
Abstract

Introduction
Observational research suggests that early age at menarche and other menstrual cycle characteristics are considered important risk factors for breast cancer. 1 Endogenous estrogen, especially estradiol concentrations, peak with ovulation, stimulating cell proliferation in the breasts and ovaries. Earlier menarche or menopause at a later age may cause more lifetime exposure to higher estrogen levels, thereby increasing the risk for breast cancer. 2
Birth size is an indicator of fetal growth and may reflect intrauterine exposure to estrogen. The association between birth size and age at menarche has been studied, with inconsistent results.3-5 Moreover, prenatal growth stress may lead to metabolic reprogramming in utero. 6 Insulin sensitivity shifts to resistance, so that the fetus can uptake the maximum amount of available energy and nutrients. This metabolic adaptation remains after birth and, in turn, can trigger rapid postnatal growth and subsequently earlier onset of puberty and menarche. 7 To date, limited research has been conducted with nationally representative data. Therefore, we examined the relationship using the National Health and Nutrition Examination Survey (NHANES) cycles 2003-2006.
Methods
The continuous NHANES is a large, national, cross-sectional survey that is designed to evaluate the nutrition and health status of the US population. Data are collected continually and are released in 2-year increments. Details regarding the survey design, data collection, and procedures can be found elsewhere (Centers for Disease Control [CDC]/NHANES analytic guidelines). All nonpregnant girls 8 to 15 years of age who provided complete demographic information, early childhood and reproductive health data, anthropometric measurements, serum for cotinine measurement, and dietary data to assess total energy and total fat intake were included. Birth weight was recorded to the nearest ounce as reported by the parent/guardian and later converted to grams. Age- and sex-specific body mass index (BMI) percentiles were calculated using the SAS Program for the Growth Charts (CDC). Current weight status was classified as obese (>95th percentile), overweight (85th-95th percentile), and lean (<85th percentile). Age at menarche (reported to the nearest year) was collected from the Reproductive Health Questionnaire. Survey participants who had not started menstruating at the time of interview were excluded.
All statistical analyses were performed using SAS 9.3 (SAS Institute, Cary, NC). Data from the 2003-2004 and 2005-2006 cycles were combined to increase statistical power. The 4-year sample weights and specific survey procedures were used. Those who reported other than Mexican American, non-Hispanic black, or non- Hispanic white as their race/ethnicity were excluded because of small numbers. PROC SURVEYFREQ was used to determine the frequencies of categorical variables. Pairwise comparisons (PROC SURVEYREG) were performed to estimate means and standard errors (SEs) and to evaluate the differences in age at menarche between different categories for each variable of interest. Multiple linear regression models (PROC SURVEYREG) were used to evaluate the associations between age at menarche and birth weight as both continuous and categorical predictor variables. Potential covariates, including survey cycle, race/ethnicity, socioeconomic status, participant’s current smoking status, BMI-for-age percentile, maternal age when the participant was born, maternal smoking status during pregnancy, physical activity, and current total energy and total fat intake, were examined. Interactions between birth weight and related covariates were examined, and nonsignificant interactions were removed. Statistical significance was set at P < .05. All aspects of the present study were approved by the institutional review boards of the Pennsylvania State University.
Results
Demographic Characteristics
A total of 652 girls were included (Table 1); 14.2% were Mexican American, 17.0% were non-Hispanic black, and 68.8% were non-Hispanic white. As regards birth weight, 82.6% were in the normal range, and 7.7% were lower than and 9.7% were higher than normal. The overall mean (±SE) of age at menarche was 11.86 (±0.05) years (range = 8-15 years). The relationship between age at menarche and the continuous birth weight variable was not statistically significant (Table 2, model 1; P = .868). Compared with non-Hispanic white girls, age at menarche was 0.47 years (~6 months) earlier among non-Hispanic black (P < .001) and 0.24 years (~2.9 months) earlier among Mexican American girls (P = .048). Girls who were heavier in adolescence had their first menstrual cycle earlier (P < .001). Maternal smoking status during pregnancy (P = .159) and maternal age had no effect on daughter’s age of menarche (P = .839, data not shown). In model 2, compared with those of normal birth weight, girls with both low and high birth weights experienced menarche 0.24 years (~2.9 months) and 0.32 years (~3.8 months) earlier, respectively; with a marginally significant association observed for the high-birth-weight group (P = .072).
