
Abstract
Background. Injuries from bicycles is a leading cause of trauma in children. We sought to investigate the epidemiology of bicycle handlebar injuries. Methods. A retrospective analysis of bicycle trauma treated at our institution was preformed. Results. A total of 462 children younger than 17 years had bicycle trauma. Abdominal handlebar injuries, representing 9% of bicycle injuries, contributed to 19% of all internal organ injuries, and 45.4% of solid, 87.5% of hollow, 66.6% of vascular or lymphatic, and 100% of pancreatic injuries. Handlebar injuries were 10 times more likely to cause severe injury, yet more than half of the children were misdiagnosed at their initial presentation. Delayed diagnosis and longer hospital stays were observed in handlebar injuries to the abdomen. Conclusion. Physicians should be aware of the serious impact of bicycle handlebar injury to the abdomen. The mechanism alone should raise the suspicion of internal organ injury, and timely imaging and surgical consultation.
Cycling remains a popular pastime for children in Canada with three quarters of Canadian children participating in the activity.1,2 In Alberta, bicycle trauma tops the list of sport and recreational activities injuries, especially in children who do not wear helmets: They are 3 times more likely to suffer head injury in a crash and are 20 times more likely to die. To mitigate such risk, Alberta passed a law in May 2002 whereby cyclists younger than 18 years are required to wear an approved bicycle helmet. Helmet use has helped reduce the rate of head injuries by up to 54% in parts of Canada; however, cycling injuries continue to rank among the highest in injury severity among children.1,3,4 Even though assessments of fractures, lacerations, and head injuries are common practice, handlebar induced injuries may be overlooked initially because of the internal nature of the injuries with its associated insidious presentation.
Handlebar injuries have been shown to account for 10% of bicycle-related injuries.5,6 Modern bikes allow handlebars to rotate perpendicularly to the cyclists’ body. Striking the handlebars at this angle imparts localized, blunt trauma on the abdomen because of the small surface area of the handlebars that can cause serious damage to internal organs from focused distribution of force.5-9 Patients presenting with severe handlebar injuries often have a trivial history of a minor fall at low speeds and relatively little external trauma.2,5,8-10 Furthermore, many handlebar injuries lack outward signs proportional to the severity of the internal damage and tend to have a delayed presentation that can take up to 24 hours to become apparent.2,5,7,9,10 As such, severe handlebar injuries to the abdomen can be overlooked.
Timely management of handlebar-induced trauma is critical to prevent peritonitis, sepsis, hemorrhages, and other serious sequelae. 7 Physicians must maintain a high index of suspicion when dealing with patients with a history of handlebar impact and keenly observe them for signs that point toward severe abdominal trauma.2,7,10 Our study aims to draw attention to the severity of handlebar injuries to the abdomen and contribute useful information for physicians in their assessment of patients and counseling of caregivers.
Methods
After obtaining approval from our Institutional Health Research Ethics Board–Health Panel (approval study number 38558), a retrospective analysis of pediatric (<17 years) with bicycle trauma treated at our institution was done using existing complementary databases (Canadian Hospitals Injury Reporting and Prevention Program (CHIRPP) and Alberta Trauma Registry (ATR) Database as well as medical chart review by comparing epidemiology, injury, and outcomes from February 2012 through July 2013.
CHIRPP is an injury and poisoning surveillance system presently operating in the emergency departments of all 11 pediatric and 4 general hospitals across Canada.11,12 The CHIRPP system, which has been in operation since 1990, runs on an Oracle platform and currently contains about 2.2 million records (injury events). When an injured or accompanying person (parent or caregiver) presents to a CHIRPP site, they are asked by hospital staff to complete one side of a CHIRPP data collection form. The hospital staff complete the reverse side of the form with clinical data. Information collected includes activity at the time of injury, activity leading to the injury, the direct cause of the injury, contributing factors, time and place of the injury event, the patients’ age and sex, up to 3 injuries (body part and nature of injury) and the treatment received in the emergency department. Narrative fields provide information to further refine the coding and identify rare events and consumer products. All collected data are reviewed by the CHIRPP site coordinator for any missing information. Completed forms are sent to the Public Health Agency of Canada in Ottawa for entry by a trained coding team. Although only select hospitals report to CHIRPP, previous work has shown that the data collected through the program represent general injury patterns among Canadian youth. 13 Previous investigations have also reported on other methodological aspects of CHIRPP.14 -18
By accessing the complimentary ATR Database, we determined the epidemiology, injury, and outcomes for all pediatric bike traumas with severe injuries (determined as Injury Severity Score (ISS) >12) 19 treated at our institution. The ATR data were further enhanced by more information provided in the hospital medical chart in terms of specifics of treatment and outcomes.
