
Abstract
Asthma is the most prevalent chronic condition affecting children and a common chief complaint in emergency departments (EDs). We aimed to improve parents’ understanding of their child’s asthma severity on accessing our pediatric ED for an acute asthma exacerbation. A retrospective chart review was conducted to determine outpatient follow-up rates from our ED in 2010-2011. In an attempt to educate parents at ED discharge about their child’s asthma severity at presentation, we included a visual severity scale on their discharge instructions. Postdischarge telephone interviews were completed to determine postintervention follow-up rates. Asthma follow-up rates at 1 week improved from 20.8% to 50% after intervention. This difference was statistically significant after controlling for age and clinical asthma score with logistic regression (P < .0001). Offering predischarge education about a child’s initial asthma severity is a simple intervention that significantly improved follow-up rates for children seen in the ED for asthma exacerbation.
Introduction
Asthma is the most common chronic condition affecting children. It affects more than 10% of American children and contributes to nearly 2 million emergency department (ED) visits annually in the United States. 1 The National Heart, Lung, and Blood Institute’s (NHLBI) 2007 guidelines for the management of acute asthma exacerbations recommend asthma follow- up within 1 to 4 weeks after an ED visit for acute asthma. 2 Adhering to these guidelines has contributed to lower morbidity among children and prevented relapse or recurrent exacerbations, thus decreasing return ED visits.3-5 Despite this, reported rates of post-ED follow-up for acute asthma exacerbations remain poor, ranging from 7% to 52%.6-10 Follow-up is particularly low in urban populations who are at high risk for asthma morbidity.11-13 In a previous cohort study done at our institution, 76% of the patients who presented to our pediatric ED visit for an acute asthma exacerbation in 2007-2009 were of a minority race, and 12% of the study population presented for outpatient follow-up. 14
Several studies have identified factors associated with increased likelihood of follow-up after an ED visit for acute asthma exacerbation. Patients were more likely to follow up after a recent hospitalization if they had more than 1 ED visit for asthma in the past year, if the parents believed that their child had “very severe” asthma, and if the child had daily use of a controller medication.7,8 Barriers to and beliefs about asthma follow-up have also been evaluated, and a commonly cited barrier to follow-up was difficulty accessing their primary care provider (PCP).7,15-19
The purpose of this study was to improve parental understanding of their child’s asthma severity at the time of presentation to the ED for an acute asthma exacerbation. We hypothesized that the addition of a visual asthma severity scale to our asthma discharge instructions and an explanation of their child’s severity at presentation provided to parents by a medical provider at the time of discharge would lead to an increase in pediatric ED asthma follow-up rates.
Materials and Methods
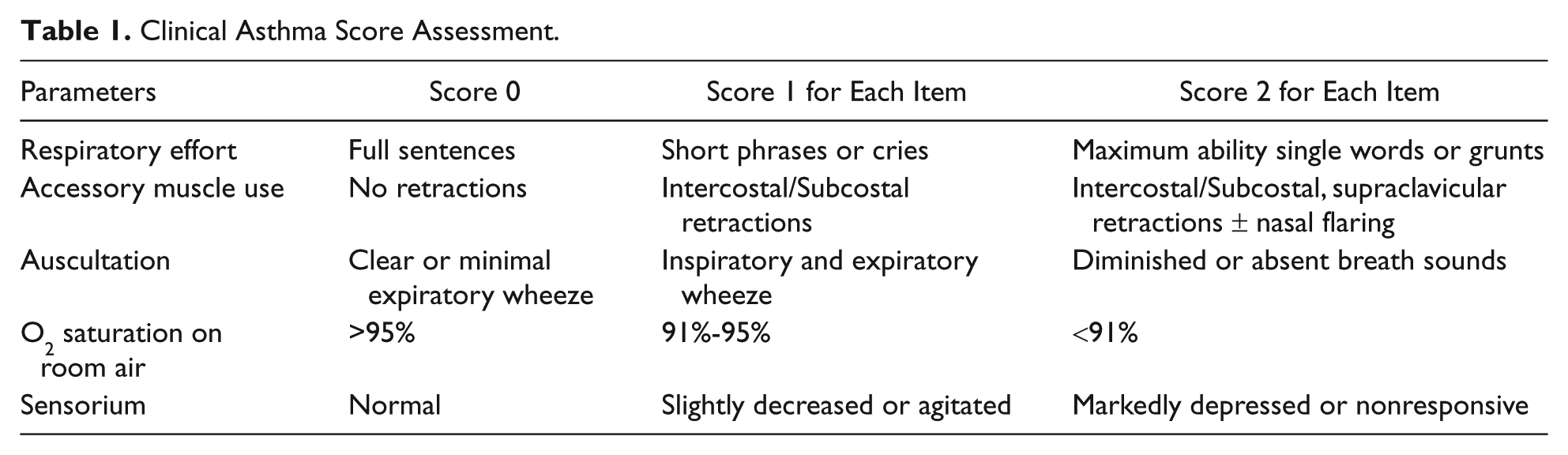
Our study involved 3 key components: a preintervention retrospective chart review, implementation of a new discharge handout that included a visual severity scale of the child’s initial clinical asthma score (CAS, Table 1), and a postintervention telephone follow-up interview. The study was reviewed and approved by our internal review board at the Medical University of South Carolina (MUSC), a tertiary care academic pediatric hospital.
