
Abstract
Bisphosphonates are synthetic analogues of pyrophosphate that inhibit bone resorption by their action on osteoclasts. In recent years, bisphosphonates have been used in children for treatment of a growing number of disorders associated primarily with generalized or localized osteoporosis, genetic and acquired metabolic bone diseases, heterotopic calcifications in soft tissues, and for hypercalcemia. In this review, the authors address the role of and experience with bisphosphonate therapy in disorders of childhood.
Introduction
In the human body, pyrophosphates are naturally occurring polyphosphates that prevent uncontrolled calcification by binding to newly formed crystals of hydroxyapatite. Bisphosphonates, which are stable analogues of these naturally occurring pyrophosphates, were widely used as antiscaling additives in washing powder, water, and oil brines to prevent deposition of calcium carbonate scales in industries before their biological importance was appreciated. 1 In 1968, Schibler et al 2 showed that pyrophosphate and long-chain condensed phosphates could inhibit aortic calcification induced by vitamin D3 in rats. In 1969, Bassett et al 3 reported successfully treating 2 children with myositis ossificans, a disease characterized by progressive heterotopic ossification of the connective tissue with etidronate. Since then, bisphosphonates have been used extensively in adults to prevent and treat a variety of bone conditions, such as postmenopausal and glucocorticoid-induced osteoporosis, Paget’s disease of the bone, and malignancy-induced hypercalcemia. Previously, the use of bisphosphonates in children was avoided due to concerns of potential adverse effects of these agents on the growing skeleton. During the past 2 decades, numerous studies and reports demonstrated success with high degree of safety with the use of bisphosphonates in pediatric patients although long-term outcome data into adulthood are still needed.
In the current review, we propose to acquaint the practicing pediatrician with bisphosphonates as a drug class and its role in the management of both primary and secondary bone and mineral disorders of childhood.
Bone Remodeling and Modeling
The bone undergoes normal wear and tear with time. Remodeling cycle is a mechanism by which the skeleton replaces “old bone” and repairs microdamage that occurs in bone from physiological repetitive loading during daily activity. The remodeling process involves bone resorption by osteoclasts followed by bone formation by osteoblasts, which together form a temporary structure called the basic multicellular unit. At any time there are about 1 million active basic multicellular units each measuring 1 to 2 mm in length and 0.2 to 0.4 mm in width, and it takes 6 to 9 months to complete 1 remodeling cycle (Figure 1). This allows for complete regeneration of the skeleton in about 10 years. Bone remodeling occurs with bone resorption always being followed by bone formation, a phenomenon referred to as coupling. At any time, some bone will have been resorped and not yet replaced, which is referred to as the remodeling space. In addition, modeling is the process of shaping the skeleton during growth, which is responsive to mechanical forces that are placed on the skeleton. Bone formation exceeds bone resorption and the process results in a net increase in bone mass during childhood and adolescence. Bisphosphonates, through their action on osteoclasts, decrease the rate of initiation of new remodeling cycles, resulting in fewer remodeling sites and a decrease in the remodeling space. The increase in bone mineral density observed with bisphosphonate treatment is due to the filling in of the remodeling space with new bone. 4
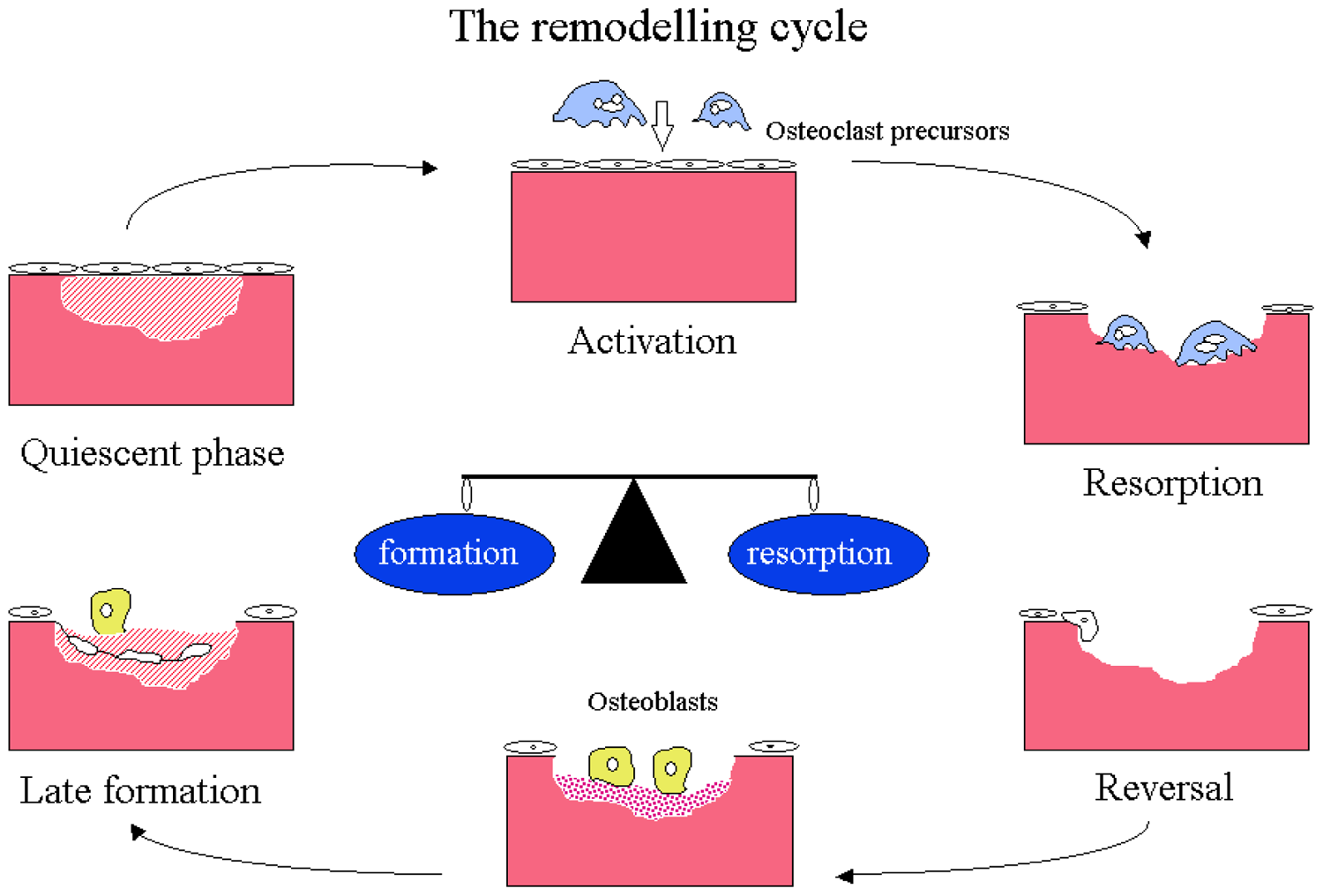
The remodeling cycle
Assessment of Bone Health in Children
Assessment of bone health in children encompasses the amalgamation of information obtained from clinical presentation, skeletal x-rays, measurement of bone mineral content, and laboratory studies for bone turnover markers and hormones related to skeletal metabolism.
