gram-negative bacilli and Streptococcus pneumoniae, lower with Lancefield group B streptococcus, and lower still with Listeria and other Gram-positive bacteria. 4
For neonates with meningitis, the most consistent initial finding is temperature instability. Term infants tend to present more commonly with fever (rectal temperature >38°C), whereas preterm infants are more likely to present with hypothermia (rectal temperature < 36°C). In one large series, 62% of neonates presented with temperature abnormalities, 52% had lethargy or irritability, 48% had anorexia or vomiting, 31% had convulsions, 28% had a bulging fontanelle, and finally 16% presented with nuchal rigidity. 3 Early diagnosis is critical for optimal outcome as mortality increases with progression of disease. A recent study of children admitted to the hospital for bacterial meningitis found that there is an increased risk of death with patients who have a Glasgow Coma Score (GCS) of 10-12, and an even higher risk of death in patients admitted with a GCS of 6 and below. 3
The obvious first step in management of suspected meningitis is to obtain a CSF sample for culture, Gram stain, WBC count, and glucose and protein concentrations. However, the initial CSF parameters may not always suggest CNS (central nervous system) infection. In a study of CSF obtained from 9111 infants, of 95 patients with culture-proven bacterial meningitis, 12 (13%) had normal CSF parameters. 3 Therefore, all CSF specimens must be cultured in suspected meningitis. Most experts also recommend that unless the patient is clinically unstable, a baseline cranial ultrasound be performed if there is clinical suspicion of bacterial meningitis. If there are further complications during the patient’s clinical course, a second study should be considered.
Complications of meningitis can be remembered with the mnemonic HACTIVE (hydrocephalus, abscess, cerebritis, thrombosis, infarct, ventriculitis, empyema). If any signs of these processes are identified, the patient should have an immediate magnetic resonance image taken. 5 Magnetic resonance imaging is preferred over computed tomography because it uses no ionizing radiation, has better soft tissue resolution, and provides a better examination of the posterior fossa.5,6
Streptococcus bovis has been documented as a causative organism in neonatal bacteremia and meningitis, albeit a rare one. 7 Fortunately, there is a lower mortality associated with S bovis meningitis compared with other meningeal infections. 8 This organism is most noted for causing endocarditis in adults and its correlation with colonic neoplasms. From 1975 to 2000, only 6 cases of nonenterococcal group D streptococcus meningitis had been reported in the English literature, although it is believed that prior cases may have been mislabeled as enterococci or streptococcus viridans. 8 A search of the English literature for “Streptococcus bovis meningitis” on PubMed revealed 8 infant cases from 2001 to 2011 (Table 1). Every case listed S bovis type II as the cause of the child’s meningitis. An additional paper was found that included 4 patients who developed S bovis meningitis from 1998 to 2004; however, it was not possible to discern in what year the infants contracted the disease, nor were any of the laboratory results or histories/outcomes present. 