
Abstract
Rationale
Sodium is essential for adequate growth; the daily requirement in infants is 2 to 3 mmol/kg/d.
Objectives
The study aimed to establish a reference range for the ratio of urinary sodium (UNa) to creatinine (UCr) in healthy infants in a suburban setting in the United States.
Methods
UNa and UCr were measured in healthy infants and UNa:UCr was calculated. Daily sodium intake was estimated by parental report.
Results
Mean estimated sodium intake in the 71 infants was 1.34 mEq/kg/d (95% confidence interval = 1.23-1.44). The mean UNa:UCr was 11.73 (95% confidence interval = 10.24-13.23) and did not differ significantly in age-groups. There was no direct correlation between sodium intake and UNa:UCr in healthy infants.
Conclusions
The UNa:UCr was 11.73 in this population of healthy infants. This likely reflects the appropriate physiologic response to sodium intake in the study population, which was at the lower end of the usual estimated needs for infants.
Keywords
Introduction
Sodium (Na) is an essential element for adequate growth. The sodium requirement is highest in infants and young children in whom extracellular fluid volume is rapidly expanding. In healthy infants with normal growth, the daily requirement for sodium is 2 to 3 mmol per kilogram of body weight per day. 1 Most infants are sodium sufficient; however, sodium deficiency is associated with anorexia and poor weight gain in infants. This association mimics the symptoms and signs seen in animals that have been made sodium deficient experimentally. 2 In the current era of low-sodium formulas, sensitivity to salt loss could be a reason for failure to thrive. Chloride-deficient infant formulas, intestinal chloride loss in preterm infants, and renal loss of chloride in Bartter’s syndrome have all been associated with growth abnormalities. 3 Infants with cystic fibrosis (CF) may present with hypoelectrolytemia or may suffer hypoelectrolytemia after diagnosis because of excess loss of electrolytes through sweat. 4 Sodium is an extracellular electrolyte, thus levels of sodium in the blood are an insensitive measure of total body sodium status. A low level of urinary sodium in a random sample likely indicates that the kidneys are conserving sodium because of total body sodium depletion; however, random urinary electrolyte values are affected by urine flow rate. Fractional excretion of sodium (FENa = [urine Na × plasma creatinine]/[urine creatinine × plasma Na] × 100) is a measure of the clearance of sodium relative to the creatinine clearance. Low FENa indicates sodium retention by the kidney, suggesting decreased intake or sodium loss extrinsic to the urinary system such as sodium or volume depletion through gastrointestinal or skin loss. UNa:UCr has been shown to correlate well with FENa 5 and with 24-hour urine sodium measurements 6 and avoids the requirement for blood samples and timed urine collections. Although a normal range of 17 to 22 has been imputed based on a report of infants with CF receiving sodium supplements, the range for urinary sodium:creatinine ratio (UNa:UCr) in healthy infants has not been established by direct measurement. This study aimed to establish a reference range for UNa:UCr in healthy infants.
Methods
This cross-sectional study was conducted in an ambulatory private practice setting. The protocol and informed consent document were reviewed and approved by the Children and Youth Institutional Review Board of the State University of New York at Buffalo. A research assistant approached parents of prospective study subjects at scheduled well-child visits to describe the study and solicit participation. Infants with known acute vomiting or diarrhea, including viral gastroenteritis, and those with CF or kidney disease were excluded. After informed consent was obtained, parents were asked to record a 24-hour diet recall. A urine collection bag was placed on the infant when weight and vital signs were taken at the beginning of the office visit and was removed at the end of the visit. If no urine was collected, the bag was discarded and the infant was not included in the final data set. If urine was collected, the sample was sent for sodium, chloride, potassium, and creatinine. Demographic information was obtained, including date of birth, race, gender, and weight. Since the goal of the study was to establish a reference value to help guide sodium supplementation in infants with CF, a disease that affects a mostly Caucasian population, a private practice setting was chosen that was likely to mirror this demographic. Daily sodium intake was estimated from the 24-hour dietary recall sheet. The assumptions used to estimate sodium intake are given in Table 1. UNa:UCr was calculated as follows: (urine sodium in mmol/L)/(urine creatinine in mg/dL) × 0.0883.