Bone Densitometry
Dual-energy x-ray absorptiometry (DXA) is commonly used to measure bone mineral content (BMC) and bone mineral density (BMD) in children and adults. 5 In DXA, 2 photon energies are used to estimate BMC; low-energy photons penetrate only the soft tissue, whereas high-energy photons penetrate both the soft tissue and the bone. The differential absorption between the 2 energy strengths is used to estimate BMC. The BMC value is then divided by the projected area of the bones to calculate BMD expressed as g/cm2. The mathematical assumptions that were made in the original studies to represent a 3-D volume into a 2-D projected area, and for the shape of the bones, have been under significant debate in interpretation of DXA data, and in children multiple alternative strategies such as bone area for height, BMC for bone area, and others have been suggested. 5 The International Society for Clinical Densitometry recommends that in children we refrain from the use of “osteopenia” and “osteoporosis” and preferably use the term “low bone mineral content or bone mineral density for chronologic age.” Osteoporosis in children is defined as a Z-score equal or less than −2.0, adjusted for age, gender, and body size, as appropriate. With all its debated limitations DXA is still a useful tool in clinical practice, and even more so when one uses serial measurements in conjunction with other assessments of bone health to compare changes over time in a diseased state with or without pharmacological interventions (Figure 2). The most common error in interpreting Z-score data is failure to correct for body size, most commonly for small stature. 6 Other imaging tools used to measure BMC/BMD are computed tomographic procedures (peripheral quantitative computed tomography, quantitative computed tomography) or sonographic procedures (quantitative ultrasound), but currently they are mostly used for research purposes.
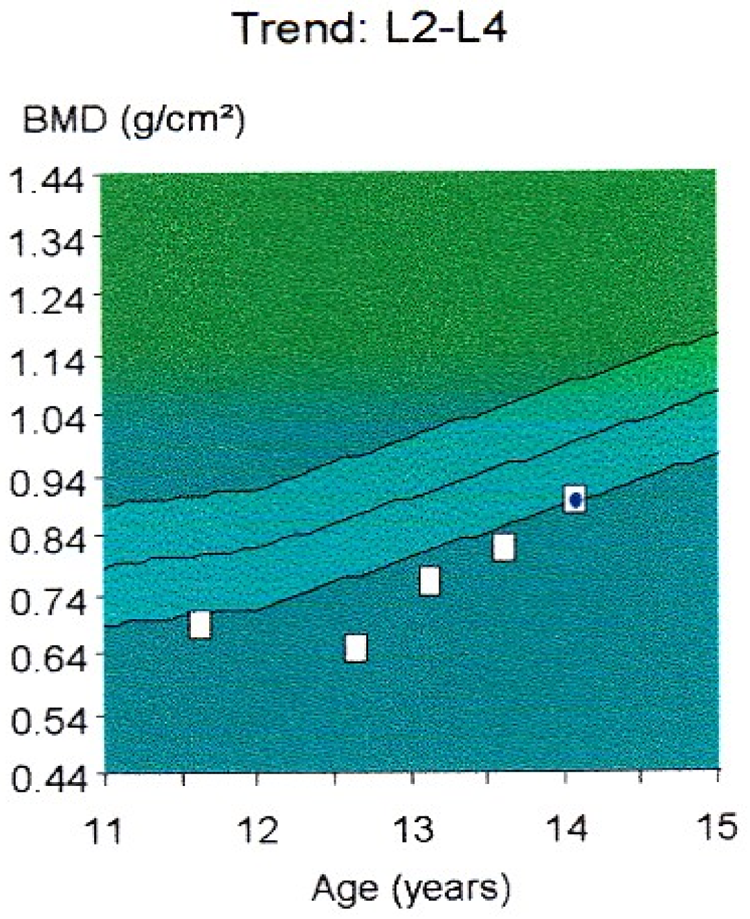
Effect of corticosteroids treatment on lumbar bone mineral density (BMD) as observed by DXA in a boy with nephrotic IgA nephropathy (with normal serum creatinine)
Biochemical Markers of Bone Turnover
Biochemical assays for monitoring bone turnover rely on the measurement, in serum and urine, of enzymes, matrix proteins, and collagen degradation products that spill over into the body fluids during the processes of bone modeling and remodeling. Markers of bone formation are all osteoblast products such as serum alkaline phosphatase, bone-specific alkaline phosphatase, and osteocalcin, while the markers for bone resorption are products of osteoclast activity such as urinary hydroxyproline, pyridinoline, deoxypyridinoline, N- and C-telopeptides, and serum tartrate resistant acid phosphatase. In daily practice, serum osteocalcin and bone-specific alkaline phosphatase are good indicators of bone formation activity though they do not always show parallel response as each may reflect the expression of these proteins at different stages of osteoblast development and synthetic activity. 7 Urinary cross-linked N-telopeptides is the most responsive bone resorption marker, followed by total pyridinoline and deoxypyridinoline. 8 Data about the physiology of bone markers in children is scant. Mora et al 9 found, as expected, that during periods of more rapid growth the values of the aforementioned parameters are elevated, reaching higher levels during infancy and again during puberty. It is also important to remember that the values are higher following a fracture (or surgery) in a major bone when normal physiology attempts to quickly replace injured bone by a healthy one. Following the initiation of therapy with bisphosphonates, a decrease in bone resorption markers can be seen and it characteristically exceeds the observed reduction in bone formation markers, indicating a total effect of increase in bone formation (Figure 3). Bone markers can be used to learn about abnormalities in bone metabolism (such as elevated serum alkaline phosphatase activity in children with rickets), the effect of drugs as aforementioned, and for long-term monitoring to make sure that the appropriate dose of bisphosphonate is used, in particular, making sure that bone metabolism does not become too suppressed, leading to a pathologic condition as adynamic bone disease and osteopetrosis (vide infra).
