
Abstract
Background. Few population-based studies have assessed health outcomes and health care access and use among youth in the US Commonwealth of Puerto Rico. Methods. Data are from an island population–based sample of 337 youth, 10 to 17 years old, who participated in the Asthma, Depression, and Anxiety in Puerto Rican Youth Study. In-person interviews with youth and caregivers assessed self-rated physical and mental health, weight status, diagnosed health conditions, and health care access and use. Results. Island Puerto Rican youth report slightly worse physical and mental health than mainland youth. Puerto Rican youth have high rates of asthma, headaches, and stomachaches. Also, 6 in 10 island youth use public health insurance, and 1 in 3 regularly receive care at the emergency department. Conclusions. Island Puerto Rican youth are at a health disadvantage compared with mainland youth. Public health research is needed to fully understand and combat health challenges among Puerto Rican youth.
Introduction
In contrast to children and adolescents living in the continental United States, relatively little is known about the health of youth in the US Commonwealth of Puerto Rico. The primary data source regarding the health behaviors and outcomes of island Puerto Rican children and adolescents has been the Youth Risk Behavior Surveillance System (YRBSS), which samples high school youth in Puerto Rico in about half of its survey years. Data from 2005, the most recent YRBSS survey year that included Puerto Rico, paint different pictures of the health behaviors and outcomes of Puerto Rican youth compared with their US peers. 1 For example, YRBSS indicates that high school youth in Puerto Rico are less likely than those in the United States to be physically active for an hour or more on at least 5 days per week (20.8% vs 35.8%). 1 One reason island youth are less active than mainland youth may be that they are much more likely to have been diagnosed with asthma (31.5% vs 17.1%), although the reasons for this higher asthma prevalence remain under investigation.1-4
One of the challenges in gaining a complete understanding of child and adolescent health in Puerto Rico using the YRBSS is that data are only collected on a limited range of health topics, and the survey does not collect data among children who are younger than high school age. Additionally, the YRBSS is a school-based sample that includes only students currently enrolled in a public high school. Thus, it is difficult to determine how design aspects of the YRBSS affect the generalizability of its findings. For example, a number of population-based studies conducted among children and adolescents on the island have found results that contrast with those of the YRBSS. One area of discrepancy is mental health. Findings from the YRBSS suggest that 32.1% of Puerto Rican youth reported feeling sad or hopeless for 2 weeks or more at some point in the previous year, compared with 28.5% of those in the United States. 1 Similarly, the YRBSS found that 14.8% of island youth reported engaging in suicidal behavior in the previous year, compared with just 8.4% of mainland youth. 1 These findings contradict those of several population-based studies that have found that rates of psychiatric disorders and suicidal behavior do not differ between Puerto Rican youth and those in the United States.5-8 The Boricua Youth Study, for instance, found no difference in children’s depressive or anxiety disorders between population-based samples of island youth and youth of Puerto Rican descent in the South Bronx. 8
Although a number of population-based studies have been conducted among youth in Puerto Rico, they have investigated only specific health issues, primarily mental health and asthma.4,7-9 The dearth of population-based data regarding the general health and well-being of island Puerto Rican children is concerning because studies among adults have found that island Puerto Ricans have significantly poorer health outcomes than other Latino subgroups as well as the overall US population. 10 One cause of the health disadvantage faced by island Puerto Ricans may be poverty. Data from the 2007 American Community Survey suggest that the median household income in Puerto Rico is $18 184, compared with $49 807 in the US mainland. 11 In fact, median household income in Puerto Rico is about half that in Mississippi, the lowest-income state in the United States.
The socioeconomic disadvantage of Puerto Rican children and adolescents relative to their mainland counterparts may contribute to disparities in access and use of health care services and greater susceptibility to negative health outcomes. To our knowledge, few studies have examined health care access and use among Puerto Rican youth. One exception is the Rhode Island-Puerto Rico Asthma Center Study (RIPRAC); however, RIPRAC recruited convenience samples of participants from local clinics and other organizations rather than from a population-based sample. 9 Furthermore, RIPRAC only included health care access and use data related to asthma care. In this study, we use data from a population-based study to assess the general health status, health outcomes, and access and use of general health care services among Puerto Rican youth aged 10 to 17 years old. The purpose of this study is to add to the very limited empirical literature regarding the overall health of children and adolescents in Puerto Rico and to highlight particular areas of need.
