
Abstract
Objective. To describe parent/caregiver reasons for attrition from tertiary care weight management clinics/programs. Study design. A telephone survey was administered to 147 parents from weight management clinics/programs in the National Association of Children’s Hospitals and Related Institutions’ (now Children’s Hospital Association’s) FOCUS on a Fitter Future II collaborative. Results. Scheduling, barriers to recommendation implementation, and transportation issues were endorsed by more than half of parents as having a moderate to high influence on their decision not to return. Family motivation and mismatched expectations between families and clinic/program staff were mentioned as influential by more than one-third. Only mismatched expectations correlated with patient demographics and referral patterns. Conclusions. Although limited by small sample size, the study found that parents who left geographically diverse weight management clinics/programs reported similar reasons for attrition. Future efforts should include offering alternative visit times, more treatment options, and financial and transportation assistance and exploring family expectations.
Introduction
Obesity now affects 17% of US children and adolescents. 1 Effective treatment to reduce obesity and reduce or prevent its comorbidities is available through pediatric tertiary care weight management clinics and programs throughout the United States 2 as well as through ongoing clinical trials, 3 though the need outpaces these limited resources. One particularly significant barrier to obesity treatment is attrition of patients and families. A recent review of attrition in pediatric weight management programs noted that the literature on this topic is scant and that published rates of dropout ranged from 27% to 73%, with the majority of programs reporting rates >50%. 4
Attrition has negative implications on multiple levels. On the program level, as several authors have pointed out, attrition decreases the cost-effectiveness of an already expensive and poorly reimbursed intervention.4,5 Institutional (often a pediatric tertiary care hospital) support may be jeopardized because these interventions typically rely heavily on underwriting of program costs by host hospitals. Treatment staff who have invested time and energy in assisting patients and families with lifestyle change may feel personally rejected or feel that their efforts have not had an impact on those who leave the program. A recent survey of pediatric tertiary care weight management clinics and programs described the multiple efforts made by staff to engage patients prior to the initial visit and retain them in treatment. 6 On the individual level, when treatment is discontinued, patients’ weight status and comorbidities may worsen, putting them at even higher risk for adverse physical and emotional health consequences.
Several studies have investigated demographic correlates of patient attrition, and mixed findings have been reported.7-12 Whereas some investigators found that children who were older, more severely obese, African American, and Medicaid recipients had higher attrition rates, other investigators’ findings did not support these correlates. Only a few published studies have reported parental perspectives on contributors to attrition. Consistent themes include program cost and poor insurance coverage,8,10 scheduling difficulties, 10 and the child’s wish to discontinue treatment.8,12 Only 2 studies8,13 reported parental suggestions to improve the program; help with insurance problems was the most common suggestion. In their literature review of attrition in pediatric weight management programs, Skelton and Beech report an “urgent need to study the interaction of families with treatment programmes to determine what contributes to dropout.” 4
In 2008, the National Association of Children’s Hospitals and Related Institutions (NACHRI is now known as the Children’s Hospital Association) convened a multidisciplinary discussion group on childhood obesity treatment (FOCUS on a Fitter Future I) and brought together representatives from 16 geographically diverse children’s hospitals with established or emerging obesity treatment programs to address critical issues in this field. FOCUS on a Fitter Future I (2008-2010) identified program attrition as a major barrier to program success and reported perceived reasons for attrition and approaches to increase clinic/group program retention from the perspective of program staff. 6 Cognizant of the important role that parents play in their child’s treatment success, the second group (FOCUS on a Fitter Future II, 2010-2011) sought to investigate the reasons for clinic/program attrition from the direct perspective of these stakeholders. The current study sought to determine parent/caregiver (hereinafter referred to as parent) reasons for clinic/program attrition, communication with clinic/program staff around the time of the child’s attrition, and recommendations for clinic/program modifications that might have led to retention.