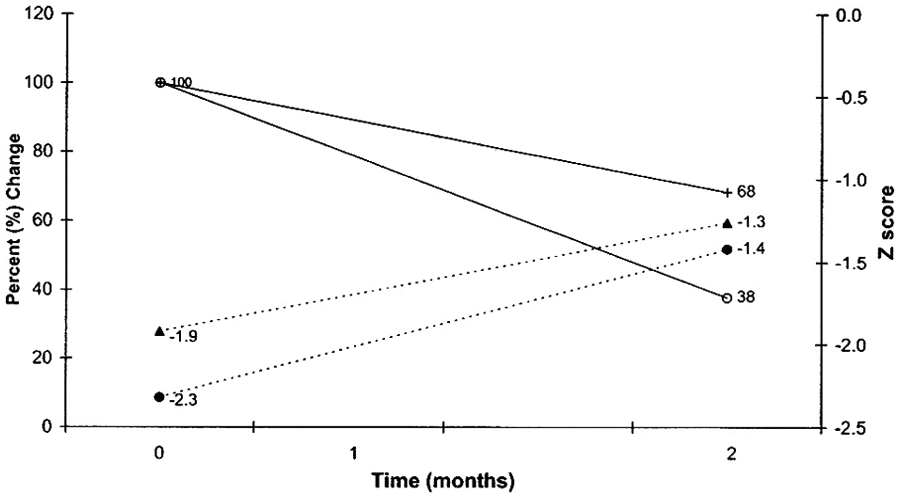
Characteristic changes in 5 children with osteoporosis treated with bisphosphonates for 12 months
Structure, Mechanism of Action, and Pharmacokinetics of Bisphosphonates
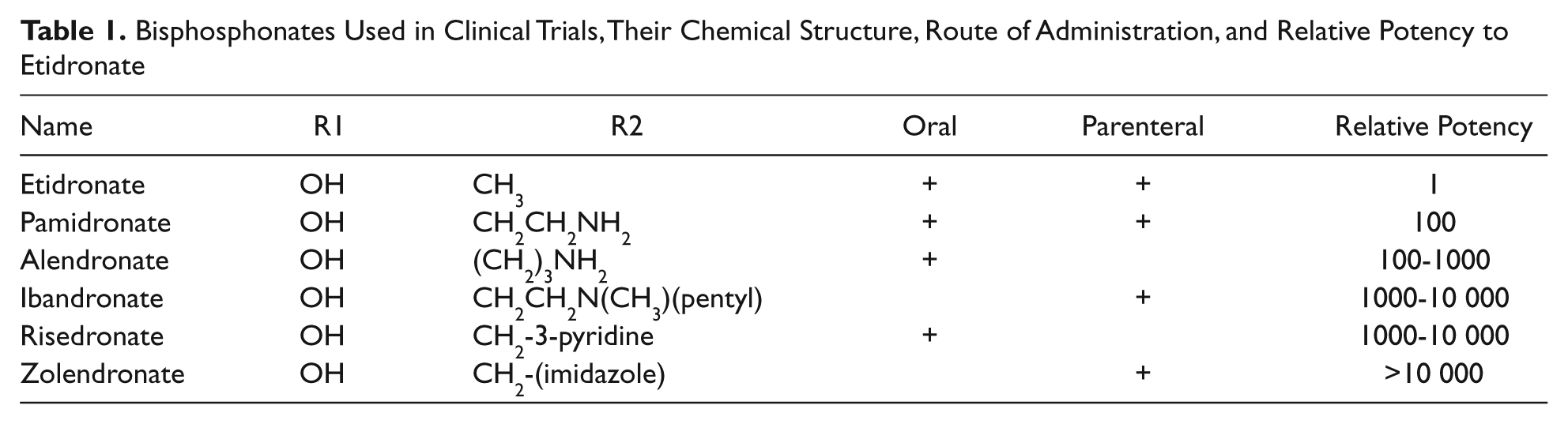
Bisphosphonates are analogues of endogenous pyrophosphate in which a carbon atom replaces the central atom of oxygen, which imparts resistance to hydrolysis of the drug by alkaline phosphatase (Figure 4). The P–C–P motif of bisphosphonates together with a hydroxyl group on the R1 side chain imparts high affinity of the drug to calcium hydroxyapatite crystal, allowing rapid and efficient targeting of bisphosphonates to bone mineral surfaces. Once localized within bone, the structure and 3-dimensional conformation of the R2 side chain become the critical determinant of antiresorptive potency and biological activity of the drug. 10 Based on the R2 chain, bisphosphonates can be either a non-nitrogen moiety or a nitrogen-containing moiety. As shown in Table 1, those with nitrogen-containing side chains (pamidronate, zoledronate, and ibandronate) have greater antiresorptive potency in vitro. 11
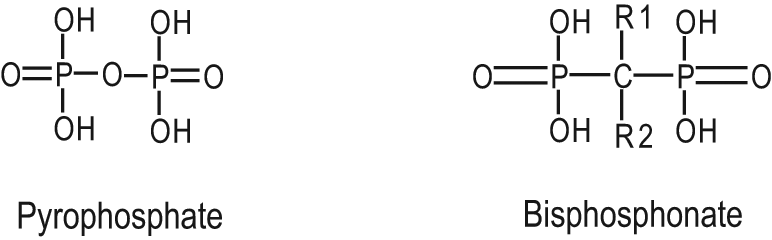
Structures of pyrophosphate and germinal bisphosphonate
Bisphosphonates Used in Clinical Trials, Their Chemical Structure, Route of Administration, and Relative Potency to Etidronate
Bisphosphonates act by interfering with the intracellular energy production, by stopping GTPase and other ATP-dependent metabolic pathways. 12 The inhibition of these critical biochemical pathways leads to significant cellular effects such as decreased osteoclast activity, inhibition of osteoclast recruitment, and apoptosis.13-16 The net effect of these cellular changes at the tissue level is suppression of bone turnover as evident on histological examination and histomorphometric assessment. Bone biopsies following therapy with bisphosphonates show no gross qualitative bone abnormalities, normal bone mineralization (normal mineral apposition rate), and decreased bone turnover (decrease in activation frequency).4,5 The increase in BMD following bisphosphonates therapy results from reduction in bone resorption, and hence these class of drugs are also termed as antiresorptive agents, in contrast to anabolic agents such as calcitonin, growth hormone, and low-dose PTH (Teriparatide).4,5
The bioavailability of the oral preparations is very poor, with less than 5% of an orally administered dose being absorbed. Additionally, the absorption is further diminished by presence of other medications, food, or liquids other than water in the upper gastrointestinal tract. Once absorbed, the half-life in serum is short as bisphosphonates rapidly incorporate into bone by binding to calcium in the hydroxyapatite crystals of the actively remodeling bone areas. Therefore, their distribution is higher in trabecular bone than in cortical bones. Around 50% of the drug is excreted in the urine without entering into the skeleton.17,18 Bisphosphonates in the bone inhibit calcification and hydroxyapatite