Clinical Asthma Score Assessment.
We initially conducted a retrospective chart review of pediatric patients who presented to our urban pediatric ED (annual census of approximately 24 000) with an asthma exacerbation between January 1 and December 31, 2010. Charts were selected based on primary discharge diagnosis coding of asthma using International Classification of Diseases, 9th Revision (ICD-9) codes 493.00-02, 493.10-12, 493.20-22, 493.8, 493.9, and 786.07. From this group, we excluded all patients who listed their PCP as outside of the MUSC health care system because the patient records of a possible follow-up visit would not be viewable in our electronic medical record. We also excluded all charts that did not document initial CAS on presentation to the ED. This resulted in a total of 216 patients for our final analysis.
For each electronic chart, we collected 4 main variables: initial asthma score (0-9), patient age, patient disposition (eg, discharged home, admitted to floor, or admitted to the pediatric intensive care unit [PICU]), and PCP data. Our primary outcome variable was attendance at an outpatient asthma follow-up visit within 1 week and 1 month of the ED asthma visit. To assess attendance, we used the electronic medical record to verify a documented clinic visit that addressed asthma follow-up from our pediatric ED.
Prior to our intervention, our ED’s routine asthma care, provided primarily by our respiratory therapists, included education on prevention and management of asthma exacerbations, including education on inhaler technique, recognizing environmental triggers, understanding the child’s asthma action plan, and the importance of outpatient follow-up. At discharge, a nurse reiterated the discharge instructions handout, which includes medication instructions and recommended follow-up. For our intervention, we modified our ED asthma discharge instructions handout to include visual and numerical representations of each patient’s initial CAS (Figure 1). Additionally, we had the ED clinical provider explain the child’s initial asthma score to the parents prior to discharge from the ED. The goal of this intervention was to improve parental understanding of their child’s asthma severity at the time of presentation to the ED for an acute asthma exacerbation. Carbon copies of the completed asthma discharge handout, which documented the child’s age, initial CAS, and discharge medications (including new ones), were collected. The handout also included a request for parental consent to allow the study investigators to telephone the guardian to conduct a short survey within a week of the patient’s evaluation in the ED. The handout was approved by the MUSC forms committee and the institutional review board (IRB), and parents had the right to refuse participation in our study.

Visual asthma severity scale added to our ED asthma discharge instructions.
Postintervention telephone surveys were administered to parents of previously diagnosed children with asthma who presented to our pediatric ED with a mild to moderate acute asthma exacerbation from December 2011 to May 2012. Patients seen for wheezing who were not previously diagnosed with asthma were excluded. Study surveys were conducted if the patient was between the ages of 1 and 17 years and their parent consented to a follow-up telephone call. The survey was developed by the study investigators and the language approved by the IRB. The survey included 5 short questions designed to identify factors that may have contributed to the parental decision on whether or not they attended an outpatient asthma follow-up visit after their ED asthma visit (Figure 2). Additionally, if a patient was unable to follow up, we asked an open response question to identify the reason for the lack of a follow-up visit.