Methods
Semistructured Survey Development
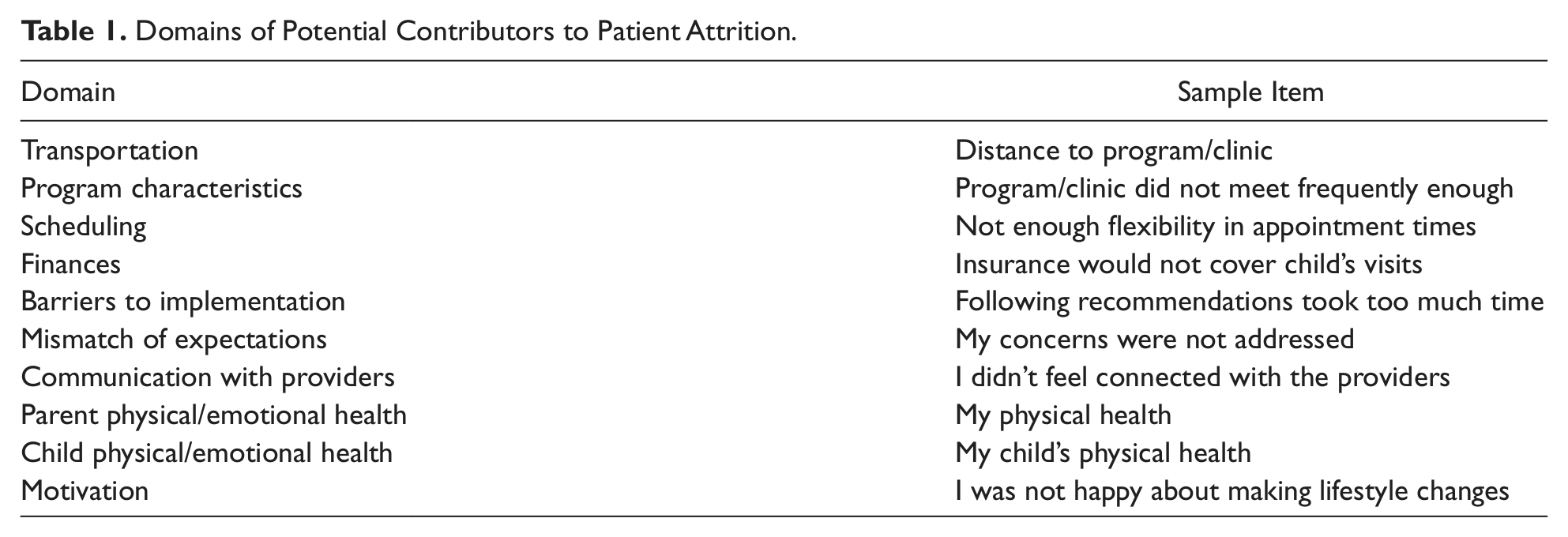
The semistructured survey was developed by 2 of the coauthors (ER and BJS) and designed to assess factors that contributed to families discontinuing participation in pediatric obesity clinics or group programs. The survey was designed as a telephone interview and was informed by a related survey contributed by Cincinnati Children’s Hospital Medical Center as well as a review of the literature and clinical experience. The 2 coauthors generated a list of factors that may contribute to attrition and created a Likert scale ranging from a lot to not at all with 2 additional options of don’t know and not applicable. This list of factors was presented to the larger group for suggestions. Consensus was reached regarding a final list of 48 factors that may contribute to attrition. These factors were grouped into 10 domains (Table 1). Open-ended questions were included to allow parents to describe (1) conversations their family had with the clinic/program about discontinuing participation, (2) what the clinic/program could have done to retain their family, and (3) features of a clinic/program that would work best for their family. Qualitative analysis of the open-ended questions will be presented in a separate report. The survey was designed for a seventh-grade reading level. The survey was formatted onto a teleform to enable transmission to the data coordinating center (Rainbow Babies and Children’s Hospital).