Patients injured while fixing, walking a bike, or involved in a bicycle collision while not cycling were not included. The involvement of the health care system following the injury was analyzed. This includes the date and location of initial health care contact and number of health care visits prior to presentation at our hospital (level 1 pediatric trauma center). Presentation to our institution was defined as either an initial or delayed definitive visit. An initial visit was defined as one presenting to or being transferred to us with a prompt initial diagnosis. Delayed definitive visits were defined as those where previous health care contact resulted in a missed/incorrect diagnosis, or a premature discharge from the emergency room. The length of time between initial and delayed definitive visits, where applicable, was also noted. Vitals, laboratory and radiologic investigations and results at the initial and definitive visits were recorded.
All patients with bicycle injuries were then classified in 2 groups: handlebar and non-handlebar injured. According to the mechanism of injury, the handlebar group was further subdivided into: handlebar versus abdomen, and handlebar versus other. The handlebar versus abdomen group included only those whose abdomen made direct contact with the handlebars. All injuries resulting from handlebar contact to any other region of the body were placed in the handlebar versus other group. Statistical analysis was done using Microsoft Excel using Fischer’s exact test, with P value <.05 considered as significant.
Results
Of the 462 children injured while riding a bicycle, 71% were male with median age 11 years. In all, 76% of participants were using an unspecified bicycle, 9% were using a dirt-bike, and 11% were using a BMX bike (4% unknown). Only 55% of participants wore a helmet.
Handlebar impact accounted for 12% of all injuries, with 75% of these being handlebar versus abdomen (Figure 1). Sixty-eight percent of handlebar versus abdomen injuries occurred from a general fall, 10% from stunting, 12% from excess speed, and 5% from collisions with vehicles. Of significance, 1 out of 4 patients with handlebar injury to the abdomen presented with damage to internal organs compared with 1 in 100 of non-handlebar injuries. Furthermore, 10.9% of handlebar and only 1.2% of non-handlebar injuries had severe injuries with ISS >12.
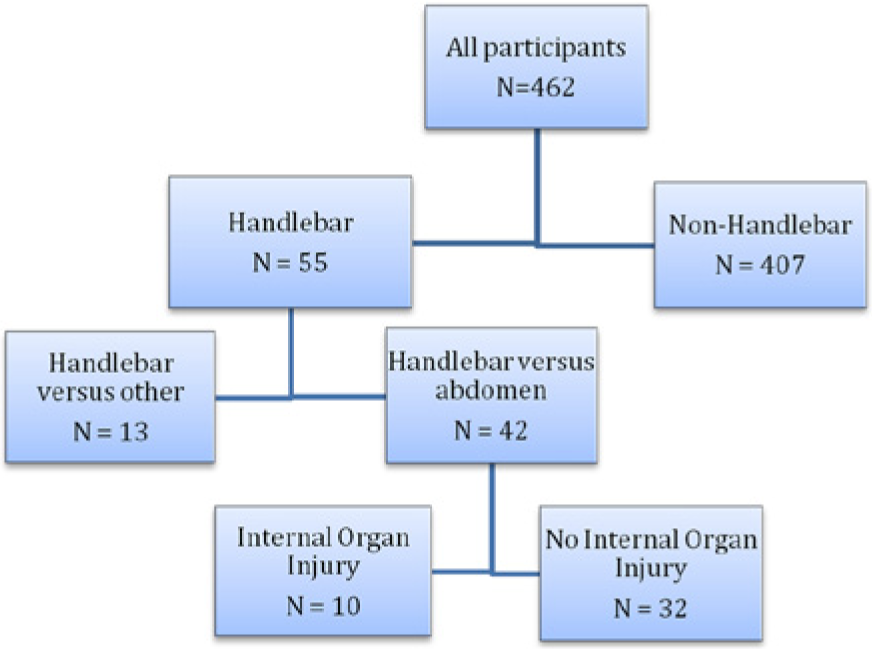
According to mechanism of bicycle trauma, participants were divided into 2 groups: those injured by handlebar and non-handlebar. The handlebar group was further divided into handlebar versus abdomen and handlebar versus other.
