
Abstract
Background. Youth violence is a widespread public health problem. Despite recommendations to address youth violence by the American Academy of Pediatrics, it is unclear how often primary care practitioners (PCPs) do so. Purpose. To determine PCPs’ documentation of violence involvement. Methods. Children 11 to 17 years old were enrolled while attending a clinic. They completed questionnaires assessing violence involvement confidentially without the knowledge of the PCP. The primary outcome, documented reference to violence involvement, was determined by chart review. Results. A total of 165 youth participated: mean age = 14.5 years (standard deviation = 1.7), 43% male, 46% white. In all, 14.5% of charts documented any violence involvement. Of the 20% of youth who reported serious violence involvement, PCPs documented violence issues 19.4% of the time. Factors associated with documentation included nonwhite race (P < .05), having public (or no) insurance (P < .001), visit type (routine checkup (P < .05), and clinic site (P < .001). Conclusion. PCPs infrequently document discussion of violence-related issues, specifically in youth who are demonstrating risk.
Keywords
Introduction
Youth are involved with violence at an alarming rate, as victims, perpetrators, and witnesses in the context of peer, dating, and family situations. Involvement with violence has a profound impact on future school performance, substance use, mental health issues, and delinquency.1,2 Significant health disparities exist when evaluating morbidity and mortality related to youth violence because minority youth and youth from lower-income groups are affected at a higher rate than white, higher-income-group youth. 1
Overall, 33% of high school students surveyed by the Youth Risk Behavior Surveillance System 3 in 2011 were in a physical fight within the past year. Approximately 26% of male youth reported carrying a weapon such as a gun, knife, or club in the past 30 days, with little change since 1999. 3 Homicide is the second leading cause of death in adolescents and young adults. In 2010, 228 000 youth 15 to 19 of age were treated for nonfatal injuries sustained from assaults, representing the fifth leading cause of injury in this age group. 4 In a confidential, national phone survey of youth and their violence exposure, Finkelhor et al 5 found that 48% of teenagers were victims of a physical assault, and 16% were injured as a result of the assault in the past year. The direct and indirect costs of youth violence are estimated to exceed $158 billion per year. 6
Both the American Medical Association (AMA) and the American Academy of Pediatrics (AAP) have strongly encouraged primary care practitioners (PCPs) to screen youth for violence-related behavior.7-9 The AAP’s Task Force on Youth Violence published recommendations in 1999, with an update in 2009 describing the role of the pediatrician in youth violence prevention. The AAP argued that because violence and injuries are a serious threat to the health of children, “pediatricians should incorporate preventive education, screening for risk, and linkages to necessary intervention and follow-up services.” Despite the recommendations of the AAP and AMA, health care professionals are not routinely identifying or diagnosing violence issues in the youth they work with. In a study of self-reported pediatricians’ violence screening practices, Borowsky and Ireland 10 found that 67% of practitioners never or rarely asked adolescents about their involvement in physical fighting. In a cross-sectional sample of pediatricians in California, Chaffee et al 11 found that pediatricians reported screening their patients only 31% of the time for fighting, 39% of the time for violence in the home, and 29% of the time for weapon carrying. Additionally, Sigel et al 12 examined the rate of diagnoses of assault injury and violence risk in the primary care setting using the National Ambulatory Medical Care Survey, finding that only 0.3% of 10- to 21-year-olds were assigned an International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9) code suggestive of injury caused by assault, and only 0.8% of youth were assigned an ICD-9 code suggestive of risk for violence involvement. Without better information about the needs of adolescent patients, providers will not be able to formulate or refer to appropriate interventions for their at-risk adolescent populations.
The focus of this article is to describe the extent to which providers document violence risk among their adolescent patients in accordance with the AAP’s recommendation of the role of health care in addressing youth violence. We were also interested in comparing the documentation practices in private practice versus that of academic providers.