breakdown, thereby effectively suppressing bone resorption. Additionally, they have an effect on osteoclast and osteoblast apoptosis. The half-life in the bone may be several years depending on the rate of bone remodeling. During osteoclastic bone resorption, by the surrounding acid pH, the bisphosphonate molecule becomes soluble and reenters into blood circulation, where it undergoes renal excretion. After completion of treatment course bisphosphonates can be detected in urine for weeks to months due to gradual release from the bone. 19
Bisphosphonates Use in Pediatric Disorders
Osteoporosis in Children
Osteoporosis is characterized by loss of bone mass and microarchitectural integrity, resulting in an increased bone fragility and risk of fractures with associated morbidity and mortality. Pediatric osteoporosis may arise from an intrinsic abnormality such as a genetic structural one or extrinsic factors such as certain medications (most importantly corticosteroids), nutritional, vitamin, and mineral deficiencies (vitamin D, C, K, calcium), as well chronic medical conditions associated with chronic inflammation or failure of other organs, such as liver and kidney. While primary osteoporosis is not uncommon, bone specialists see an increasing number of patients with secondary osteoporosis.
As a result of improved treatments of congenital, autoimmune, malignant, and other chronic pediatric diseases, for example, cystic fibrosis, leading to extended longevity of the patients, secondary osteoporosis has become more prevalent among them. The issue at times is further compounded by chronic therapy with glucocorticoids in many of the aforementioned disorders as well in those who receive an organ transplant (vide infra).
In general, one can divide pediatric osteoporosis into primary, which is most often genetic by nature, and secondary, which is acquired in a child who previously had a healthy skeleton.
Primary Osteoporosis
Idiopathic juvenile osteoporosis
Idiopathic juvenile osteoporosis occurs sporadically in prepubertal children with no family history of bone disease and is diagnosed of exclusion. It is characterized by recurrent fractures following minor trauma of vertebrae or long bones especially at the metaphyses, formation of new osteoporotic bone without callus formation (neo-osseous osteoporosis), and gradual remission after the onset of puberty. 20 Children may experience recurrent fractures, bone pain, and kyphosis, and in severe cases the fractures may lead to permanent skeletal damage. Bisphosphonate in children with symptomatic disease showed marked clinical improvements irrespective of bisphosphonate used in the published series; however, no control study is available.20-22 In our own experience, children with idiopathic juvenile osteoporosis associated with vertebral collapse fractures that were dependent on multiple narcotic medications and a spine brace were able to successfully discontinue all pain medications and spinal brace with adequate healing of fractures following use of intravenous zoledronic acid (unpublished observation).