In the sample at large, the most common injuries include abrasions (n = 135), closed fractures of upper extremities (n = 114), and soft tissue injuries of extremities, head, and neck (n = 118). The handlebar versus abdomen group accounted for only 9% of the sample but accounted for the majority of internal visceral injuries: 45.4% of solid, 87.5% of hollow, 66.6% of vascular or lymphatic and 100% of pancreatic injuries (Figure 2).
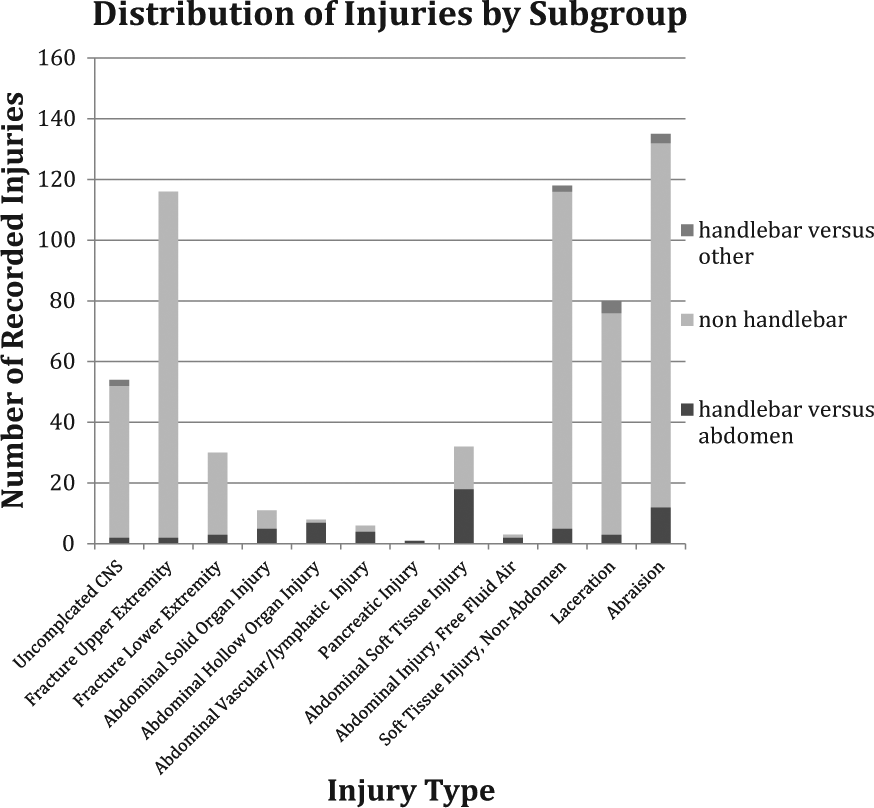
The most common injuries across the sample include abrasions, closed upper extremity fractures and soft tissue injuries of the head, neck, or extremities (CNS= central nervous system injury). The handlebar versus abdomen subgroup accounts for only 9% of the sample, yet is overrepresented in all abdominal injuries.
Of those with internal organ injuries from handle bar contact, there was a greater likelihood of presenting with fever, emesis, signs of peritonitis, and high lipase as seen in Table 1. Other laboratory results such as white blood cell count and neutrophil count, and liver enzyme levels were initially non-specific for injury. Less than half of the patients with handlebar versus abdomen mechanism of injury had diagnostic imaging at their initial visit to investigate abdominal injuries.