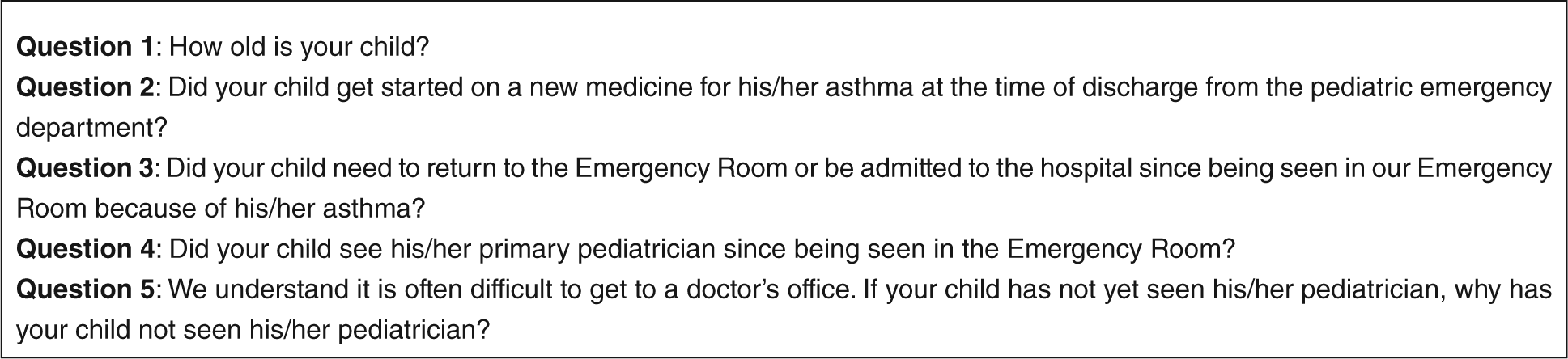
Questions asked on telephone follow-up.
For the preintervention and postintervention analyses, we calculated response frequencies for all variables and survey questions. We used χ2 tests to compare characteristics between patients who attended an outpatient asthma follow-up visit and those who did not. Additionally, in our preintervention secondary analysis we used χ2 tests to determine if there was an association between age, CAS, and ED disposition (ie, home, floor, or PICU) and attendance at an asthma follow-up visit. In our postintervention secondary analysis, we used χ2 tests to determine if there was an association between age, CAS, the start of a controller medication in the ED, and a necessary return ED visit and attendance at an asthma follow-up visit. Using logistic regression to control for age and CAS, the difference in asthma follow-up rates at 1 week were compared before and after the intervention. All analyses were performed using JMP 10 (SAS Institute, Cary, NC). Statistical significance was defined as P < .05.
Results
Our retrospective chart review yielded 264 children with asthma who presented to our pediatric ED for an acute asthma exacerbation and listed their PCP as within MUSC’s health care system between January 2010 and December 2011. Of these patients, 48 were excluded from our evaluation as a result of incomplete CAS documentation at the time of ED presentation, which resulted in 216 patients for our analyses. The mean age (±standard deviation) of patients at presentation to the ED was 7.14 ± 4.40 years, with a median age of 7 years; 47% were 1 to 6 years of age, 37% were 7 to 11 years of age, and 16% were 12 to 17 years of age. The mean CAS at presentation to the ED was 2.88 ± 1.98, with a median CAS of 3.
Approximately 21% of our patients, by medical record documentation, followed up with their MUSC PCP within 1 week (n = 45). Among these patients, the mean age was 5.96 ± 3.90 years, and the mean CAS was 3.33 ± 2.13. Of the patients who did not follow up within a week, the mean age was 7.37 ± 4.63 years, and the mean CAS was 2.56 ± 1.77 (Table 2). Using a Wilcoxon rank-sum test, these 2 populations were not statistically significantly different from one another with respect to the mean age or CAS (P = .06 and .12, respectively). Patients who followed up were younger than those who did not follow up.
Comparison of Patients Who Followed Up Versus Those Who Did Not in Our Retrospective Cohort.

Abbreviation: CAS, clinical asthma score (defined in Table 1).
Using a Wilcoxon rank-sum test.
