
Abstract
Sudden sensorineural hearing loss (SSHL) is defined as a unilateral or bilateral sensorineural hearing loss with at least 30 dB decrease in threshold in 3 contiguous test frequencies occurring over 72 hours or less. It is very rare in children. Sudden hearing loss is a symptom that suggests that there is a problem in the inner ear, surrounding structures, or the whole organism. The etiology and development of this disorder are still not fully understood. The literature contains numerous models of the pathogenesis of SSHL, with childhood SSHL having certain peculiarities. In practical terms, the multifactorial nature of SSHL is important in the choice of diagnostic methods and treatment methods. It is important to determine the cause and effect relationship between the underlying disease and hearing loss.
Sudden Hearing Loss in Children
Sudden hearing loss (SHL) is defined as sudden unilateral or bilateral sensorineural hearing loss, greater than 30 dB for 3 speech frequencies, that develops during a maximum of 3 days. It is rare in children. SHL is a symptom that indicates that there is a problem in the inner ear, surrounding structures, or entire body. The nature of occurrence and course of this disorder is still not fully understood. The etiopathogenesis of acute hearing loss (AHL) is complex. The child’s age has effects that significantly influence the choice of diagnostic methods and therapy.1-3 AHL in the population of children <14 years of age accounts for 3.5% of all cases of SHL. Every year, about 4000 children in the United States and about 15 000 children around the world get an AHL. 2
Etiology of SHL
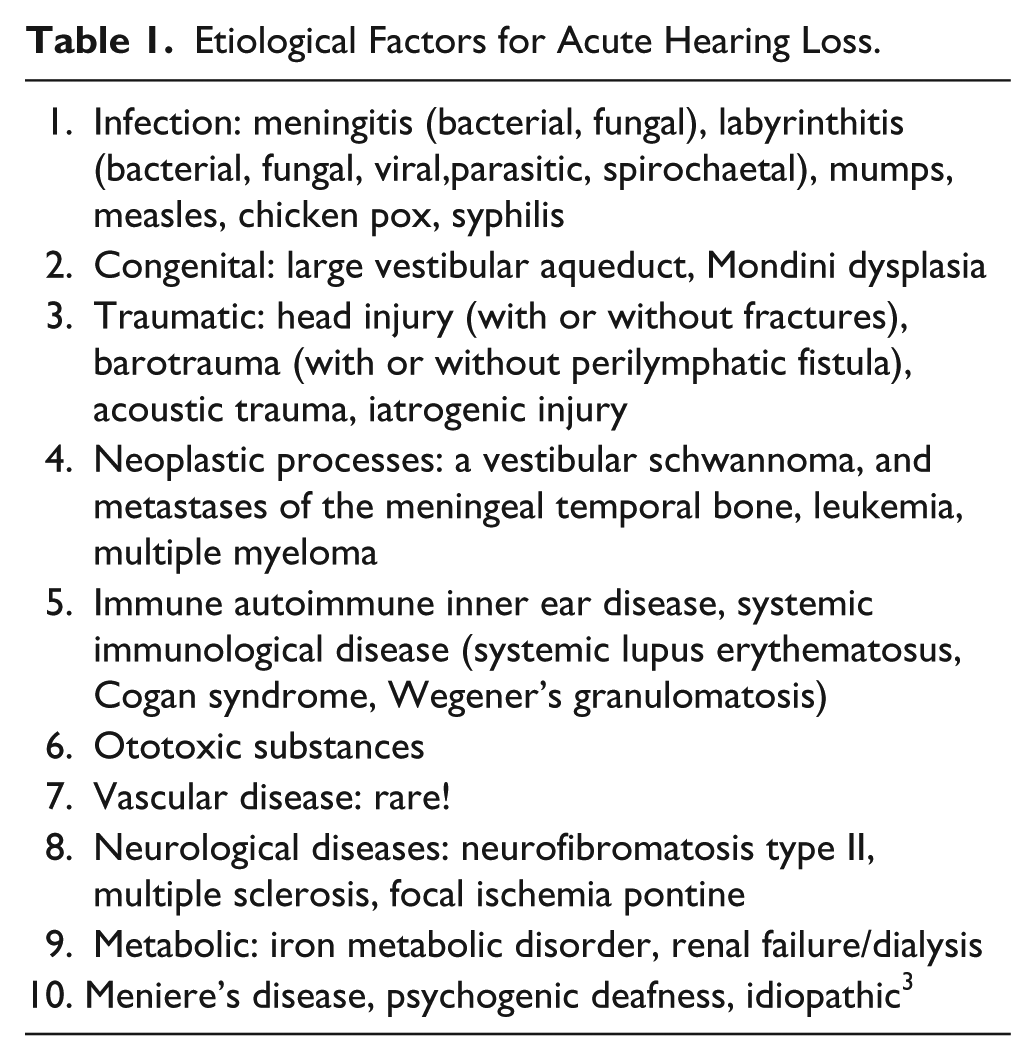
The causes of AHL can be numerous and can be congenital or acquired (Table 1). It often cannot be proved that infectious agents cause such sensorineural hearing loss, including SHL. It is not always possible to determine the time of occurrence of lesions. Audiological tests indicate the existence of a functional deficit but not the location, extent, and duration of infection. Diagnosis of diseases of the membranous labyrinth cannot be confirmed by standard radiography. Serological tests do not confirm that infections damage inner ear; if viruses or bacteria in the epipharyngeal region exist, it does not mean that they are the cause. 4 Meningitis causes very different forms and degrees of AHL. Predictors of occurrence of SHL are the severity of the clinical picture and the time of initiation of therapy. 5
Etiological Factors for Acute Hearing Loss.