Osteogenesis imperfect
Osteogenesis imperfect (OI), or “brittle bone disease,” represents a phenotypically heterogeneous group of conditions that result from more than 200 genetic mutations in qualitative and/or quantitative defect in type I collagen synthesis. 23 The clinical expression is primarily that of bone fragility, but other tissues can also be involved, including teeth, ligaments, and joints. There is no curative treatment at this point in time. In 1987, Devogelaer et al 24 first reported the use of bisphosphonates to treat bone disease in an OI patient. Since then, bisphosphonates have frequently been used in the treatment OI-related bone abnormalities, nowadays even in infants. 25 Previous case studies showed inhibition of bone resorption resulting in decreased osteoclast number and eroded surface combined with increase in cortical width, increase in cancellous bone volume, and increase in number of trabeculae. 26 Consequently, bisphosphonates decrease bone turnover markers, increase BMD, decrease fracture rate, increase vertebral size, and ameliorate vertebral misshape at the skeletal level and clinically improve quality of life by improving ambulation, providing relief from chronic pain and fatigue without affecting linear growth after administration of either intravenous or oral bisphosphonates (Table 1). Recent studies reflect no sign of deterioration of growth after such a therapy was started in infancy. In a Japanese follow-up study of OI infants, bisphosphonate prevented bone fractures and improved vertebral height, concavity index, femure BMD, and height Z score as well decrease fracture rate after cyclic pamidronate therapy at 18 months. 25 Growth hormone provided additional increase in lumbar spine, distal and distal radius’ BMD with increased growth velocity without increase in fracture rate of 15 OI children who received growth hormone therapy additionally to neridronate for 12 months. 27 Zoledronic acid provided significant decrease in fracture rate and increase in bone density on DXA in children with OI type III after 20.4 months of treatment. 28 Additional studies and our own experience support the beneficial effect of bisphosphonates in children with OI.29-32 The length of therapy and when to start treatment are still undetermined; however, early and aggressive treatment with close follow-up of OI infants is recommended to ensure growth and decrease fracture rate. 32 Of note, dental eruption has been showed to be delayed after bisphosphonate therapy as well osteotomy with hardware placement healing without adverse effect on fracture healing rate.33,34
Fibrous dysplasia of bone and McCune–Albright syndrome
Fibrous dysplasia (FD) of bone is a rare congenital disease leading to osteolytic lesions of ribs, craniofacial, and long bones. Bone biopsy of pathological tissue shows a combination of bone, fibrous tissue, and cartilage. McCune–Albright syndrome, a form of FD, consists of osteolytic lesions combined with multiple endocrinopathies that occur from an activating mutation of the Gsα proteins. 34 These conditions are associated with bone pain, bone fractures, and bone deformity due to high bone turnover reflected by raised serum alkaline phosphatase and urinary hydroxyproline. The current literature shows that bisphosphonate therapy in FD leads to decreased pain and improved mobility, although the results for radiological improvement of bone lesions in FD are mixed.35-37
Other genetic disorders with bone involvement
Bisphosphonates have been successfully employed in children with familial idiopathic hyperphosphatasia (juvenile Paget’s disease),38,39 Gaucher’s disease, 40 Hadju–Cheney syndrome (hereditary osteodysplasia with acro-osteolysis),41,42 and osteoporosis pseudoglioma syndrome. 43 The details of case reports and studies associated with the treatment of these diseases are beyond the scope of this review. Typical bone lesions of a 10-year-old girl with neurofibromatosis with cystic bone disease who benefitted from oral bisphosphonate treatment are shown in Figure 5.

Bone lesions in a girl with neurofibromatosis. Once treatment with alendronate was started she suffered no more pathologic fractures and her bone pain resolved
Secondary Osteoporosis
Glucocorticoid-induced osteoporosis
Osteoporosis is a recognized complication of corticosteroid therapy due to its variety of effects on calcium and bone metabolism, including osteoblast inhibition, increased bone resorption by stimulating osteoclastogenesis, reduction in intestinal calcium absorption, and increase in renal tubular calcium excretion. The loss of bone is particularly rapid within the first 6 to 12 months of corticosteroid use.44,45 Vertebral fractures are the most prevalent fractures associated with glucocorticoid use in children. Two-year follow-up of 55 children with glucocorticoid-induced osteoporosis suggested higher risk for osteoporosis among nonambulatory, growth-retarded children and those receiving in addition long-term methotrexate therapy or in those with positive family history of osteoporosis. Two years treatment with alendronate of those who had vertebral fractures increased spinal BMD from a Z-score of 2.69 to −1.39. 46 A similar study of 38 adults with glomerulonephritis treated with steroid, who received either vitamin D or risedronate (2.5 mg/d) or both, showed increased bone density and decreased markers of bone resorption with bisphosphonate and further improvement in the combined therapy group. 47 An illustrative case of the adverse effect of glucocorticoid treatment on spinal BMD and the beneficial effect of bisphosphonates is shown in Figure 2.
Osteoporosis associated with immobilization
Development of osteoporosis in children with cerebral palsy and other neurological conditions that confine children to bed/wheelchair has been noted for a long time. The mechanism of osteoporosis in these conditions is due to impaired weight-bearing ambulation, lack of muscular forces on bone, inadequate nutrition, low calcium and vitamin D intake, and/or anticonvulsant therapy. Children with cerebral palsy have been extensively studied. Recently, long-term follow-up studies with posttreatment observation up to 10 year after 1 year treatment with pamidronate (15 doses) showed decreased fracture rate at 1 year, which lasted for 4 years; however, a subset of children sustained fracture after discontinuation of bisphosphonates. 48 Additional, smaller, nonrandomized studies found improvement in bone density, decrease in fracture rate, and reduction in pain in children with cerebral palsy treated with bisphosphonates.49-51 Similar decrease and remarkable improvement in bone mineralization after administration of bisphosphonates were observed in children with other neurological conditions or with acute immobilization such as after spinal cord injury. 52
Osteoporosis associated with gastrointestinal disorders
Gastrointestinal diseases such as inflammatory bowel diseases, celiac disorder, or liver diseases can cause decreased bone mass secondary to decreased intestinal absorption of calcium and fat-soluble vitamins, direct effect on bone of increased inflammatory cytokines (interleukin-6), and chronic glucocorticoid use. Sbrocchi et al 53 evaluated 13 adolescents with Crohn’s disease in a double-blind randomized study, where children received either 1 dose of 0.066 mg/kg zoledronic acid or saline infusion. At 6-month follow-up there was significant increase in lumbar spine BMD in the zoledronic acid group compare with placebo (Z-score of 0.7 vs 0.1, respectively), which was still observable at 12 months with associated decreased urinary C-telopeptides excretion, indicating decreased bone resorption in the treated group. 53
Osteoporosis associated with cystic fibrosis
Children with cystic fibrosis are living longer with mean survival of more than 30 years of age. Osteoporosis has been documented in these children for some time but the rapid deterioration following lung transplantation has highlighted this problem. Poor bone health in children with cystic fibrosis is multifactorial: hormonal failure (hypogonadism), malabsorption, inadequate bone mineral accretion in childhood, pancreatic deficiency, calcium and vitamin D deficiency, reduced weight bearing exercises, corticosteroid use, presence of pro-inflammatory cytokines, and disease severity. 54 Haworth et al 55 in a placebo controlled trial of 6 months showed that BMD increased with pamidronate over the lumbar spine and hip compared with placebo. Interestingly, 75% of patients not receiving steroids developed acute severe bone pain, starting about 12 hours and lasting up to 3 days after the infusion of bisphosphonate. 56 Although “flu-like” symptoms are well recognized following administration of intravenous bisphosphonates the reason for its high frequency in this patient population is unclear. 57 A possible explanation might be lower serum 25-vitamin D vitamin levels, which were found to be associated with higher rates of “flu-like” symptoms” in patients receiving intravenous bisphosphonates. 58
Bone diseases associated with hematologic and oncologic disorders
As children with β-thalassemia survive longer, bone disease becomes a serious cause of morbidity from rickets, scoliosis, spinal deformities, nerve compression, fracture, and severe osteoporosis. The etiology is multifactorial: hormonal deficiency (gonadal failure), bone marrow expansion, nutritional deficiency, calcium and vitamin D deficiency, and desferal toxicity. 59 Recent and previous randomized placebo controlled adult trials reflected increase in BMD Z-scores at lumbar spine and hip following treatment with bisphosphonates,60,61 while it decreased or remained unchanged with Vitamin D or placebo. In our experience, there was an improvement in BMD in our patients treated with intravenous pamidronate 30 mg monthly and subsequently with zolendronate 0.5 mg monthly for 2 years, receiving the medication while in the hospital each time for blood transfusion. No complaint of bone pain and no fractures have occurred during this period.