Approximately 36% of our patients, by medical record documentation, followed up with their MUSC PCP within 1 month (n = 77). Among these patients, the mean age was 6.71 ± 3.95 years, and the mean CAS was 3.45 ± 2.21. Of the patients who did not follow up within a month, the mean age was 7.45 ± 4.49 years, and the mean CAS was 2.76 ± 1.93 (Table 2). Using a Wilcoxon rank-sum test, these 2 populations were not statistically significantly different from one another with respect to the mean age (P = .43). The groups were statistically significantly different from one another with respect to the CAS (P < .01). Patients with a higher CAS were more likely to follow up at 1 month.
Of the patients included in our retrospective chart review, 82% were discharged home, 13% were admitted to the general pediatric floor, and 5% were admitted to the PICU. Those patients discharged home had a mean age of 7.44 ± 4.34 years and mean asthma score of 2.42 ± 1.71. The patients admitted to the general pediatrics floor had a mean age of 4.67 ± 3.51 years and mean asthma score of 4.75 ± 2.01. The patients admitted to the PICU floor had a mean age of 8.36 ± 5.57 years and mean asthma score of 5.45 ± 1.29.
Out of the 177 patients who were discharged home from the pediatric ED, 17% had documented asthma follow-up within 1 week of their ED visit, and 29% had documented follow-up within 1 month of their ED visit for an acute asthma exacerbation.
Of the patients with asthma who were admitted to the general pediatrics floor, 50% attended an asthma follow-up visit within 1 week of their ED visit and 64% attended within 1 month. The children with asthma who were admitted to the PICU had follow-up rates of 9% and 64% at 1 week and 1 month, respectively.
For our postintervention assessment of asthma follow-up, a total of 100 asthma discharge instructions were collected in the MUSC’s pediatric ED from December 2011 to May 2012. Of these patients, 30 were excluded from our analysis for the following reasons (Figure 3): failure to consent (3), inadequate documentation (11), and unable to reach by phone (16). The mean age of patients at presentation to the ED was 5.14 ± 3.80 years, with a median age of 4 years; 66% were 1 to 6 years old, 27% were 7 to 11 years old, and 7% were 12 to 17 years old. Bivariate analysis revealed no statistically significant association between age of the child and attendance at a follow-up visit (P = .86).
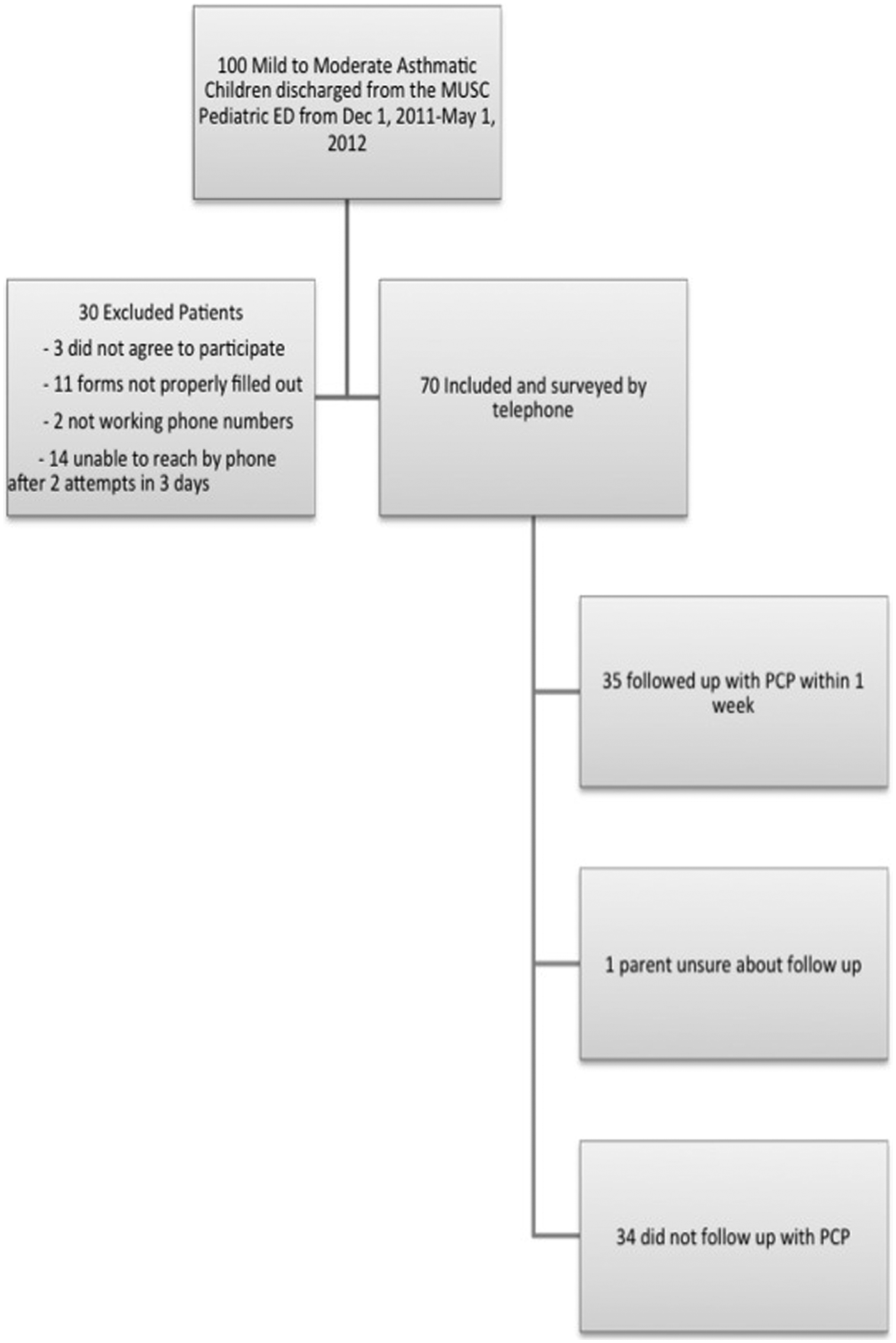
Postintervention study population flow diagram.