Methods
Sample and Study Design
The study took place in 2 primary care clinics located in a diverse urban setting, in 2006: one academically based adolescent medicine practice with an existing electronic medical record and one general community-based pediatric practice without electronic medical records. The clinic sites were selected to represent a range of socioeconomic, racial, and ethnic diversities and were situated in the same geographic area, half a mile apart. Youth 11 to 17 years of age, attending their primary care clinic for a routine or sick visit, and their parents were invited to participate. Because of consent issues, patients with significant developmental disabilities were excluded. Written informed consent was obtained from parents, coupled with written assent from youth. The research assistant (RA) used a standardized, written script to explain the study. For youth attending the clinic alone, verbal consent from parents was obtained by phone. The study was approved by the Colorado Multiple Institutional Review Board. Analysis of the data was completed in 2012.
To minimize selection bias, every other youth meeting inclusion criteria on the clinic schedule on any given day was selected. The RA reviewed the daily schedule at each site before the clinic began and approached each patient to invite him or her to participate after registration for their visit. As part of the consent process, the RA explained that if they reported any suicidal or homicidal intent, or abuse/maltreatment, confidentiality would be broken and appropriate personnel notified. Once consent/assent was given, participants completed a confidential, self-administered, paper-and-pencil survey after enrollment in the waiting room. They began the survey before their clinic visit with their provider. Some youth finished surveys before their visit, whereas others completed it after the visit. Results were not shared with their health care provider at any point in the clinical interaction. A chart review by the RA, evaluating documentation of any violence-related characteristics was performed 4 weeks after the visit.
Instruments and Measures
The primary outcome, documented reference to any level of violence involvement in the chart note by the PCP was determined by chart review approximately 4 weeks after the baseline visit. The RA was trained by the principal investigator to use a chart abstraction tool to identify any patient-provider discussion or reference to violence. We documented any violence-related discussion, regardless of whether the comment reflected whether youth were violent or nonviolent. The chart abstraction tool guided the RA in identifying any discussion or reference to violence and was divided between the subjective section of the chart, the assessment, and the plan. Some providers separate assessment and plan when documenting the chart note, whereas others combine the sections. For the subjective section, any reference to violence involvement, such as fighting, anger issues, aggression, bullying, or injuries from violence were noted. For the assessment/plan (A/P) section, any diagnosis related to aggression, anger, assault, or violence was recorded as well as any topics discussed, such as anger management, harm reduction, or bullying prevention. Treatment or referrals for violence-related issues, including violence-specific agencies, counseling, or medication, was recorded. We also captured notation of any discussion or diagnosis of mental health issues in either the subjective or A/P part of the chart. Finally, we examined ICD-9 codes to assess whether an actual diagnosis of violence-related behavior was assigned. We recorded any ICD-9 code related to fights (E960) assaults (E961-968), aggressiveness (301.3), conduct disorders (312), and others to capture a broad range of possible violence-related ICD-9 codes.
Current violence involvement was determined by youth self-report, using a 7-item scale developed and validated in the National Longitudinal Study on Adolescent Health that measures violence perpetration and injuries related to violence (VPIA).13,14 Any positive response to one of the questions was coded “yes” for violence perpetration or injury (Table 1). Cronbach’s α for the VPIA = .83. Youth also filled out several additional scales related to violence and mental health. For the purpose of this study, we used single items to describe certain violent behaviors, including the number of physical fights, number of fights in which youth suffered injuries, and number of injuries that required medical attention. We also created 2 measures to determine physically violent perpetration and physically violent victimization. Physically violent victimization included answering positively to one of the following questions within the past year: (1) Have you gotten into a fight where you were injured and had to be treated by a doctor or nurse? (2) Were you hurt in a fight? (3) Did you need medical care for an intentionally caused injury? (4) Did someone beat you up? and (5) Did someone slap or kick you? Physically violent perpetration included scoring one or higher on the following behaviors in the past year: (1) having hit or punched someone, (2) kicked someone, (3) hurt someone else in a fight, and (4) used a knife or gun on someone.