Domains of Potential Contributors to Patient Attrition.
Participants
Participants are each defined as the parent/guardian of a child between 2 and 18 years of age who, as a new patient, attended a clinic or program at one of the participating sites between June 1, 2009, and February 1, 2011. Inclusion criteria specified that the child had not been seen within 6 months of the first clinic appointment or had attended less than 25% of the program sessions. Parent and child had to be fluent in English or Spanish. Participants were recruited between June 2011 and September 2011 from 13 sites participating in FOCUS on a Fitter Future II (see the appendix). One additional site participated but was unable to recruit any eligible participants. The Joint Pediatric institutional review board (IRB) of the University of Nebraska Medical Center/Children’s Hospital and Medical Center (Omaha, NE) was the IRB of record for 5 participating sites; 8 additional sites obtained independent approval by their own IRBs.
Data Collection
The survey was conducted via telephone interview with eligible participants by research staff from each participating site. Interviews in Spanish were facilitated by Spanish translation of the survey provided by Florida Hospital for Children and the use of bilingual interviewers or certified translators. A subset of interviews at each site was either audiorecorded or monitored by a second staff person for quality control purposes. The child’s height, weight, and demographic data, including race/ethnicity and insurance status, were abstracted from the clinical record. BMI-for-age percentile and z score were calculated based on reference standards of the Centers for Disease Control and Prevention. These data were collected on a Microsoft Excel spreadsheet.
Completed surveys were scanned and e-mailed or faxed to the data coordinating center where they were compiled in a Microsoft Access database, along with the demographic and clinical data above. Data were all submitted to NACHRI (now Children’s Hospital Association) for analysis.
Statistical Analysis
Descriptive data are presented as means with standard deviations or proportions, as appropriate. To summarize the responses to the questions into the influence of each domain, the answers to each question were summed into a total score based on points assigned to the Likert scale response (ie, a lot = 3, a little = 2, not at all = 1, and don’t know = 0). Each domain (eg, transportation) was then recategorized based on the total score split into tertiles as “no/low influence,” “moderate influence,” and “high influence.” The number of questions differed in each domain; the cut-points for the tertiles varied with the domain. Because of small numbers, moderate- and high-influence categories were combined for bivariate analyses. The χ2 test and ANOVA were used to evaluate the association between patient or program characteristics and the influence of the 10 identified domains on attrition. A P value <.05 was considered significant. SPSS version 19 (SPSS Inc, Chicago, IL) 14 was used for analyses.
Results
Study Sample
A total of 147 parent/guardians were interviewed, with a range of 3 to 29 respondents contributed per site. Of these, 6% completed the interview in Spanish, and the majority of respondents were mothers (87%). Characteristics of the patients are summarized in Table 2. Overall, patients were significantly obese (mean BMI z score = 2.4 ± 0.5), but the population represented was diverse with respect to race/ethnicity and insurance coverage.
Study Sample Characteristics.