Methods
Data for this study are from the third wave of the Asthma, Depression, and Anxiety in Puerto Rican Youth Study (ADA). In brief, ADA is a cohort study based on a probability sample of children living in Puerto Rican households. Child participants were 4 to 17 years old during wave 1 of data collection, from 1999 to 2000. Wave 3 data were collected from 2005 to 2008, when the original cohort of children were between 10 and 25 years old. Wave 3 data were collected from a stratified probability sample of all participants in the first 2 waves of ADA, with oversampling among those with asthma, anxiety, or depression. Wave 3 data were collected from a total of 641 of 825 targeted households, for a response rate of 78%. For this study, we have restricted our analyses to the 337 children who were 17 years old or younger during Wave 3 because the third wave had more survey measures of general health than the first 2 waves. Further details regarding the ADA study design and all 3 waves of data collection are available elsewhere.7,12,13
Data were collected via in-person interviews with youth and their caregivers. Measures of sociodemographics, health status, and health services access and use are based on either youth self-report or a caregiver report regarding the youth. Sociodemographic variables were reported by caregivers and include the following: caregiver education, caregiver marital status, caregiver work status, caregiver income, household composition, perceived poverty status, youth age, youth sex, and youth years of schooling. Anxiety and depression were measured using the Spanish translation of the Diagnostic Interview Schedule for Children and Youth (DISC-IV).6-7 Weight status was defined according to Centers for Disease Control and Prevention growth charts using caregiver-reported height and weight for youth 10 to 16 years old and youth self-report for those who were 17 years old. We defined obesity as body mass index (BMI) ≥ 95th percentile and overweight as BMI ≥ 85th percentile. All analyses were conducted using SUDAAN software (Survey Data Analysis; RTI International). To account for the complex survey design and nonresponse, all analyses were weighted using sample weight based on 2008 US Census Bureau data.
Results
Table 1 shows the demographic characteristics for the 337 youth participants and caregivers in our sample. Table 2 includes measures of physical and mental health status, health conditions, and access and use of health care services. One third of participants rated their physical health as excellent, whereas 44% reported that their mental health was excellent. Nearly 43% of participants were either overweight or obese. Caregivers reported that 41% of youth had been diagnosed with either asthma or bronchitis, 29% had been diagnosed with headaches or migraines, and 1 in 9 reported serious stomachaches. Nearly every child in the sample reported having a regular source of health care; however, 32% of caregivers said that their children regularly received care at an emergency department, and 29% reported regular care from an urgent care facility. Although the vast majority of caregivers reported having no trouble getting a health care appointment for their children, about 20% said that they had paid out-of-pocket for health care in the year prior to the survey.
Demographic Characteristics of Youth and Caregiver Participants in Wave 3 of the Asthma, Depression, and Anxiety in Puerto Rican Youth Study (N = 337)

Health Indicators and Access to Care Among Youth Participants in Wave 3 of the Asthma, Depression, and Anxiety in Puerto Rican Youth Study (N = 337)
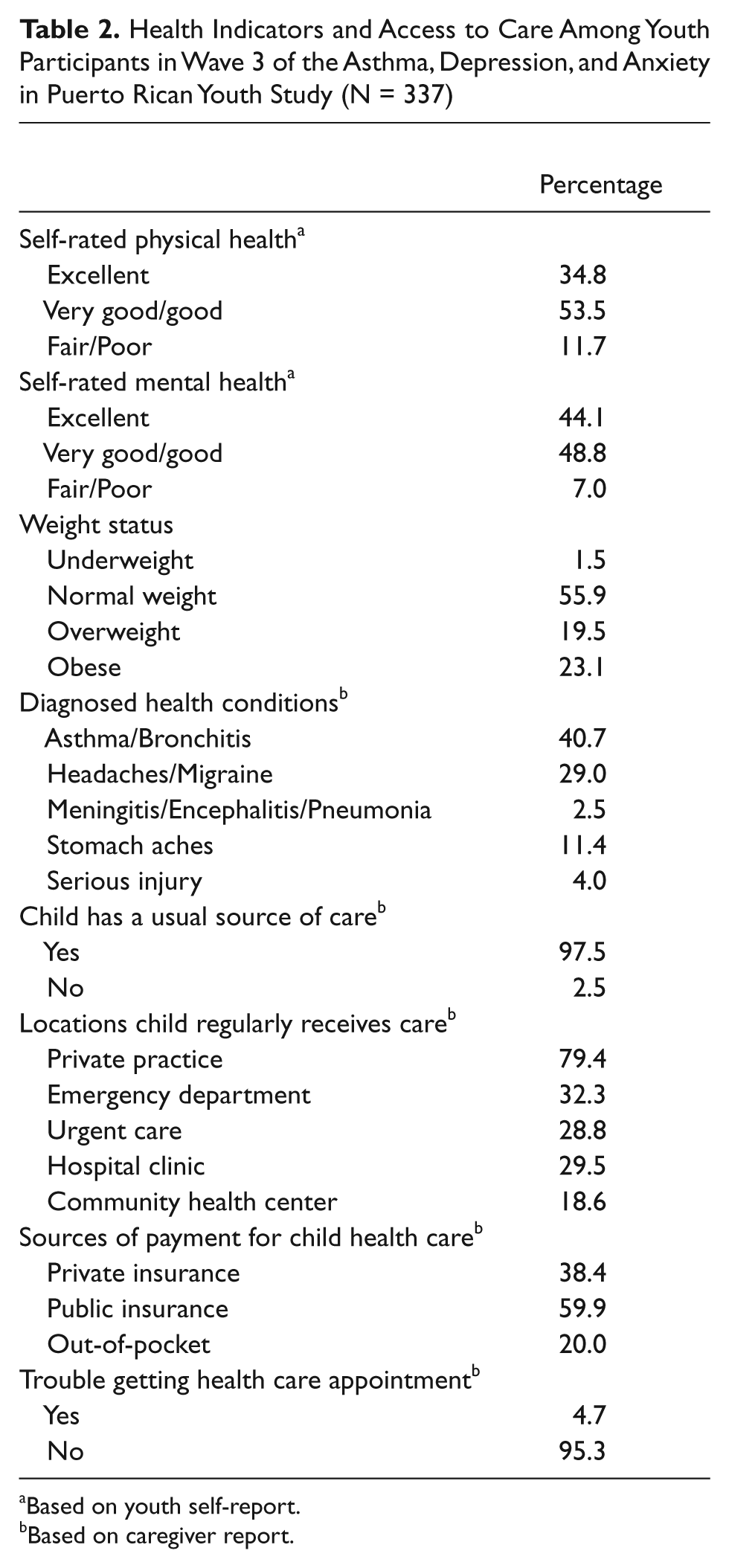
Based on youth self-report.