In the study by Strauss et al, 62 the main risk factors for development of osteoporosis and avascular bone necrosis in acute leukemic processes were glucocorticoid, methotrexate therapy, as well nutritional deficiencies, reduced mobility, cranial radiation, older age, and male sex. Lethaby et al 63 recently reported improvement in lumbar spine BMD Z-score without short-term toxicity after oral adendronate administration to 15 children with acute lymphoblastic leukemia and osteoporosis while receiving maintenance chemotherapy. Successful treatment of osteoporosis has been reported also in children with congenital erythropoietic porphyria, 64 Langerhans cell histiocytosis, 65 giant cell tumor of the bone, 66 and following hematopoietic cell transplantation. 67 It is important to be acquainted also with the role of bisphosphonates in the management of bone pain originating from single or multiple lesions of both benign and malignant tumors. 68 The mechanism by which these drugs exert their analgesic effect under such conditions is yet unknown.
Bone mineral disorder of chronic kidney disease
Mineral bone disorder of chronic kidney disease starts early in the course of the disease once glomerular filtration rate is less than 70 mL/min/1.73 m2. The disease is manifested in 2 main fronts, bone disease due to the patients’ secondary hyperparathyroidism and concomitantly the development of vascular calcifications and subsequent arterial stiffness that are regarded as major contributing factor to cardiovascular morbidity and mortality in these patients. Due to their bone disease this patient population is at high risk to develop bone pain and fractures even after receiving a kidney transplant. Several studies were conducted in adults and the majority did show a beneficial protective effect of bisphosphonates in decreasing the rates of fracture.69-73 However, in the pediatric population their efficacy and safety have not been documented and consequently in their recent extensive review Haffner and Fisher 74 concluded that at this point bisphosphonates should be used only under research protocols.
Because bisphosphonates are cleared by the kidneys, it is very important to keep in mind that when given to a patient with either acute or chronic impairment in kidney function a dose adjustment and slower infusion rate are indicated (vide infra). On the other hand, concerns expressed in the past about possible nephrotoxicity of bisphosphonate administration have not materialized in the pediatric population when appropriate dose modification protocols are used (vide infra).
The Use of Bisphosphonates in Heterotopic Calcifications
Fibrodysplasia ossificans progressiva, alternatively called myositis ossificans, is a rare autosomal dominant disorder that is characterized by symmetrical congenital skeletal abnormalities and progressive heterotopic ossification of the connective tissue. Fibrodysplasia ossificans progressiva is a better term over myositis ossificans as the fibrodysplastic process occurs not only in the muscle but also in other soft connective tissue. It is believed to result from a mutation in the ACVR1 gene on chromosome 2q23, which is believed to regulate bone morphogenetic proteins. 75 Treatment with bisphosphonates has shown improvement in ambulation and a significant reduction of previously existing calcifications and the disappearance of some new ectopic ossifications.76,77 Generalized arterial calcification of infancy is a rare genetic disorder, and presents with untreatable hypertension due to arterial stenosis subsequently to calcification of the media and proliferation of intima. Infants usually die within first month of life. Several cases have been reported with complete resolution of arterial calcification with chronic bisphosphonate therapy. 78
Hypercalcemia
Severe hypercalcemia, defined as total serum calcium above 14.0 mg/dL, is an emergency that can quickly become a life-threatening event due to its cardiotoxicity. Etiologies of hypercalcemia in childhood include malignancies, hyperparathyroidism, vitamin D toxicity, thyrotoxicosis, neonatal and infantile genetic disorders such as hypocalciuric hypercalcemia, Williams syndrome, or subcutaneous fat necrosis. Complications secondary to hypercalcemia include emesis, polyuria, systemic hypertension, convulsions, coma, renal failure, and as aforementioned dysrhythmias. The most common etiology of severe hypercalcemia in children is hematological malignancy. It occurs either from direct invasion of the skeleton by malignant cells that release bone resorbing cytokines or from production of parathyroid hormone related protein (PTHrP), which when secreted into the circulation leads to osteoclastic bone resorption. 79 Whereas the normocalcemic effect of bisphosphonates is excellent in those with invasion of bone by malignant cells, it is only partial in PTHrP-related hypercalcemia as the drug cannot counteract the calcium reabsorption in the kidneys stimulated by PTHrP. Bisphosphonates are now used in adults as first-line treatment for tumor-induced hypercalcemia. Case reports in the pediatric literature also support the beneficial effect of such treatment. 80 Moreover, as some patients develop acute renal failure secondary to the hypercalcemia, the treatment with bisphosphonates reverses this condition as well. 80 It is important to remember though that hypercalcemia also causes dehydration, and therefore adequate hydration continues to be an important element in the treatment of these patients, often accompanied by furosemide for its diuretic and calciuric properties. 80 Our experience shows that these children are highly responsive to the bisphosphonate treatment and therefore half the usual dose is needed, and if renal failure is present the dose should be further halved, thus ending in 0.25 mg/kg. The dose can be repeated a few days later if needed. As shown by Srivastava et al, 79 it is also important to keep in mind that when combined with anticancer therapy, some children treated with bisphosphonates may develop a “hungry-bone like” picture in which the bones starting to rebuild themselves avidly move calcium, phosphate, and magnesium from the circulation to the bone. This may result in hypocalcemia, hypophosphatemia, and hypomagnesemia, and supplementation with these minerals for several weeks is required. 58 Vitamin D toxicity in the infant poses a special challenge due to the fact that the vitamin is fat soluble and hence its effect may last weeks. A few cases have been reported, that after failing to respond to conventional therapy their hypercalcemia resolved with single dose of pamidronate.81-83 About 15% of children with Williams syndrome, a genetic condition associated with elfin face, supravalvular aortic stenosis, and behavioral changes develop hypercalcemia, which responds to treatment with bisphosphonates.84-86