Assumptions Used to Calculate Sodium Intake
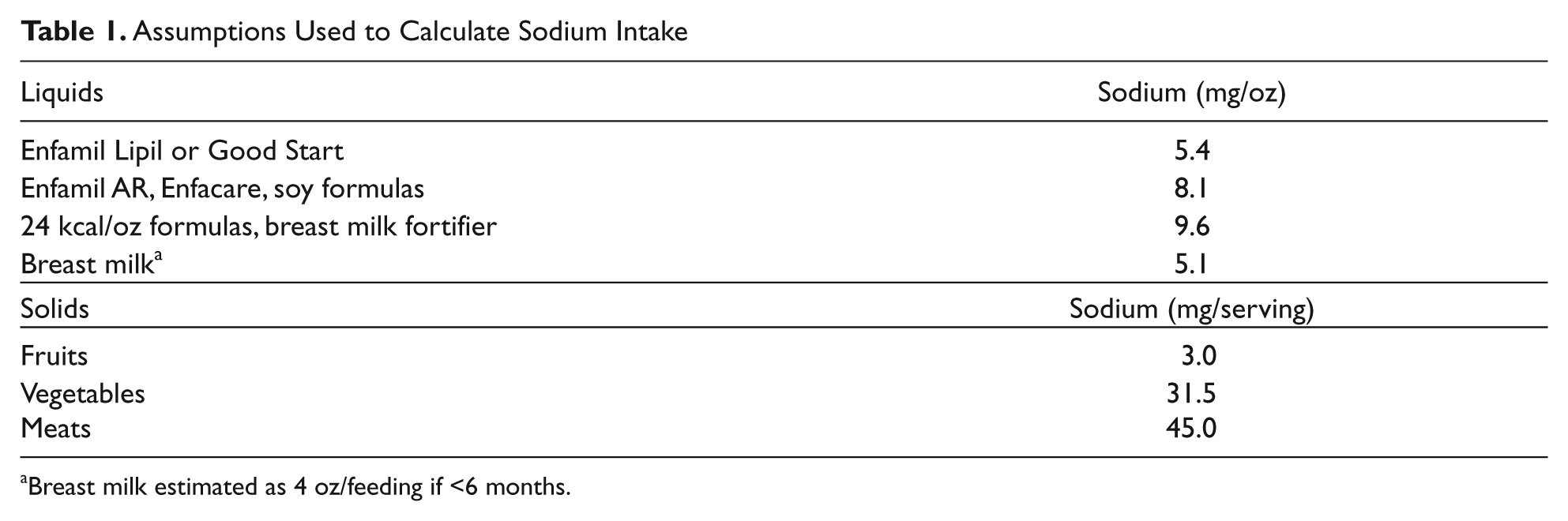
Breast milk estimated as 4 oz/feeding if <6 months.
Statistical Analysis
We assessed sodium intake, UNa:UCr in age-groups 0 to 3, 3 to 6, 6 to 9, and 9 to 12 months. Mean and standard deviation were calculated for each group. We used a Kruskal–Wallis one-way analysis of variance to determine statistical differences between age groups of Na intake and of UNa:UCr. Mann–Whitney test was used to test for significant difference between groups. We also used a linear regression model to determine if other factors such as age or estimated sodium intake significantly affect the values of the UNa:UCr. Data were analyzed using Prism Graphpad 5.02 statistical software. Based on UNa:UCr range of 17 to 52 reported previously, the standard deviation is about 7. A sample size of 100 produces a 95% confidence interval (CI) equal to the sample mean ± 1.4 when the estimated standard deviation is 7. A post hoc power calculation based on a sample size of 70 with an estimated standard deviation of 7 produced a 95% CI of ±1.7, and thus the data were analyzed.