Based on caregiver report.
Discussion
Our study is the first that we know of to use population-based data to report on the perceived physical and mental health status among children and adolescents in the US Commonwealth of Puerto Rico. Data from the first wave of the National Longitudinal Survey of Youth found that about 39% of US adolescents 12 to 16 years of age reported that their health was excellent, and just 5% reported that their health was fair or poor. 14 We found that fewer Puerto Rican youth (35%) rated their health as excellent, and more rated their health as fair or poor (12%). Self-reports of mental health by Puerto Rican youth were better, with 44% rating their mental health as excellent. Similar to previous studies, we found that island Puerto Rican youth suffer from very high rates of asthma,3,4,8,9 overweight, 15 stomachaches, 8 and headaches. 8 The Boricua Youth Study, the only other population-based study we know of to report on headaches and abdominal pain among island youth, found that both outcomes are significantly more common in island Puerto Ricans than in youth of Puerto Rican descent living in the South Bronx. 8
Our study is also the first we are aware of to examine general health care access and use among island Puerto Rican youth. Data from the 2009 National Health Interview Survey (NHIS) suggest that about 37% of children below 18 years of age in the US mainland were covered by public health insurance at some point during the year. 16 This is a considerably lower rate than what we found among island Puerto Rican youth, 6 in 10 of whom had used public insurance in the year prior to the interview. Conversely, we found that just 38% of island Puerto Rican youth were covered by private insurance, compared with 60% on the mainland. 16 Higher rates of public insurance coverage among Puerto Rican children likely reflects the fact that poverty is far more common among island Puerto Ricans than in the general population. Further research is needed to determine what health effects, if any, result from such widespread use of public insurance. A study by Canino and colleagues 17 found that public insurance policy in Puerto Rico creates barriers to the appropriate prescription of long-term control medication for children with asthma. Additional data should be collected that will allow researchers to examine how public insurance policy affects health care access, utilization, and quality among Puerto Rican youth.
We found that very few Puerto Rican youth lack a regular source of health care; however, one third of Puerto Rican youth regularly receive care at the emergency department, and 29% regularly receive care at an urgent care facility. This figure is alarmingly high, especially considering data from the 2003 National Survey of Children’s health, suggesting that 13% of US children 0 to 17 years old received care at an emergency department once in the previous year, and less than 6% received emergency department care twice or more. 18 Our findings are consistent with the RIPRAC study, which found that a clinic-based sample of island Puerto Rican children with asthma were more than twice as likely to have been to the emergency department for their asthma than a similar sample of asthmatic children of Puerto Rican and Dominican origin who resided in Rhode Island. 9 High rates of use of emergency departments and urgent care facilities are troubling not only from a cost efficiency standpoint but also because they suggest that more appropriate care facilities may not always be available or acceptable to Puerto Rican youth and their caregivers.
This study has several limitations. One is that the ADA study set out to determine the associations between asthma and mental disorders and did not measure all health outcomes of island Puerto Rican children. We carried out secondary analyses and thus were limited to the indicators of health included in the ADA data set. Furthermore, the sample size in wave 3 may have been too small to provide accurate estimates of uncommon health outcomes such as infection and serious injury. Despite this, ADA is one of very few population-based studies to assess the health of island Puerto Rican youth. As such, we see our work as a guide for more comprehensive research into a much broader spectrum of health outcomes. Our study and others have demonstrated that island Puerto Rican youth are at a distinct health disadvantage compared with mainland youth. Puerto Ricans have poorer physical and mental health outcomes, coupled with worse access to care. Future surveillance and intervention research is critically necessary to better understand and combat the health challenges faced by youth in Puerto Rico.
Footnotes
Acknowledgements
The authors thank Pedro Garcia for conducting the statistical analyses.
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by National Institute of Mental Health (NIMH) grant R01 MH069849 and National Heart, Lung and Blood Institute (NHLBI) grant P50 HL105188.