Adverse Effects
In general, bisphosphonates are well tolerated when given either orally or intravenously. However, as true for any other drug, some patients may develop adverse effects. It is extremely important though to differentiate between adverse effects seen in the adult, often an elderly, and the child. Whereas great concerns were expressed about the development of osteonecrosis of the jaw following dental procedures in adults, there has not been a single case report in a child.87-89 The pediatrics concern for pediatrics of growth impairment has remained unproven; in fact, treatment with bisphosphonates resulted in improved growth in children with OI. 25 Similarly, the hypothetical concerns about potential teratogenicity have never materialized either, as demonstrated in a few offspring of women who were treated with bisphosphonates during pregnancy.1,90
Although rare, the most common adverse effect of taking bisphosphonates orally is gastrointestinal reflux, which in extreme cases may lead to corrosive esophagitis.91,92 It is therefore important when taking the medicine to take precautions against the development of back flow of the drug from the stomach to the esophagus and to provide consideration whether to prescribe the oral route in those with known gastro-esophageal reflux. Special instructions on how to provide the oral preparations should be discussed with the family (vide infra).
The 2 more common adverse effects to the intravenous administration route are the development of “flu-like” symptoms and that of symptomatic hypocalcemia manifested by tetany and/or prolongation of QTc interval.57,93,94
There are reports of bisphosphonates leading to a delay in bone healing after an orthopedic procedure such as osteotomy with or without placement of hardware, but not with clinical (nonoperative) fractures. It has become prudent, although not scientifically supported, to hold bisphosphonate treatment 3 to 4 months before an elective surgery and resume it only after the bone has fully healed from the operative procedure. 95 An additional potential adverse effect is drug toxicity on the bone itself caused by cumulative overdose. This results in drug-induced osteopetrosis with bone pain and recurrent fractures. 89 Besides the typical findings on x-rays bone markers are depressed (Figure 6). Fortunately, if diagnosed early enough and the medication held in time, it can reverse itself. 94 In some cases treatment can be resumed after recovery of bone metabolism. 22 The recovery however requires several years, due to the fact that as previously discussed the drugs stay in the bones for a prolonged time. As showed by us in the past, in the majority of patients the last phenomenon plays to their advantage by extending the beneficial effect of bisphosphonates on bone up to 2 years after their discontinuation. 96

Osteopetrosis-like picture in a child with osteogenesis imperfecta treated with high intravenous bisphosphonate doses over a 4-year period (compare with Figure 7)
Treatment Protocols at Our Center
Intravenous and oral bisphosphonate therapy in our Bone and Mineral Disorder Clinic is offered to children with either primary or secondary osteoporosis who have fragility (atraumatic or minimally traumatic) fractures, severe bone pain, and/or are planned for corrective major orthopedic surgery. The goal of bisphosphonate therapy in most children is to prevent or minimize frequency of bone fractures and/or bone pain, achieve a satisfactory BMD, improve or prevent further worsening of bone quality, with no or minimal adverse effects. In other categories of patients the drugs are used to treat extraskeletal calcifications and hypercalcemia.
Prior to initiation of bisphosphonate therapy, a baseline evaluation history of fractures in the previous 2 years, skeletal pain (as reported by the patient and the guardians), dental problems, and dietary intake of calcium and vitamin D are recorded and anthropometrical data obtained. Laboratory evaluation includes serum creatinine, calcium, phosphorous, parathyroid hormone, 25 vitamin D, osteocalcin, bone-specific alkaline phosphatase, and creatinine kinase, and random urine for urinalysis, urinary calcium/creatinine ratio, and urine N-telopeptides. Imaging studies include radiographs of the left knee and BMDe obtained by a densitometer with pediatric software. The above-mentioned same data are collected prior to each treatment session besides radiographs of the left knee and bone density, which are conducted every 6 months. After completion of therapy, all data continue to be collected on a semiannual/annual basis for at least a minimum of 5 years.
In children in whom intravenous therapy is elected, either pamidronate or zoledronic acid are prescribed. Pamidronate is given at 0.75 to 1.0 mg/kg/dose in normal saline over 3.5 hours and zoledronic acid at 0.025 mg/kg/dose in normal saline over 30 minutes. The first dose is regarded as a “test dose” and given at half strength. In patients with impaired kidney function, all doses should be decreased by 50%. Children are given acetaminophen or ibuprofen an hour before and 5 to 6 hours after treatment. The frequency of infusions depends on the condition indicating the treatment; in general, they are given every several months. Not uncommonly the first dose is given in our institution, and if tolerated well subsequent doses are given by the primary care provider.
In children with severe or resistant hypercalcemia, our choice is a single dose of pamidronate 0.5 to 1.0 mg/kg intravenously, and if the child’s clinical condition so demands, a repeat dose is given after 2 to 7 days. It is important in such cases to closely follow serum calcium as in some cases it may drop to very low concentrations requiring calcium supplementation.
In case oral therapy is elected, alendronate is regarded as drug of choice (it should be stressed that other health providers may have other drug preferences). It comes in the form of tablets of 5, 35, and 70 mg. The standard dose is 1 mg/kg, not to exceed 70 mg, given once weekly. In young children and those with G-button the pill can be crushed and dissolved in 60 mL of tap water. To minimize potential adverse effects in the gastrointestinal tract and assure maximum absorption, the following instructions are given:
The medicine is taken in the morning on an empty stomach, or 2 hours after the last meal with 6 to 8 oz. of tap water only (no other fluids allowed).