Patterns of Chart Documentation of Violence Present: Violence-Involved versus Non–Violence-Involved Youth
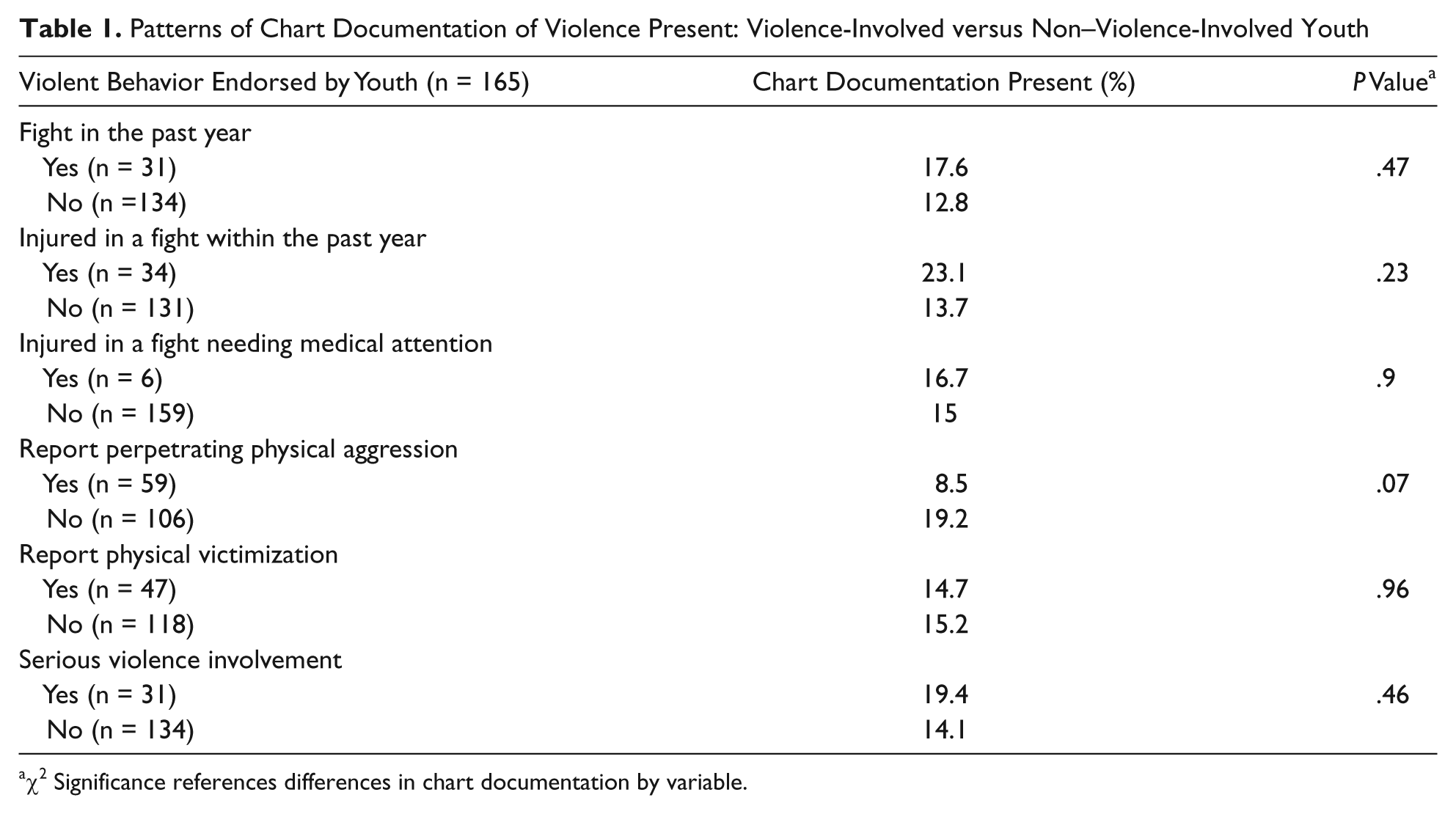
χ2 Significance references differences in chart documentation by variable.