Demographic Characteristics and Sample Size of 8- to15-year-old Adolescent Girls: NHANES 2003-2006 a
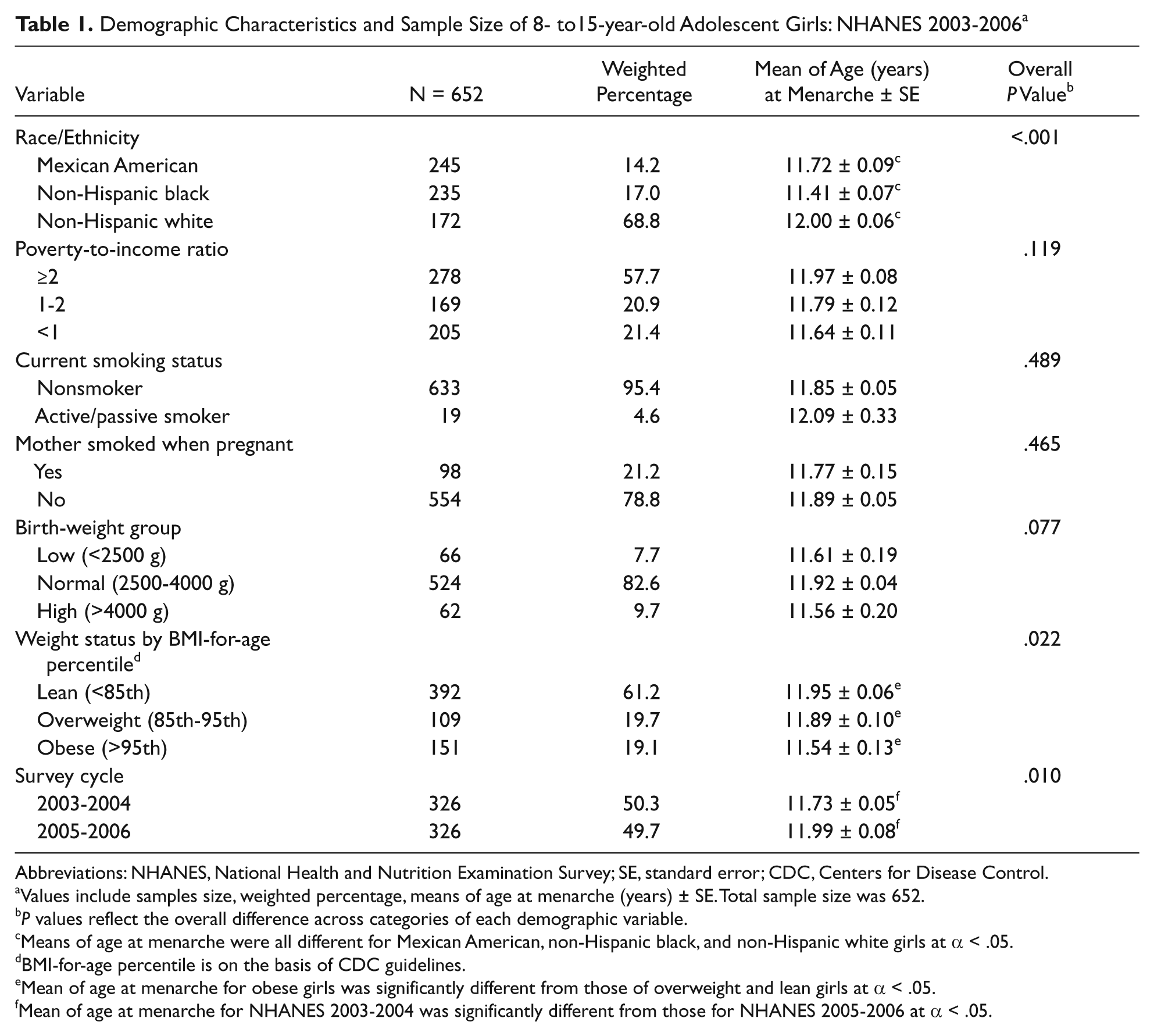
Abbreviations: NHANES, National Health and Nutrition Examination Survey; SE, standard error; CDC, Centers for Disease Control.