To sit upright or stand and not to lie down for the next 45 minutes.
Not to eat for at least the next 45 minutes.
Calcium supplements should not to be taken for at least 1 hour after taking the medicine.
In all children treated with bisphosphonates by either route for osteoporosis we recommend supplementation with RDA (recommended daily allowance) of calcium and vitamin D. In those with vitamin D insufficiency, treatment with vitamin D is prescribed and bisphosphonates held until the patients are replenished with the vitamin.
A characteristic sclerotic line is consistently observed at the metaphyses of long bones (around the knees and the distal forearm) and in the vertebrae when the treatment is given before closure of the epiphyses is complete, and has no clinical consequence. 97 A gradual decrease and subsequent complete disappearance over time of these sclerotic lines are observed after withdrawal of therapy. In children who receive repetitive doses of intravenous pamidronate or zoledronic acid, a typical picture of multiple transverse sclerotic lines representing individual treatment cycles are seen at the end of long bones (Figure 7).
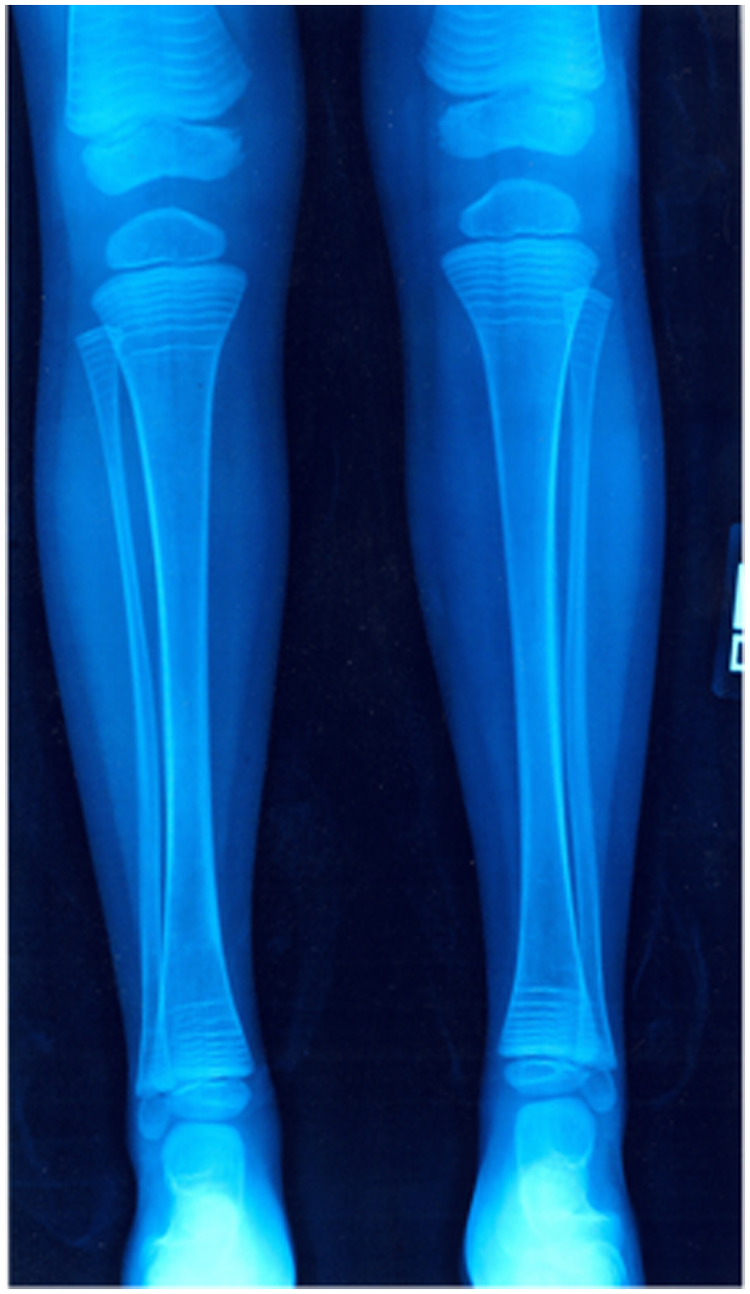
Characteristic finding on X-rays in a child treated with intravenous bisphosphonates in a protocol providing a dose of the drug every several months. Each transverse sclerotic line seen at the end of long bones represents 1 treatment session
Bisphosphonate therapy is discontinued when the goals of the planned treatment are achieved or earlier if (a) Z-scores on DXA scan become −1.0 or higher, (b) pain has been alleviated, or (c) if adverse effects related to therapy develop. Consequently, the duration of therapy may vary among patients. In general, though, in most children bisphosphonate therapy is given for 1 to 2 years except in children with OI where the recommended therapy is 3 to 5 years. We do not go beyond a total of 5 years of continuous therapy. As aforementioned the effect of the drugs last up to several years after their discontinuation; however, in some children, after a few years of being off the medication there might be a need to reinitiate it due to recurrence of fractures and/or bone pain and/or significant decrease in BMD Z-score. In most cases a brief “booster” course suffices.
Conclusions
Bisphosphonates exert their antiresorptive effect by inhibiting bone resorption by their action on osteoclasts. They are being used in children in 4 broad categories of generalized osteoporosis whether primary or secondary, localized bone disease, soft tissue calcifications, and hypercalcemic states. Both intravenous and oral preparations are well tolerated and safe in the doses used in clinical trials. Their use has demonstrated to result in increased bone strength, improved height Z-score, decreased pain, decreased fracture rate, provided protection from extraskeletal calcifications, and increased correction of hypercalcemia. Adverse effects are rare but require the appropriate precautions and recognition by the physician. Furthermore, due to the fact that at this point they are still not routinely prescribed, the evaluation of the child for bisphosphonate therapy and their administration and monitoring requires the collaboration between the primary care provider and specialists in pediatric bone and mineral metabolism.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.