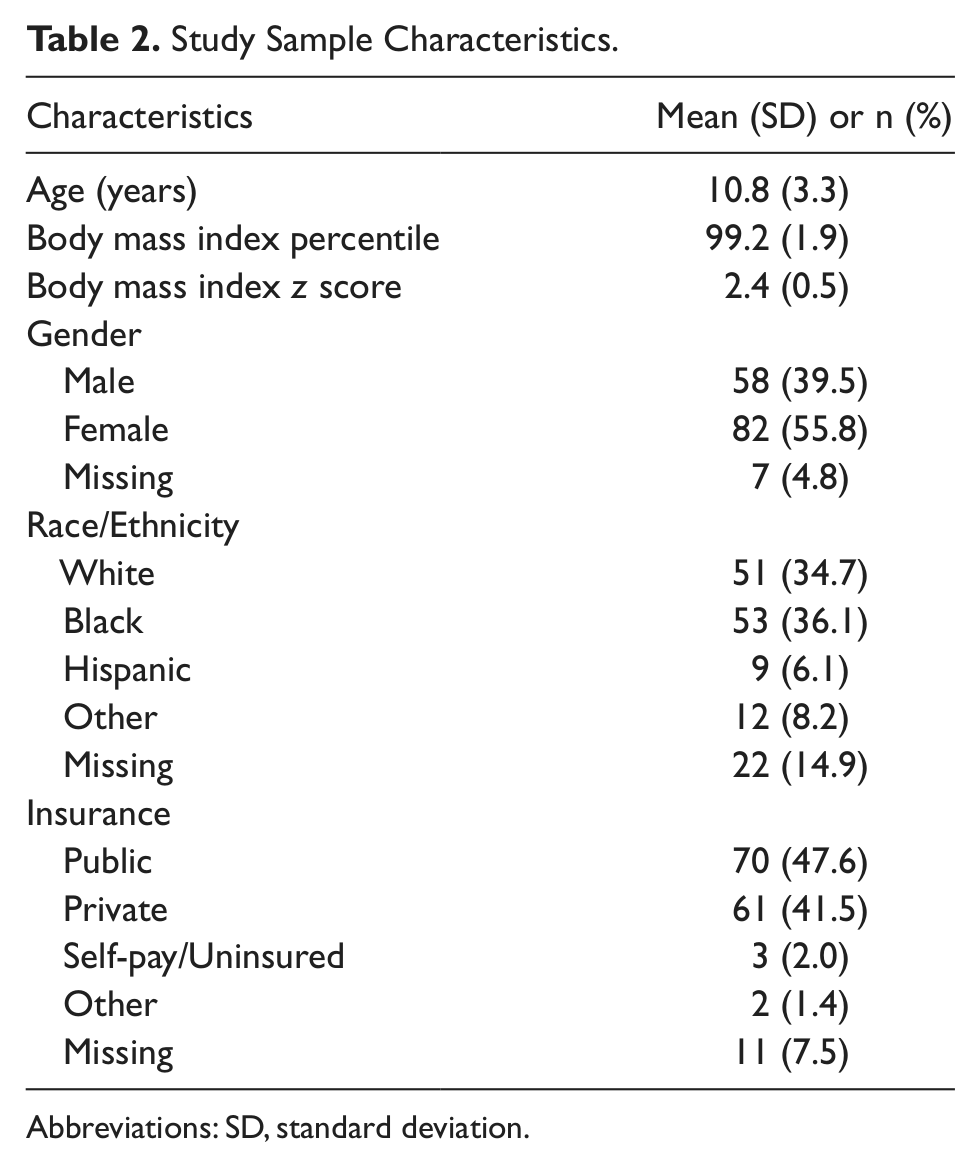
Abbreviations: SD, standard deviation.
Program and Referral Characteristics
The majority of patients were seen in clinics (56%) rather than programs, and 33% reported that the program/clinic offered rewards for participation. Most patients were referred to the pediatric weight management program or clinic by their doctors (74%), and of these, 92% of respondents agreed that their children needed to come. Most respondents felt that the program or clinic was for both the child’s weight and health (81%) and slightly more than half (53%) felt that they participated “a lot.”