Values include samples size, weighted percentage, means of age at menarche (years) ± SE. Total sample size was 652.
P values reflect the overall difference across categories of each demographic variable.
Means of age at menarche were all different for Mexican American, non-Hispanic black, and non-Hispanic white girls at α < .05.
BMI-for-age percentile is on the basis of CDC guidelines.
Mean of age at menarche for obese girls was significantly different from those of overweight and lean girls at α < .05.
Mean of age at menarche for NHANES 2003-2004 was significantly different from those for NHANES 2005-2006 at α < .05.
Relationship Between Age at Menarche (years) and Birth Weight.
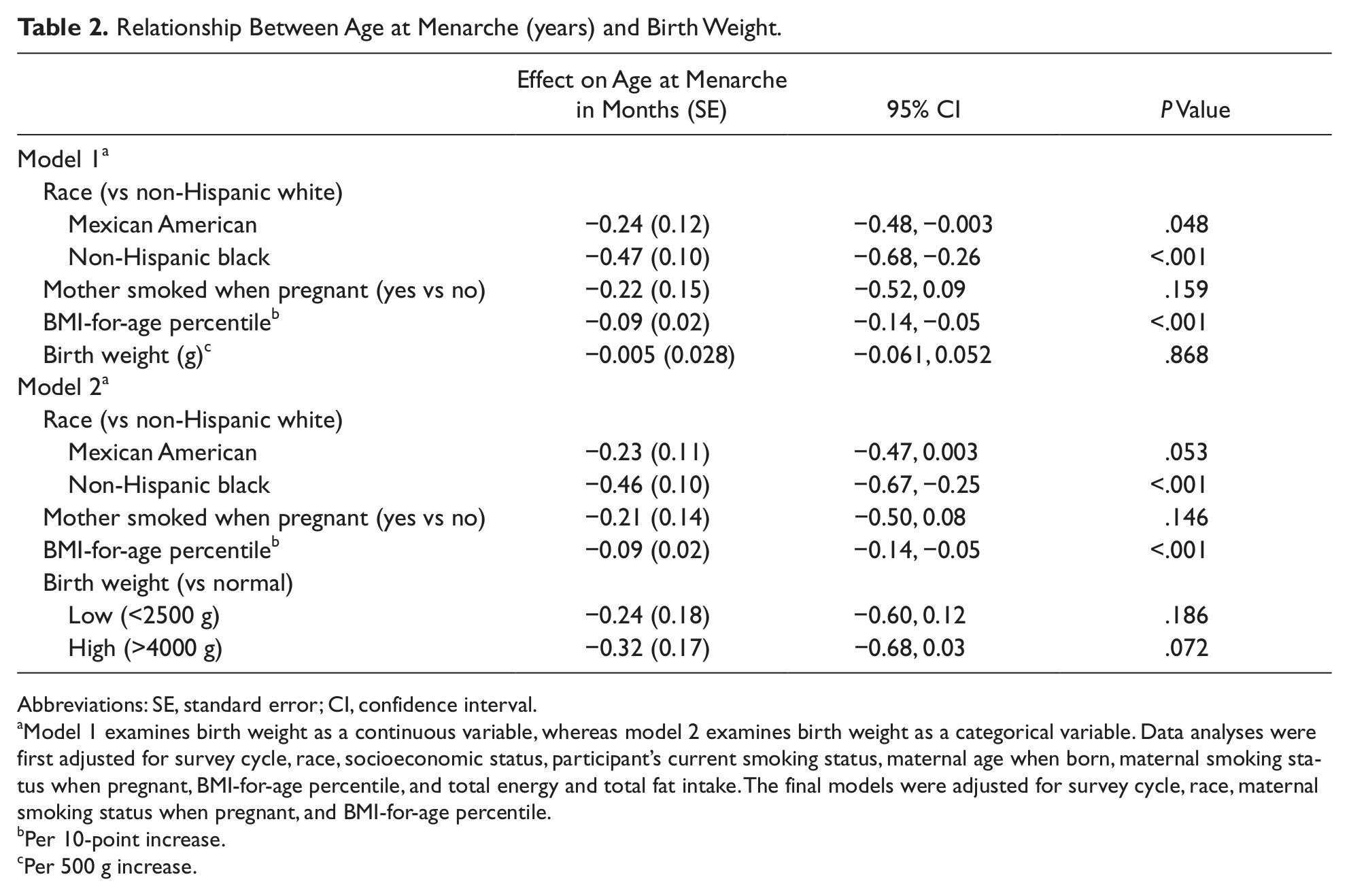
Abbreviations: SE, standard error; CI, confidence interval.