Initial Laboratory, Radiologic, and Clinical Investigations of Children With and Without Internal Organ Injury by Subgroup.
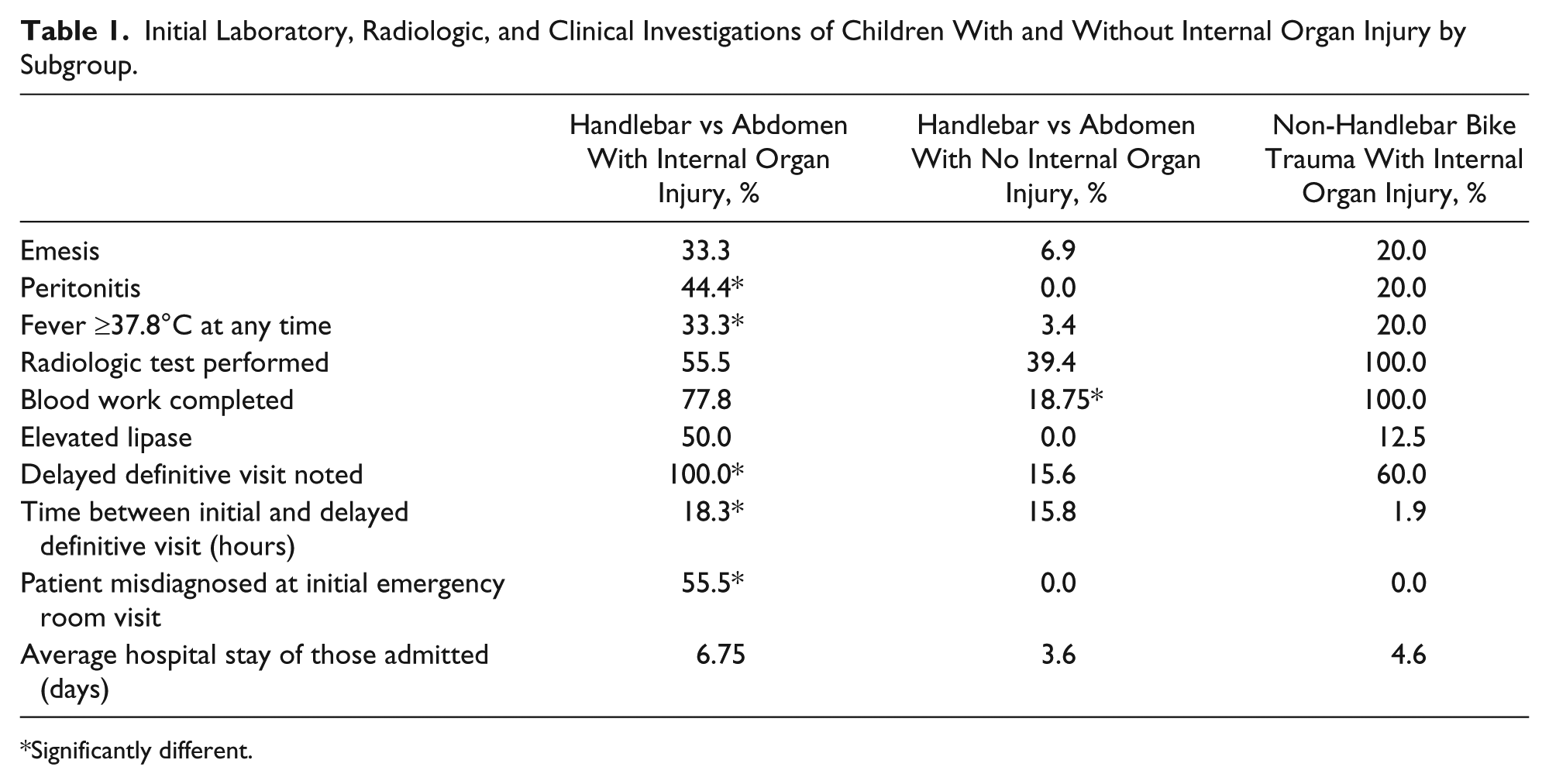
Significantly different.