Factors Influencing Attrition
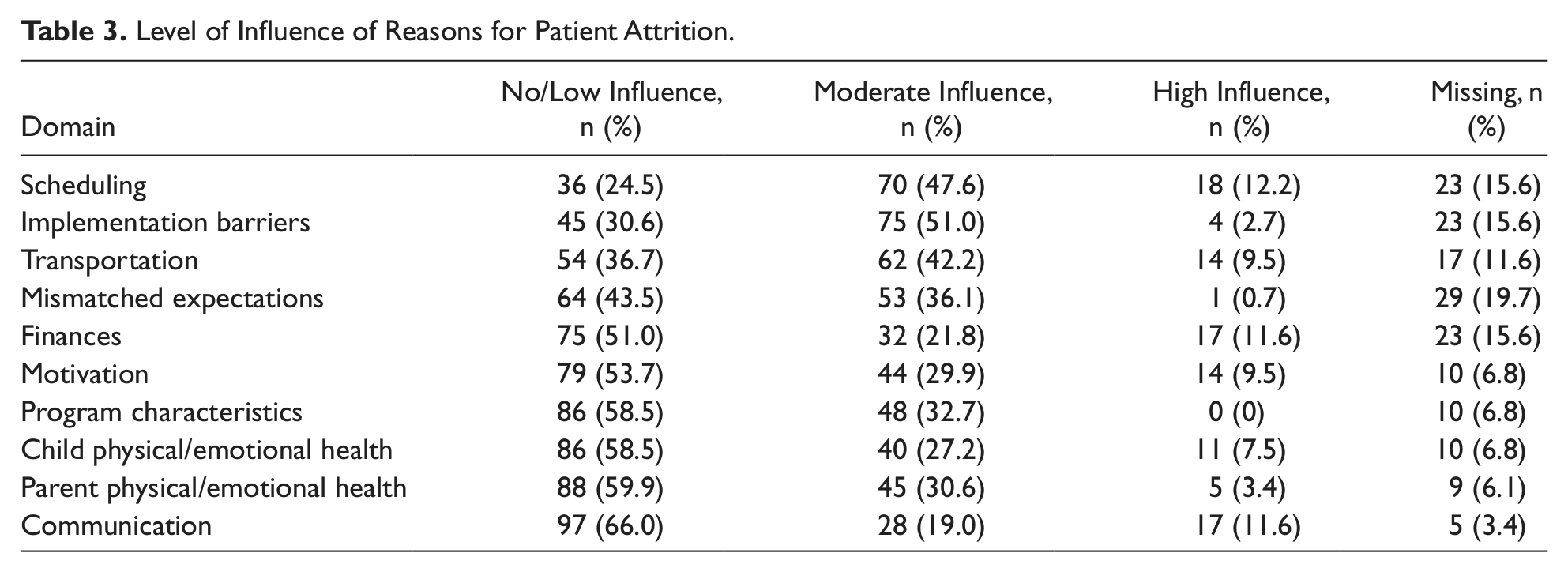
Of the 10 domains assessed, scheduling was the single domain identified most often as having a high influence on the decision not to return to tertiary care weight management clinics/programs (12.2%). Scheduling, barriers to implementation, and transportation problems were identified as having a moderate or high influence on the decision not to return for at least 50% of respondents (Table 3). Scheduling was reported as having a moderate or high influence on this decision for 59.8% of respondents, whereas implementation barriers and transportation problems were reported as having moderate or high influence by 53.7% and 51.7% of respondents, respectively. Patient/family motivation and mismatched expectations were the areas with the next highest proportion of respondents (39.4% and 36.8%, respectively) attributing a moderate or high influence of these domains to their decision not to return.
Level of Influence of Reasons for Patient Attrition.
In bivariate analyses, mismatched expectations having a moderate or high influence on the decision not to return was found to be significantly associated with a number of program and respondent characteristics. Specifically, these characteristics included respondent insurance (commercial insurance 62.5% vs all other 33.3%, P = .003), race/ethnicity (white 64.1% vs nonwhite 36.7%, P = .008), program or clinic type (clinic 52.5% vs program 32.7%, P = .04), and program/clinic offering of rewards for participation (rewards not offered 60.9% vs offered 22.2%, P < .0001). Patients referred by a physician were also more likely to indicate that transportation had a moderate/high influence on their decision not to return compared with self-referrals (63.5% vs 42.4%, P = .03), and respondents from clinics were significantly more likely to indicate a moderate/high influence of finances on their decision not to return (51.5% vs 29.8%, P = .005). There were no significant relationships between child’s gender, age, or BMI z score with any of the 10 domains.