In our postintervention analysis, the mean CAS of patients at presentation to the ED was 2.81 ± 1.76, with a median CAS of 3. Bivariate analysis revealed no statistically significant association between CAS and attendance at follow-up visit (P = .76).
By parental report, 50% of the children with asthma included followed up with their PCP within 1 week (n = 35). Among these patients, the mean age was 4.89 ± 3.88 years, and the mean CAS was 2.86 ± 1.88. Among the patients who did not follow up within a week, the mean age was 5.44 ± 3.82 years, and the mean CAS was 2.79 ± 1.67. These 2 populations were not statistically significantly different from one another (P = .50 for mean age; P = .84 for mean CAS).
Of the 70 surveyed patients, 3 (4.3%) had not yet seen their PCP for follow-up and had a necessary return ED visit for asthma within 1 week from previous ED discharge. These patients had a mean age of 3.67 ± 2.08 years and a mean CAS of 4.33 ± 3.06. We found no statistically significant association between return visit to the ED and attendance at an asthma follow-up visit (P = .79).
Approximately 24% (n = 17) of our surveyed patients were started on an inhaled corticosteroid during their acute asthma exacerbation pediatric ED visit. These patients had a mean age of 5.12 ± 4.04 years, and the mean CAS was 2.82 ± 2.04. The mean age and CAS of the patients who were started on an inhaled corticosteroids were not statistically significantly different from those of patients who were not started on this new asthma medication (P = .98 for mean age; P = .76 for mean CAS). Approximately 53% (9/17) of the patients who were started on an inhaled corticosteroid for their asthma followed up with their pediatrician within 1 week. We found no statistically significant association between whether the patient was started on a new asthma medication and attendance at an asthma follow-up visit (P = .21).
The mean age of the children with asthma seen in our ED in 2010-2011 was statistically significantly different from the mean age of the children with asthma seen in our ED in the period December 2011 to May 2012 and who consented to participate in our study (P < .01), as determined by the Wilcoxon rank-sum test. The mean CAS of the patients with asthma seen in our ED in 2010-2011 was not statistically significantly different (P = .98; Table 3) from that of the patients who consented to participate in our study in the period December 2011 to May 2012.
Comparison of Patients Who Presented to Our ED With an Acute Asthma Exacerbation From January 2010 to May 2012.