More than half of the children with handle bar injuries to the abdomen had delayed definitive diagnosis (were misdiagnosed and discharged, only to come back within hours) at their initial visits. The average time between initial and definitive visits in this group was 18.3 hours. The average hospital stay for those admitted was 6.75 days.
Interestingly, of those with internal organ injury due to non-handlebar bicycle trauma, 60% had a delayed definitive visit because of transfer from a non-level-1 trauma center to our center as a level 1, and none were misdiagnosed. (Please note that on average, 60% of all our pediatric trauma patients are transferred from another facility to ours.) The average time between initial and delayed definitive visits was 1.9 hours with an average hospital stay of 4.6 days for those admitted.
Patients in the handlebar versus abdomen group with solid organ injuries such as liver/spleen/pancreatic injuries were all managed conservatively with success. The 3 patients with bowel injuries and one with vascular injuries were managed surgically. Three patients from the handlebar versus abdomen with internal organ damage subgroup were later seen for complications. Two children were admitted for 5 and 7 days for postoperative bowel obstructions from adhesions. One child was admitted for 14 days for a splenic abscess arising from their splenic injury.
Discussion
The mechanism of bicycle handlebar impact to the abdomen should raise suspicion of potential significant internal organ injury. Though often subtle at initial presentation and delayed in definitive diagnosis,2,5,8,10 our findings indicate that a significant proportion of handlebar injuries to the abdomen have an elevated injury severity score when compared with non-handlebar bicycle injuries. Handlebar to the abdomen cause the vast majority of internal organ injuries incurred while cycling.5,7,10 In our study, 1 out of 4 patients with a history of handle-bar trauma to the abdomen had internal organ damage to the splee/liver/pancreas/bowel.
In congruence with previous findings, our study suggests that clinical symptoms such as vomiting, peritonitis, or fevers are indicators of internal organ injury after blunt trauma from bicycle handlebar to the abdomen.6,10 Half of the children with internal injuries from handlebar trauma presented with elevated lipase at their initial visit, while all of the children without any internal injuries had a normal lipase.
Furthermore, the finding that more than half of the patients with internal organ injuries from handlebar impact to the abdomen were misdiagnosed initially, and discharged prematurely, only to return with frank peritonitis, reflects the subtle initial presentation, and need for initial high suspicion based on mechanism of injury and initial radiological imaging using a computed tomography scan for definitive diagnosis.5,6,10 Injuries from handlebar to the abdomen result in longer hospital stay because of a delay in definitive diagnosis, treatment, and increased severity of injuries. 10
Our study is limited as it is a single center observational research with a limited time frame. However, our study points out the severity if there is impact of bicycle handlebar to the abdomen. We are not suggesting not riding a bicycle, but consideration of safety mechanism to the handlebar may be warranted. Previous studies have recommended retractable, curved, or padded handlebars to reduce the kinetic energy imparted on the abdomen.5,8 We also recommend that industry design a device to prevent handlebars from rotating perpendicular to the body such as to reduce the direct impact of the handlebar head-on end (rotating the handlebar is often a fun “bike trick” to show off to friends).
Handlebar injuries are serious in nature and can be life threatening. Their subtle or delayed presentation and deceptively minor history can cause them to be overlooked.2,5-8,10 However, a delay in diagnosis and treatment can result in sepsis, hemorrhages, or even death. 5 Physicians should have a high index of suspicion when evaluating a child with a history of handlebar trauma to the abdomen. The mechanism of handlebar injury to the abdomen in a child presenting to the emergency room is by itself an indicator of potential severe injury and requires serial abdominal exams, laboratory investigations, and prompt computed tomography of the abdomen to rule out hollow viscus or solid organ injuries. Caregivers should seek health care if emesis, peritonitis, or fever appears following a handlebar injury. Modifications to handlebars may reduce the severity and number of injuries.
Footnotes
Acknowledgements
We would like to thank the Canadian Hospitals Injury Reporting and Prevention Program and Alberta Trauma Registry for access to their databases.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a grant from the University of Alberta Faculty of Medicine and Dentistry (Wynne Rigal Summer Research Award).