Discussion
Given the heterogeneity of program structure at different sites and differences in patient population, it is challenging to clearly identify consistent predictors of attrition. Indeed, a systematic review of 61 adult studies published before May 2011 did not find a consistent, positive link between typical correlates such as demographics, pretreatment weight, psychological behaviors, or comorbidity profile and treatment attrition. 15
This study’s results suggest that clinic/program scheduling was the contributor that was most often mentioned as a reason for patient attrition. Kitscha et al 13 found similar results, with reported reasons for nonreturn for their clinics being scheduling, parking, and location along with organizational barriers (environment of the clinic) and program content. Scheduling barriers reported in this study included appointment times that did not work and desire for more flexibility in appointment times. Many clinic appointments are during the daytime hours, meaning children would miss school and parents would miss work to attend. Many parents may feel obesity is not a “disease” and, therefore, may be less willing to miss school/work for treatment than for other conditions that are perceived to be more of a health issue. The majority of families in this study were referred by their doctor, rather than families who sought weight management services on their own, which may mean that they were less inclined to recognize the health implications of obesity. Clinics and programs may consider offering additional weekend and/or evening hours for greater appointment flexibility; however, it can be challenging to provide staffing to cover evening/weekend programming.
The average wait time between appointments in a prior study of similar pediatric weight management clinics was 2 months. 6 For weight management, which requires sustained support and commitment to be successful, the wait time between appointments constitutes a significant barrier even for a highly motivated family. The Hampl et al 6 study found that 49% of pediatric obesity clinics have a dedicated scheduler for the clinic, and most programs utilized a system of reminder calls and/or letters to improve patient engagement in the program. Weight management clinics/programs may consider these factors when evaluating staffing resources to offer greater flexibility and more frequent appointments for families to keep them engaged. In a review of attrition from their program, Cote et al 8 noted that items that would facilitate return to treatment included reminder phone calls and flexibility of appointment scheduling.
Factors related to transportation were also found to exert a major influence on attrition. These factors included the distance to the clinic or program as well as cost and availability of transportation. Distance was the most often mentioned transportation-related factor having a high influence on the decision to leave the clinic/program, although because of the multisite nature of the study, it is difficult to determine when distance from the program or clinic becomes a barrier. Distance may have more impact in rural rather than urban settings, for example. Given the heterogeneity of sites with respect to geographic settings and patient demographics, we can draw limited conclusions about what the cost of transportation entails. Costs may be related to use of public transportation (ie, bus, subway, or cab fares) or may be related to the cost of gasoline for personal automobiles. Further studies looking at specific costs of transportation and distance from the programs or clinics are needed to identify specific barriers related to transportation.
The results suggest that implementation barriers had a high level of influence in a family’s decision not to return for services. In this study, questions related to implementation barriers included the following: “Recommendations were not practical,” “Following recommendations took too much time,” “I felt overwhelmed with the recommendations,” and “My child’s stress level due to the program or clinic requirements.” Clearly, more research is needed regarding implementation barriers for obesity treatment programs, though this study provides some initial findings. Furthermore, there are several clinical implications. First, it will be important for weight management programs to tailor interventions, as much as possible, to each individual family. Recommendations should be customized to the structure and resources of a family rather than being broad general requirements. For example, making a recommendation of purchasing fresh fruits and vegetables may be difficult for families who live in an area with limited access to grocery stores. In addition, given concerns with families feeling overwhelmed or feeling that recommendations take too much time, discussions with families should consider how recommendations can be implemented in the home, perhaps breaking recommendations down into smaller, manageable steps. For example, whereas most recommendations call for families to reduce screen time to less than 2 hours, this may not be immediately achievable when their current viewing time is 5 or 6 hours. It might be more feasible for families to be asked to reduce to 4 hours, then 3 hours and so forth. Furthermore, recommendations may need to be prioritized, with only 1 or 2 given at each visit to avoid families feeling overwhelmed with many goals to achieve. It is critical that clinics/programs invest time in checking on families’ progress and feelings regarding the program. What may seem simple to clinic/program staff may not be so simple for families. Having a team member whom families can contact when they are struggling or have a question may be of great help, and phone calls between appointments may be helpful in problem-solving barriers that arise.