Cytomegalovirus (CMV) is one of the most important infectious agents that may lead to hearing loss. The prevalence of congenital CMV infection in the population of infants is 0.4% to 7.4%. Less than 10% of the children have systemic and neurological symptoms, which are characterized by a clinical picture of CMV congenital syndromes, including 61% of hearing loss. A large number of children with asymptomatic CMV infection develop delayed hearing loss that occurs under the picture of acute or progressive disorder. In children with congenital CMV infection, further progressive hearing loss occurs in 50.5% and delayed start of hearing loss in 18.2% of children 27 to 60 months of age. 4 When CMV infection exists, it is necessary to continuously monitor the state of hearing.4,6 Although it rarely occurs nowadays, congenital rubella may cause bilateral severe to profound hearing loss.
Later in childhood, rubella can manifest as asymmetric AHL, sometimes unilateral, more severe at high frequencies.2-4 All forms of syphilis can cause hearing loss. Severe symmetrical hearing loss may be a sign of congenital syphilis. From the age of 8 to 20 years, “late congenital” syphilis is evident as a progressive fluctuating hearing loss (Hennebert’s sign of perilymphatic fistula). Acquired syphilis in the third and fourth stage may be manifested as an acute, progressive, asymmetric hearing loss. 4
In the past, acute unilateral hearing loss in childhood was most often caused by the mumps virus. This virus can sometimes cause bilateral AHL. Since the MMR vaccine was made mandatory, mumps AHL is extremely rare but can occur despite vaccination or in asymptomatic forms in children unvaccinated for mumps. The prevalence of mumps hearing loss is 5:10 000 in patients suffering from mumps. AHL caused by mumps is permanent and usually occurs between the third and seventh day of the onset of disease. 7 Diagnosis is based on clinical symptoms, elevated mumps virus antibodies, and the characteristic finding obtained by magnetic resonance imaging (MRI). Using the 3D-FLAIR technique, an amplified signal indicates increased concentration of protein in the acute inflammatory process. There is no medical therapy for SHL of this origin.8.9
In the Ramsay Hunt syndrome (herpes zoster oticus) infection affects ganglion geniculi, which complicates the clinical picture of varicella/herpes zoster infection, leading to paralysis of the facial nerve and the appearance of auricular bulls; in 6% of patients it is possible to find acute SHL. 6
Anomalies of the Inner Ear
An anomaly of the inner ear—large vestibular aqueduct syndrome—is the most common abnormality of the temporal bone in children with hearing loss of unknown cause. The diagnosis of this syndrome is radiological. It usually manifests in childhood and is bilateral and progressive. Unsteady gait may be the only symptom. Sometimes, it begins as an SHL immediately after a trauma to the head, after a loud blow from a musical brass instrument, or during air travel.
Mondini dysplasia, or dysplasia of the basal turn of the cochlea, is diagnosed radiologically, and sometimes its main clinical feature is SHL. It occurs in utero in the seventh week of gestation and is genetically conditioned. It is often associated with other anomalies of the inner ear. These patients are good candidates for cochlear implantation because the basal cochlear curve is increased, and there is no increased risk of cerebrospinal or perilymphatic fistula. Most ear abnormalities predispose one to the formation of perilymphatic fistulas that can occur on the oval or round window and in the otic capsula. Perilymphatic fistulas can be congenital or acquired.
Anomalies of the common cavity may cross the subarachnoid space in the internal auditory channel with perilymphatic endolymphatic space. This increases the risk of occurrence of cerebrospinal and perilymphatic fistulas and also labyrinthitis and repeated meningitis as a result of pathological communication. Local findings are characterized by shortened cochlear threads, dilated semicircular canals, and extended vestibule of the inner ear in 25% to 50% of patients. Manifested symptoms of unilateral or bilateral hearing loss can have an acute or progressive beginning and steady or fluctuating course. Sudden HL often occurs after mild head trauma or even barotrauma caused by the Valsalva probe. A common symptom in these patients is chronic ataxia.1-4,10
Ototoxic Influence
Ototoxic influence of some drugs can clinically present as SHL. The most toxic effects in children are a result of cisplatin use, radiation therapy, and aminoglycoside antibiotics. The most serious damage occurs during implementation of the protocol for treatment of endocranial cancerous tumors, which includes cisplatin and radiation.1-4,11
Autoimmune Inner Ear Disease
Systemic autoimmune diseases are rare in childhood. There are no specific tests or clear diagnostic criteria for the diagnosis of autoimmune inner ear disease as a separate entity. 12 Sudden HL is manifested as decreased threshold or understanding or the appearance of these symptoms associated with significant fluctuations over time. Sudden autoimmune HL should be suspected in all cases of idiopathic, rapidly progressive, bilateral devolvement, which improves after corticosteroid therapy. This mechanism of disease should be suspected when patients with suspected acute autoimmune HL later develop systemic autoimmune disease.