Analytical Plan
Descriptive statistics reveal baseline characteristics of the youth. Reported rates of violence perpetration and victimization were based on self-report from the survey. Provider documentation of violence involvement was calculated as rates separately for both the subjective and A/P parts of the medical record and then combined to provide a total rate of any documentation of violence involvement. Association between youth self-report and practitioner documentation was determined to assess whether actual youth behavior was consistent with chart documentation of violence discussions. χ2 Analysis was used to determine if any youth characteristics were associated with violence involvement documentation by the practitioner. Based on literature documenting that 20% of youth are expected to have been involved in serious violent events in the past year and an assumption that PCPs assign a violence-related diagnosis 0.8% of the time, we projected needing data on 30 violent youth to have 80% power to detect a difference between PCP documentation and youth self-report at the α = .05 level. Logistic regression examined which factors in the bivariate analyses were associated with the primary outcome—chart documentation of any violence discussion.
Results
Sample Characteristics
The 2 clinics were staffed by 17 health care providers who, in turn, served 165 youth who met eligibility criteria and consented to participate (82% consented). The average age of the youth was 14.5 (standard deviation = 1.7); additional demographic characteristics are given in Table 2. The academic adolescent practice patients were older, and there was a higher percentage of Hispanic and publicly insured youth among them. The general pediatric practice had a higher percentage of white, privately insured youth. The general practice had a higher percentage of visits for physicals (55% vs 40%) compared with the adolescent practice. Overall, 53% of participants were from the academic practice and 47% from the general pediatric practice.
Demographic Characteristics
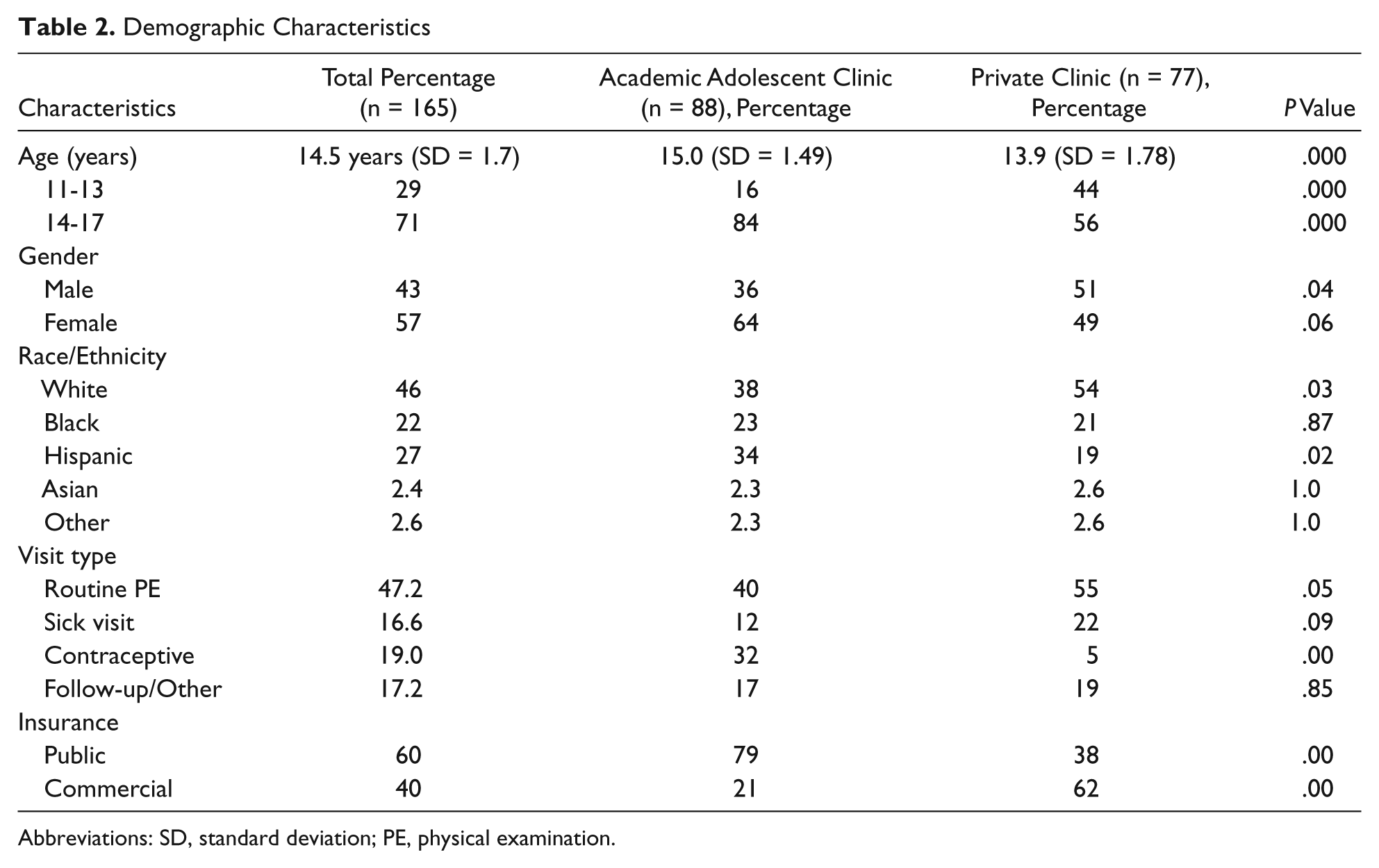
Abbreviations: SD, standard deviation; PE, physical examination.
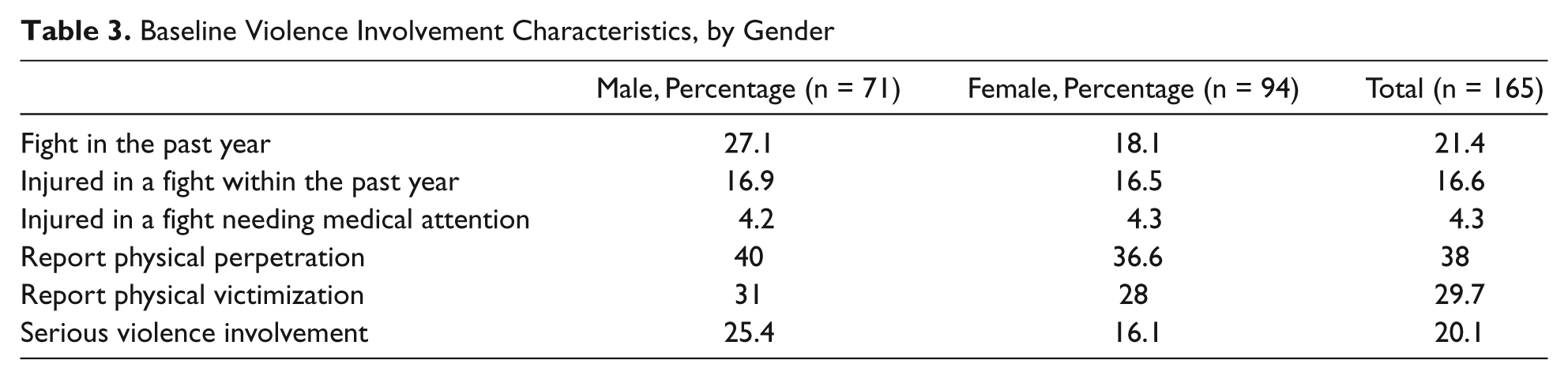
Youth-reported violence involvement was substantial, with male and female participants reporting similar rates (Table 3). Among all patients, 23% reported being involved in a fight in the past year; 13.6% were injured in a fight, and 3% were injured in a fight and needed medical attention. Overall, 19.6% screened positive for current (past year) violence perpetration or injury based on the VPIA; of these, 25% were male and 16% female. Physical violence perpetration was reported by 37% overall, and 30% reported being physically victimized.