An important finding for future retention efforts was parents’ endorsement of mismatched expectations between themselves/their child and clinic/program staff for the outcome, content, and/or delivery of the intervention. Several researchers have identified this as a primary barrier, resulting in families not adhering to recommendations or dropping out of a treatment program.6,16 Mismatched family and clinic/program expectations were more likely to be associated with attrition for families in clinics than in programs. This may be related to programs typically having greater structure and possibly more communication about what to expect at each session (eg, schedule of topics and similar format of weekly program sessions—exercise, education, and goal setting). Similarly, mismatched family and clinic/program expectations were more likely to be associated with attrition for parents who reported rewards not being offered. The process of earning rewards usually involves setting a goal first. This presents an opportunity to enhance communication between providers and families and collaboratively identify important target behaviors, which may decrease mismatched expectations. These results highlight the need for clear communication between families and providers. Finally, referring providers should inquire about financial and transportation issues prior to referring families to weight management clinics/programs because these issues can be significant barriers to retention.
The strengths of this study design include a systematic approach used for conducting the phone interviews, clearly defined patient inclusion criteria adhered to by all participating programs, comprehensiveness of interview content, and broad geographical representation of participating programs. These factors contributed considerably to the high quality and validity of the data collected. Though some clinic/program and patient characteristics were associated with reported reasons for attrition, other covariates such as site-specific response rate, clinic/program design, size and years of operation could be explored with a more comprehensive study. In addition, access to a larger sample size of respondents could help in more definitively identifying the factors affecting attrition.
Despite geographic diversity, parents of children who prematurely discontinued pediatric tertiary care weight management clinics/programs endorsed similar reasons for attrition. To improve retention rates, clinic/program staff and supporting hospital administration should consider scheduling alternative times for visits, offering a diverse menu of treatment recommendations, breaking recommendations down into manageable goals, and assessing families’ transportation and financial needs. Ensuring that parental/child expectations are assessed early in the treatment process and that clinic/program features are discussed alongside these expectations is also recommended. Improved patient retention and, ultimately, improved health outcomes may result.
Footnotes
Appendix
Acknowledgements
The authors thank Stacy Biddinger, MPA (Children’s Hospital Association), Kimberly Avila Edwards, MD (Dell Children’s Medical Center), Alicia Dixon Docter, MS, RD, CD (Seattle Children’s Hospital), Angela Fals, MD (Florida Hospital for Children), Nicole Kozma (St Louis Children’s Hospital), and Amy Schmidt, CHES (Rainbow Babies and Children’s Hospital) for their assistance with the project. The Children’s Hospital Association advances child health through innovation in the quality, cost, and delivery of care. Representing more than 220 children’s hospitals, the association is the voice of children’s hospitals nationally. Formed in 2011, Children’s Hospital Association brings together the strengths and talents of 3 organizations: Child Health Corporation of America (CHCA), National Association of Children’s Hospitals and Related Institutions (NACHRI), and National Association of Children’s Hospitals (N.A.C.H.).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The National Association of Children’s Hospitals and Related Institutions (NACHRI; now Children’s Hospital Association) was the study sponsor.
Authors’ Note
The study sponsor had no role in study design, the collection of data, or the decision to submit the manuscript for publication. A statistician supplied by the sponsor assisted with analysis and interpretation of the data, and an editor reviewed the final draft of the manuscript. The views expressed are those of the authors and do not necessarily reflect those of the Children’s Hospital Association. Dr. Rhodes’ work on this study was supported by the New Balance Foundation Obesity Prevention Center Boston Children’s Hospital.