Results
A total of 168 infants were eligible. Ninety-seven (58%) had insufficient urine obtained for measurements. Incomplete dietary data were available for 26 infants resulting in 71 complete data sets; 67.6% of infants studied were human milk fed. The mean UNa:UCr was 11.73 with a standard deviation of 6.323, standard error of 0.75 (95% CI = 10.24-13.23). The mean UNa:UCr for age-groups 0 to 3, 3 to 6, 6 to 9, and 9 to 12 months were not statistically different from each other (P = .25; Table 2).
Urinary Sodium to Creatinine Ratios (UNa:UCr) and Sodium Intake by Age-Group
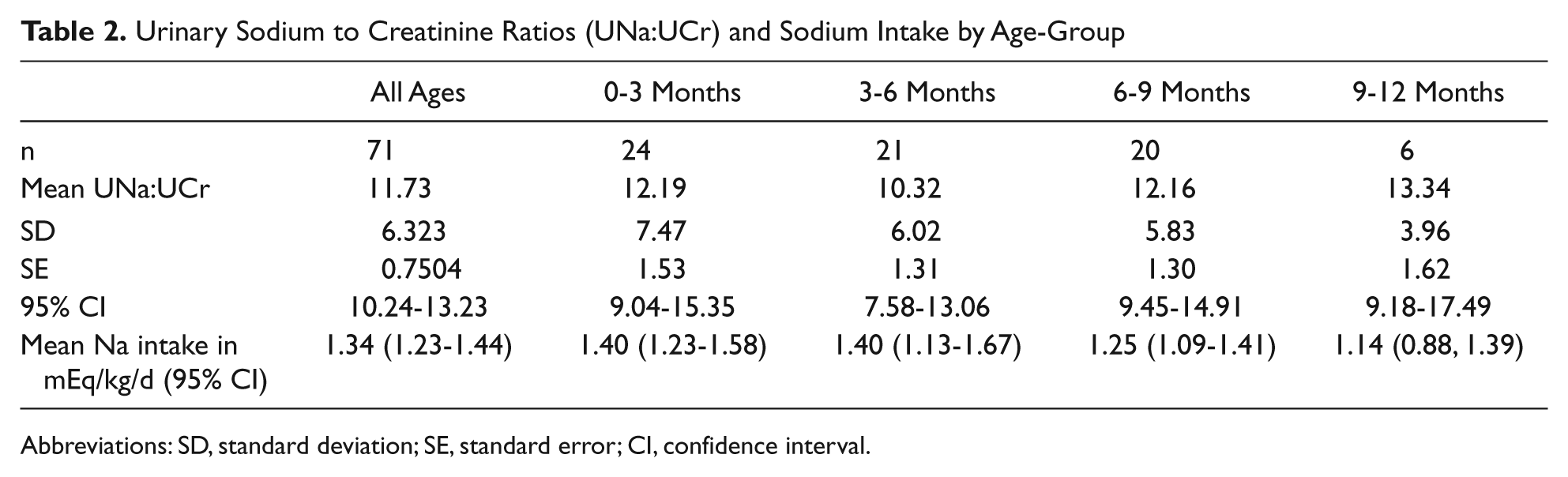
Abbreviations: SD, standard deviation; SE, standard error; CI, confidence interval.
The subjects were grouped into quartiles according to the estimated sodium intake. The mean estimated sodium intake in the lowest quartile was significantly different than that of the highest intake (0.94 mEq/kg/d vs 1.94 mEq/kg/d; P < .0001; Table 3). However, the mean UNa:UCr in the first quartile based on sodium intake (12.15 + SEM of 1.26) and the fourth quartile (12.90 + SEM of 1.68) were not significantly different from each other P = .72. Between the age-groups, there was a slight decrease in estimated Na intake in mEq/kg/d as age increased. The mean sodium intake was 1.4 mEq/kg/d in the 0 to 3 month age group and the mean was 1.1 mEq/kg/d in the 9 to 12 month age group. However, these means were not significantly different from each other (P = .26).