Baseline Violence Involvement Characteristics, by Gender
Providers’ Reports of Violence Involvement
Providers documented violence involvement in 9.9% of all patients in the subjective part of the chart, documented aggression/fighting/violence risk in the A/P 10.6% (n = 17/165) of the time, and used an ICD-9 code reflecting any type of violence involvement only 0.6% of the time. Overall, 14.5% of charts revealed any reference to violence involvement. There was no relationship between youth-reported violence involvement and documentation of violence issues in the chart (Table 1). For the 20.1% of youth who reported serious violence involvement, the practitioner documented discussion of violence issues only 19.4% of the time. For the 79.9% who did not self-report violence involvement, practitioners documented discussion of violence issues 14.1% of the time. Provider documentation of violence issues was evaluated for several types of violence involvement. In all, 30% of youth reported being physically victimized in the past year, but only 15% of those reporting victimization had any violence-related documentation in their charts. Similarly, 3.8% reported being injured in a fight that required medical attention, but in only 15% of those injured was there provider documentation. Overall, there were no differences in provider documentation of having addressed violence based on whether youth reported being violent or not.
In only 1 instance (0.6%) was there a specific violence-related diagnosis made. For the 15 cases in which there was reference to violence in the A/P, all were for counseling done by the provider. Counseling topics included weapons (5.8%), handling anger (1.8%), harm reduction (5.4%), and avoiding violence (1.2%). There were no referrals, interventions, or follow-up for any violence-related issues documented.
Providers were more likely to document violence issues if the patient was of minority race (19.2% vs 6.9%), having public (or no) insurance (24.2% vs 1.5%, P < .001), and if the visit was for a routine checkup versus all other visit types (family planning, sick visits, follow-up visits; 22.7% vs 8.2%). The charts from the adolescent practice were more likely (28.2%) to include documentation of violence-related discussion than those from general pediatric practice (1.3%).
There was a relationship between the subjective section and A/P in terms of violence documentation. If documentation of a violence-related topic occurred in the subjective section, there was documentation of violence counseling 50% (P < .001)of the time in the A/P. If a violence topic was not documented in the subjective section, then only 6.2% of the time was violence referenced in the A/P. This relationship was independent of whether or not the adolescent endorsed any type of violent behavior. Insurance status contributed to violence documentation as privately insured patients had violence referenced only 1.5% of the time compared with 23.2% for publicly insured patients.
We did find an association between documentation of mental health issues and violence. Overall, 30.4% of charts had documentation of assessing mental health issues regardless of whether a patient was diagnosed with mental health problems. If there was documentation of mental health issues, we found 43% of the charts had documentation of violence characteristics, compared with 6.2% without documentation of mental health issues (P = .000). Multivariable logistic regression showed that 3 factors—documentation of mental health assessment, odds ratio (OR) = 14.6 (95% confidence interval [CI] = 3.1-68), having public insurance, OR = 19.3 (95% CI = 1.8-201), and having a routine physical exam, OR = 5.6 (95% CI = 1.3-24)—were associated with documentation of violence involvement. Clinic site and race/ethnicity did not predict documentation of violence behaviors (Table 4).