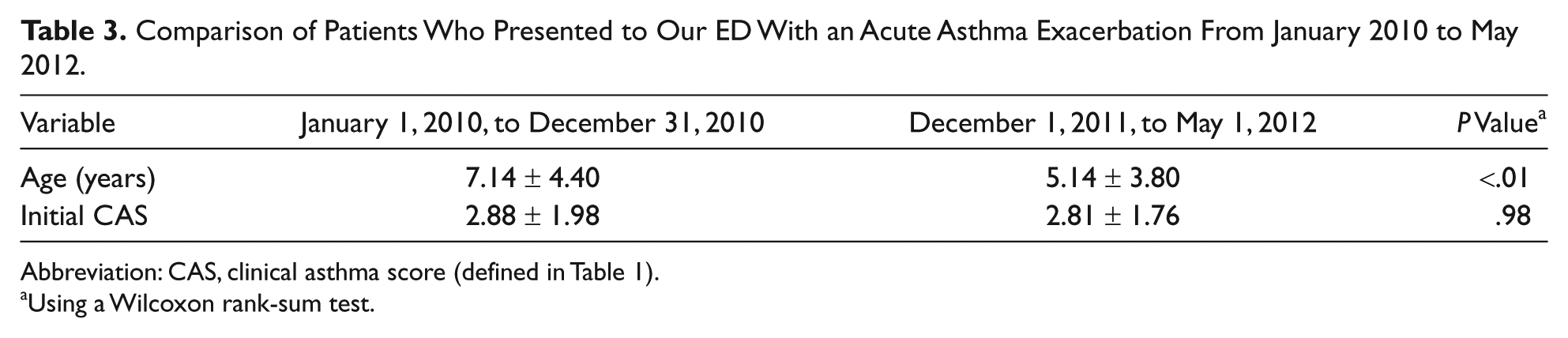
Abbreviation: CAS, clinical asthma score (defined in Table 1).
Using a Wilcoxon rank-sum test.
Asthma follow-up rates at 1 week improved from 20.8% to 50% after the intervention. After controlling for age and CAS with logistic regression, patients who received the educational intervention were more likely to attend an outpatient asthma follow-up visit at 1 week compared with those who did not (P < .0001).
Parents cited multiple reasons for failed attendance at an asthma follow-up within 1 week. Of the patients who did not follow up, 43% of their parents stated that they made an appointment for their child, but there were no available appointments within a week from ED discharge. Also, 6% of parents made an asthma follow-up appointment within a week of ED discharge but were unable to keep the appointment. Approximately 29% of parents had not yet attempted to make an appointment. Of these, parental work was a commonly cited reason for why they had not yet made the appointment. We found that 6% of parents stated that their child was no longer sick and did not need a follow-up appointment.
Discussion
Our study demonstrated that a simple educational intervention emphasizing a child’s asthma severity at presentation to the ED increased outpatient follow-up rates when compared with a similar group of children with asthma who presented to our ED the year prior to our intervention implementation. This difference in asthma follow-up was statistically significant after controlling for both age and CAS.
Our retrospective chart review revealed a low baseline 1-week follow-up rate following an acute asthma exacerbation ED visit (20.8%), despite predischarge asthma education that was already in place. This was comparable to that observed in previous studies.6-10 Because of this, our ED was an ideal setting for our quality improvement–driven intervention.
As the NHLBI 2007 guidelines for the management of acute asthma exacerbations recommend, clinicians should provide their patients with an ED asthma discharge plan and asthma education prior to discharge from the ED. 2 Wolf et al 20 conducted a Cochrane Database Systematic Review that included 3706 children and adolescents with asthma and concluded that self-management education interventions were effective at improving lung function, decreasing morbidity, and decreasing health care use (eg, ED visits and hospitalizations). To further characterize the education that should be provided in the ED, Sockrider et al 21 showed that individualized asthma education and a tailored asthma action plan provided to children and their families before discharge from the ED for an acute asthma exacerbation improved confidence in self-management of asthma and asthma-related return ED visits. With our addition of the visual severity scale and the use of clinical provider reinforcing the child’s severity at ED presentation, we have not only enhanced the recommended asthma education, but we have also shown statistically significant improvement in post-ED outpatient asthma follow-up.