Estimated Sodium Intake by Quartiles
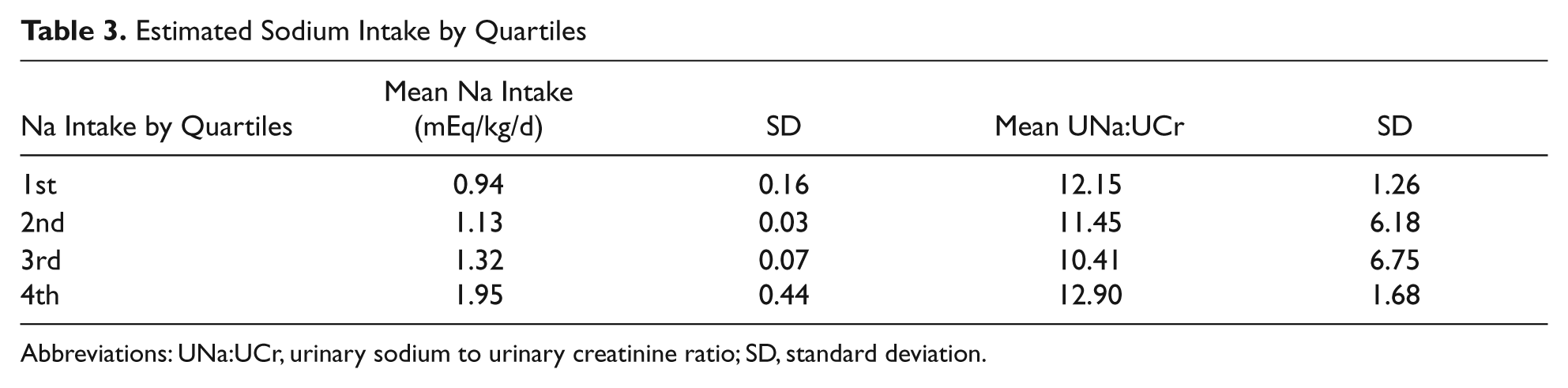
Abbreviations: UNa:UCr, urinary sodium to urinary creatinine ratio; SD, standard deviation.
Discussion
We studied the UNa:UCr in healthy infants and report it here. The range of UNa:UCr we found in our study population was lower than the range targeted for supplementation dosing in infants with CF previously reported. 5 The estimated sodium intake in our healthy infants was also low compared with the recommended intake. 1 The majority of infants in this population were human milk fed, so volume and thus sodium intake were estimates. The parental report of sodium intake also could be inaccurate from recall bias. Over recent decades the amount of sodium in infant formulas has decreased 7 and the estimated sodium intake in this population likely reflects that trend. In the infants with the lowest sodium intake, low estimated intake did not correlate with lower UNa:UCr. This could reflect an error in the assumption that UNa:UCr is an appropriate measure of sodium sufficiency, or it could indicate that low sodium intake in the range of 1 to 2 mmol/kg/d seen in our study population leads to the expected renal reabsorption of sodium.
This study was intended to obtain preliminary data to be used as reference values for the urinary sodium to creatinine ratio. For UNa:UCr to be reasonable for use as a screening measure for sodium sufficiency, it is assumed that serum sodium and creatinine are within normal limits. The infants in the study were assumed to have adequate hydration status, as they were healthy children without recent acute illnesses. Therefore, we expected that serum electrolytes and creatinine would be normal. Demonstrating a decrease in UNa:UCr with a low sodium intake and an increased UNa:UCr with a high sodium intake would be helpful in validating the ratio. However, we were unable to evaluate UNa:UCr throughout the full range of sodium intake since infants in this study had relatively low daily sodium intake. Limitations to the study include a small sample size and limited population. In summary, we have demonstrated that healthy infants in a suburban private practice setting have relatively low daily sodium intake. The low UNa:UCr seen in infants in the first year of life likely reflects the normal and appropriate physiologic response to typical sodium intake for our study population.
Footnotes
Acknowledgements
We appreciate the efforts of the physicians and office staff at Amherst Pediatrics in assisting with this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.