Odds of Provider Documenting Violent Behaviors
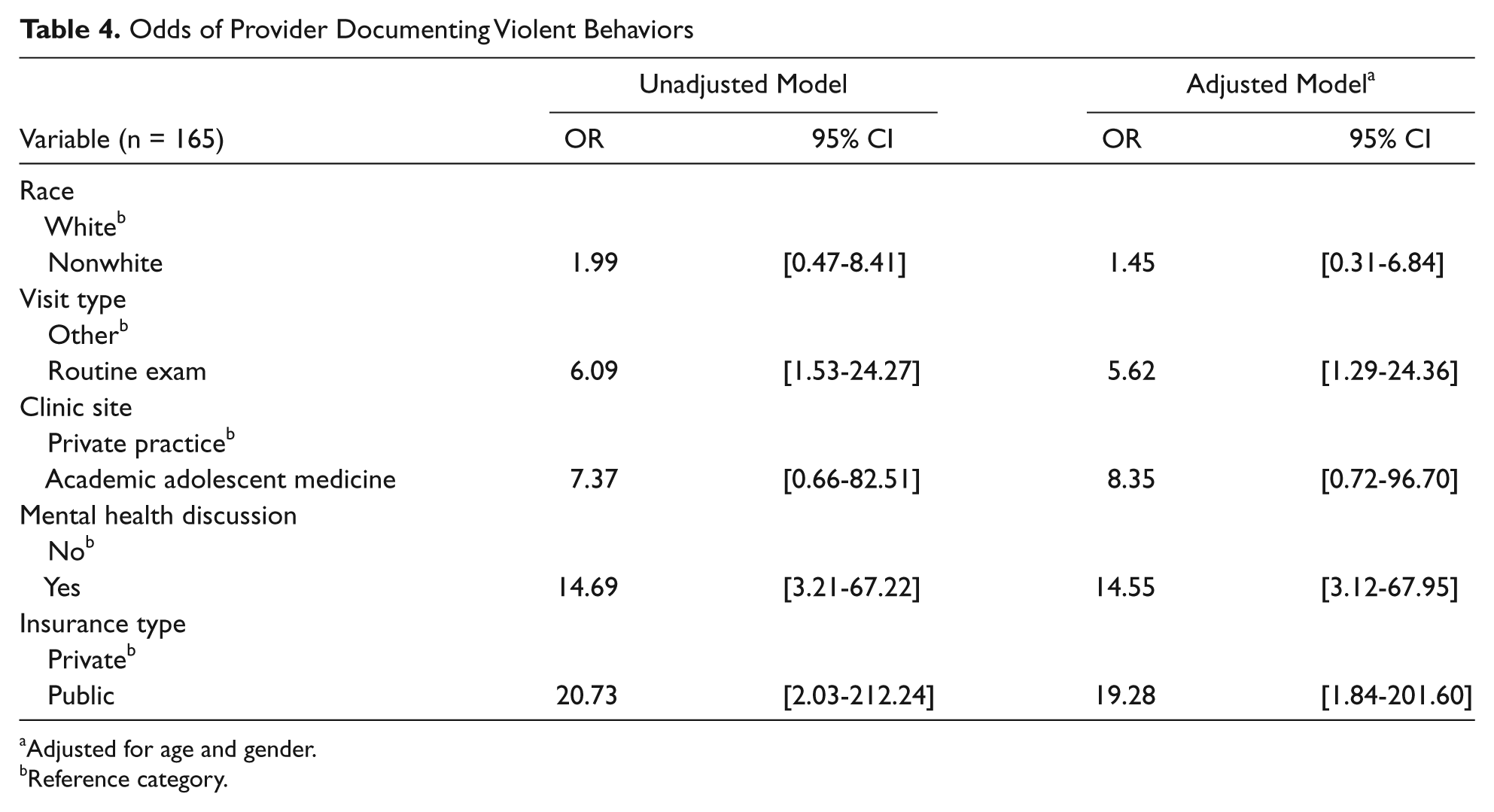
Adjusted for age and gender.
Reference category.