It is our hospital’s policy for children who are admitted to the hospital to be discharged with an outpatient follow-up appointment established. Despite this, our retrospective chart review showed that only 39% of the patients with asthma who were admitted to the hospital followed up with their PCP within 1 week. Only 9% of those admitted to the PICU followed up within a week despite further individualized asthma education that occurred throughout their hospitalization. After 1 month, the percentage that followed up from the PICU increased to 63%. We speculate that the initial low follow-up rate was the result of a longer hospitalization and the lack of parental desire to immediately return to seek medical care.
Several randomized control trial interventions have aimed to improve follow-up with PCPs after ED visits. In 2006, Baren et al 22 provided patients with free prednisone and transportation vouchers and scheduled appointments at the time of discharge or a telephone reminder to make an appointment. Follow-up rates were higher in those with already scheduled appointments (73%) versus those with or without telephone reminders (49%). Smith et al 10 provided patients with telephone asthma coaching about the benefits of follow-up after their ED visit for an asthma exacerbation and a monetary incentive after they attended an asthma follow-up visit. Those who were coached about the benefits of follow-up were more likely to attend a follow-up visit (Relative Risk [RR] = 1.21). Lehman et al 23 prescribed a 2-week course of an inhaled corticosteroid in a pediatric ED and instructed patients to follow up with their PCP in 2 weeks to obtain a prescription. Follow-up was high with this intervention (70%). In our study, 24% of patients were started on an inhaled corticosteroid for their asthma, and 53% (9/17) of those patients followed up with their pediatrician within 1 week. Our rate of inhaled corticosteroid initiation is comparable to that documented in other pediatric EDs8,13,24 as well as in a retrospective cohort study from our pediatric ED from 2007 to 2009 (18%). 14
Several of these aforementioned interventions required a significant amount of time and money to implement, making it difficult to replicate in a typical ED environment. Our study required minimal cost to the ED and could easily be reproduced at other institutions. Based on our data, it is impossible to determine whether the increase in follow-up rate was a result of the visual severity scale indicating asthma severity or of the time the medical provider spent educating parents on their child’s asthma severity at the time of presentation to the ED.
With regard to elucidating possible barriers to asthma follow-up from the ED, our study findings were consistent with that of Zorc et al, 7 in that the most prevalent reason for lack of follow-up was the inability to obtain a timely outpatient appointment. Additionally, the belief that their child had recovered and no longer needed the appointment was evident. Mansour et al 18 found that parents of urban, minority children with asthma were concerned about the use, safety, and long-term complications of the medications; the impact of limitation of exercise on their child’s quality of life; and their own quality of life. Similarly, parents from the study by Leickly et al 19 expressed doubts regarding the usefulness and concerns about the side effects of medications prescribed at ED discharge. In our urban population, neither of these concerns was raised by our study population’s parents.
This study has several limitations. We were unable to verify by electronic medical record the parental reported attendance of our patients’ asthma follow-up visit in our postintervention analysis. Because our method of determining follow-up was not the same in the preintervention and postintervention analyses, there may be a different set of biases. There was also an absence in assessment of 1-month post-ED follow-up in the postintervention analysis. We obtained the retrospective cohort of patients based on ICD-9 codes, which could contribute to some inaccuracy in identifying patients. The preintervention and postintervention study populations were not the same people; however, we assumed that the children with asthma who visit our ED from year to year were comparable. A larger sample size with a normal distribution of ages and longer data collection would have strengthened our study. Obtaining more details related to why parents chose to follow up would have better assessed the barriers to and beliefs regarding outpatient asthma follow-up. Finally, the use of a validated survey would have strengthened our study.
Conclusions
A simple and inexpensive intervention of educating parents on their child’s asthma exacerbation severity at ED discharge improved outpatient asthma follow-up rates with PCPs. Outpatient asthma follow-up visits play an important role in patient education and self-management of asthma. Whether or not this simple intervention can also reduce ED return visits and hospitalization and improve asthma morbidity or quality of life has yet to be determined. The most prevalent reported barrier to follow-up was the inability to obtain an appointment within a week from discharge from the ED. PCPs should consider partnering with the ED to facilitate timely follow-up after an acute asthma exacerbation discharge from the ED.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.