Model 1 examines birth weight as a continuous variable, whereas model 2 examines birth weight as a categorical variable. Data analyses were first adjusted for survey cycle, race, socioeconomic status, participant’s current smoking status, maternal age when born, maternal smoking status when pregnant, BMI-for-age percentile, and total energy and total fat intake. The final models were adjusted for survey cycle, race, maternal smoking status when pregnant, and BMI-for-age percentile.
Per 10-point increase.
Per 500 g increase.
Discussion
In the present study, we observed a nonsignificant inverse association between age at menarche and low birth weight, both as a continuous variable and modeled categorically. As mentioned earlier, the metabolic reprogramming in utero may lead to catch-up growth through infancy and childhood. 6 Observational studies have shown that low-birth-weight children have higher circulating adrenal androgen concentrations, 8 and this precocious adrenarche usually results in earlier menarche in girls. In our analyses, average birth weights across the 3 birth-weight groups were significantly different; however, BMI-for-age percentiles of these girls at NHANES interviews across the 3 birth-weight groups were similar (data not shown). These results suggest that more rapid postnatal growth occurred among lower-birth-weight girls and may partially explain the earlier attainment of menarche.
High-birth-weight girls experienced earlier menarche in our analyses. Studies have shown a positive relation between birth weight and the concentrations of cord blood insulin-like growth factor-1 (IGF-1) and leptin. Circulating IGF-1 concentration peaks during the pubertal growth spurt. 9 Perhaps, high-birth-weight girls have elevated IGF-1 levels throughout childhood, and they experience menarche earlier. Moreover, higher leptin levels stimulate the timing of puberty. 10 Overweight/obese girls possess more body fat than lean girls, resulting in increased circulating leptin concentrations that may act to trigger earlier menarche.
There are several strengths in our study. To our knowledge, this study was the first to evaluate the association between birth weight and age at menarche using the nationally representative continuous NHANES data set. Second, the NHANES includes a socioeconomically and racially/ethnically diverse sample. There are also a few limitations to our study. The data are cross-sectional, and birth weight and age at menarche are both retrospectively self-reported; therefore, we are unable to evaluate the relationship between birth weight and age at menarche with the precision of a prospective analysis. The NHANES collects data on age at menarche to the nearest year, and random misclassification may underestimate the true effect of birth weight on age at menarche.
In summary, findings from the NHANES 2003-2006 suggest that being at either extreme of the birth weight distribution is associated with earlier menarche. High birth weight was a more important predictor for age at menarche.
Footnotes
Acknowledgements
We would like to thank Jacqueline Vernarelli, PhD, and Diane Mitchell, MS, for their help with data interpretation.
Authors’ Note
The authors’ contributions were as follows: ZZ designed the research, conducted data analysis for the research, and had primary responsibility for the manuscript; TJH contributed to data interpretation and manuscript preparation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.