Discussion
Both the AAP, in 1999 and again in 2009, and the AMA, in 2002, have encouraged health care providers to address youth violence by screening, recognition, and referral.7-9 Guidelines for Adolescent Preventive Services (GAPS), issued by the AMA in 1994, 15 lists 5 violence-related screening questions to be assessed annually, and Bright Futures 16 lists violence and injury prevention as one of 4 priority issues to focus on in early, middle, and late adolescence. However, despite these guidelines and the overall prevalence of youth violence, even providers with expertise in adolescent health care are not recognizing patients who are involved in violence. Using chart reviews, we assessed the documentation by physicians of addressing violence in the patient encounter and found documentation in less than a quarter of visits for routine physicals and only slightly more than a fifth of encounters in which the patient self-reported violence perpetration. Similarly, for the 29.7% who self-reported being physically victimized in the past year, there was no documentation of discussion of violence in more than 85% of the encounters. Assuming the lack of documentation reflects attention to violence issues in the patient encounter, it suggests that clinicians are not addressing violence with the patients they see. Furthermore, according to our chart review, even those patients whose physicians discussed violence received no intervention or referral to address their violent behaviors apart from in-office counseling, leaving them vulnerable to the serious sequelae of violence.
It was interesting to discover that if mental health issues were documented in the subjective section, it was more likely that there would also be some documentation of violence-related issues. Though we cannot determine which concern was initially raised, the association may mean that if a mental health concern is raised, practitioners are prompted to inquire about violence-related behaviors. Conversely, if violent behaviors are discussed, this may prompt the provider to address mental health issues. This is encouraging regardless of which concern may be initially raised, indicating that providers may be making a link between mental health and violence.
Also, the correspondence between documentation of violence-related issues in the subjective part of the chart and the provider addressing the topic of violence in the assessment and plan suggests that once violent behaviors are discussed initially (subjective), providers are much more likely to consider plans for addressing violence issues and noting them in the A/P. Improving methods to help providers remember to address violence issues, such as prompts in the electronic medical record, or implementing violence risk screening may lead to increased rates of documenting violence involvement and providing subsequent interventions. Having more time for each patient visit, as is the general case for academic practices, as well as expertise in exploring the risk behavior syndrome also may have contributed to the increased documentation rate at the adolescent clinic site.
Limitations and Strengths
This study has several limitations. One, we report on what is documented and not on all that may have been discussed. Two, evidence about adolescent violence experiences rely on self-report only; however, we have no reason to believe that youth would overrepresent their violence experiences. Estimates of violence, if anything, are likely conservative. Three, it reflects the practices of only 2 clinics, and a relatively small number (n = 165), which limits generalizability.
Despite the limitations, this study is one of the first to examine provider behaviors in addressing youth violence in the clinical encounter. By using independent assessment of youth violent behaviors and physician record keeping using a standard protocol, biases associated with clinician awareness of their recording practices being studied were minimized.
Conclusions and Implications
Documentation of youth violence remains limited in the primary care setting, likely reflecting that physicians are paying inadequate attention to these issues. We demonstrate that youth at high risk for violence are not being recognized in the primary care setting. To make the health care setting a better venue to address youth violence, a framework is needed to help the busy practitioner detect violence perpetration and victimization. Using a validated violence risk screen may facilitate recognition of risk behavior. 17 Using templates embedded in the electronic medical record that include reference to fighting, for example, may prompt providers to ask specific questions and/or make it easier to record patient behavior.
Footnotes
Acknowledgements
We gratefully acknowledge the support from the Colorado Injury Control Research Center, the CDC Center for Injury Control and Prevention’s K award mechanism (CE001332-02), Children’s Hospital Colorado’s Research Institute, and the guidance of mentors Jean Kutner, MD, MSPH, Allison Kempe, MD, MPH, and Carol Runyan, MPH, PhD.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Colorado Injury Control Research Center and the Center for Disease Control and Prevention supported the study.