9 Being a rare cause of meningitis raises the question of the source. One study of 14 adults with S bovis meningitis, 10 of those patients had prior gastrointestinal disease.7,10 The only gastrointestinal symptom in this patient had been constipation for 1 day. In another report of a neonate with S bovis meningitis, vaginal and rectal cultures were obtained from the patient’s mother, which grew out the same organism. 11
Documented infant Streptococcus bovis meningitis cases: 2001-2011
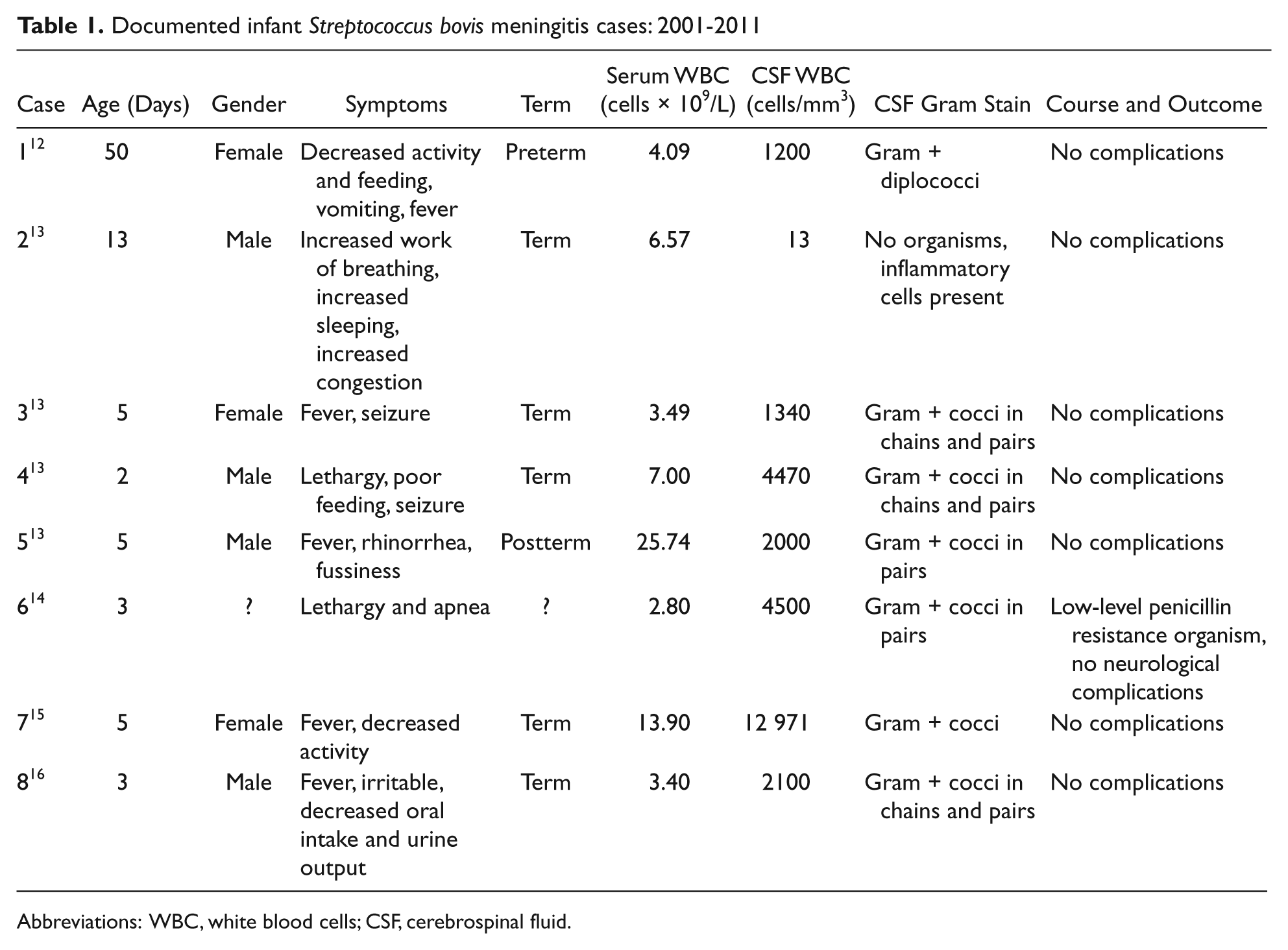
Abbreviations: WBC, white blood cells; CSF, cerebrospinal fluid.
Streptococcus bovis has some similar phenotypical characteristics to bacteria such as Enteroccoci and Streptococcus viridans. 16 However, S bovis can be adequately treated with penicillin G, whereas the other organisms require the addition of an aminoglycoside or the use of vancomycin. 8 S bovis can be distinguished from enterococci by its growth on bile esculin and at 45°C, whereas it does not grow at 10°C or in 6.5% NaCl. 17
Streptococcus bovis is a catalase negative, nonsporulating, nonmotile, Gram-positive, nonenterococcal group D streptococcus.18,19 It usually forms small and nonhemolytic colonies on blood agar, and usually expresses the Lancefield group D antigen.8,19 Several species are included in the bovis group, including Streptococcus bovis, Streptococcus agalactolyticus, Streptococcus infantarius, and Streptococcus equinus. 18 S bovis can be further subdivided into biotype I (typical) and biotype II (variant). 16 The typical strains are able to ferment mannitol and produce glucan whereas the variant strains are unable to do either. The biotype II strains can be further categorized into biotypes II/1 and II/2 by the ability of II/2 to produce beta-galactosidase and beta-glucoronidase and ferment trehalose but not glycogen. 16
Preliminary studies from the genotyping of S bovis isolates from adult and pediatric patients have suggested that specific serotypes are associated with different clinical infections. It is well documented that adult bacteremia infections with S bovis associated with colonic malignancy are more likely to be type I (71%), which is also the serotype that causes 90% of S bovis bacterial endocarditis. 9 In contrast, neonatal infections (sepsis and meningitis) caused by S bovis that were biotyped all reported infection due to type II. In that same group, of those that had further genotypical testing, all were of the variant type II/2. 16
In regards to specific meningitis infections caused by S bovis, one study reported 2 neonates with type II/2 and 3 of 4 adults also infected with type II/2. It appears that adult bacteremic infections are caused by type I and that meningitis in both the adult and pediatric populations are caused by type II/2. 16
Footnotes
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The authors received no financial support for the research, authorship, and/or publication of this article.