Psychogenic Deafness
Psychogenic deafness or pseudohypoacusis represents inorganic, functional hearing loss. It occurs in a range from mild to severe. The patients complain that they hear well or behave like that. Diagnostic procedures reveal a discrepancy between subjective and objective audiometry. Subjective audiometry shows hearing loss and objective audiometry shows normal hearing. It occurs most often between the ages of 10 and 14 years, more often in children who fall behind in psychomotor development, and it is a manifestation of psychological or emotional problems. Onset is often abrupt, after precipitating factors or without them. Treatment is based on the counseling of a psychologist. It has a good prognosis.13,14
Less Common Causes of SHL
There are some rare diseases or conditions where AHL (SHL) occurs. Cogan’s syndrome is a rare disease characterized by recurrent inflammation of the cornea, fever, malaise, acute episodes of vertigo, and hearing loss. In the case of a 7-year-old boy, hearing loss was irreversible despite corticosteroid therapy, and after 12 weeks, cochlear implantation was done. 15 There is also the rare case of a 4-year-old boy with a tumor of the endolymphatic sac whose first clinical manifestation was SHL. 16 A severe form of myeloid leukemia began as unilateral severe AHL and then moderately severe SHL in the other ear. The process is basically induced by hyperviscosity caused by leukostasis syndrome. 17 Intralabyrinthine hemorrhage accompanied by dizziness, SHL and aseptic meningitis, also represents a possible etiological factor to think about.
Audiological and Other Examinations
A survey of children with SHL involves ENT and audiological testing and application of audiological procedures to determine the etiology of hearing loss. The test protocol includes the following steps: medical history, otorhinolaryngology examination with otomicroscopy, determination of hearing threshold methods, subjective or objective audiometry, and vestibular testing. In addition to ENT examination, examination by an ophthalmologist and pediatrician is required. Specific laboratory analysis to be done include serological testing for rubella, parotitis, CMV, HSV, syphilis, toxoplasma gondii, hormone analysis testing of thyroid function, and urine analysis. A number of patients are referred to genetic counseling where decisions are made based on cytogenetic and molecular genetic testing. Neuroradiological examination includes computerized tomography, when necessary, and magnetic resonance imaging.
Prognostic Factors in SHL
Adverse prognostic factors were younger age and severity of SHL. Hearing initially greater than 50 dB has a worse prognosis. The association of vertigo and SHL as well as a steep curve of the audiogram were predictors of adverse prognosis. The association of tinnitus with SHL is irrelevant to the outcome. Full recovery occurs in about 57% of patients and partial recovery in 36%. 18
Treatment of SHL in Children
Treatment of sensorineural HL can be conservative, and surgical treatment can be considered if conservative treatment fails. In cases of AHL with unknown etiology, it may be reasonable to suppose that it is an autoimmune disease, for which many authors still suggest use of systemic corticosteroids. Also, it makes sense to try treatment with corticosteroids in patients with large vestibular aqueduct syndrome. Prevention of HL in the course of bacterial meningitis is an integral part of the protocol of the therapy, which involves antibiotics and corticosteroids. Prevention can also be done by vaccination against the most common causes of meningitis, such as Haemophilus influenzae type b and Streptococcus pneumonia. 19 Implementation of systemic corticosteroids in SHL is not indicated if the disease is caused by the mumps virus, ototoxic drugs, and infection with CMV. Diagnostic and therapeutic protocols should take place together, starting at the same time, because it is very important not to be late with treatment. Most of the authors advise the use of corticosteroids, with an initial dose of 1 mg/kg TM, with a gradual decrease over 10 to 15 days. Higher doses of corticosteroids as bolus are justified only in individual cases (proved or seriously suspected autoimmune SHL). Because of the frequent occurrence of spontaneous recovery, it is argued that routine use of corticosteroids is not justified. 20 In cases of treatment failure in bilateral SHL, hearing amplification is indicated. In the case of bilateral profound HL, cochlear implantation is the optimal choice. It is a surgical procedure of installing an electronic device that bridges the dysfunctional inner ear and transmits electrical impulses to the auditory nerve.
Table 2 shows the etiological factors and outcome in patients with SHL treated at the Institute for Mother and Child Health Care in Serbia “Dr Vukan Cupic” from 2000 to 2013.
Patients Treated for Acute Hearing Loss at the Institute for Mother and Child Health Care in Serbia “Dr Vukan Cupic” During 2000-2011.
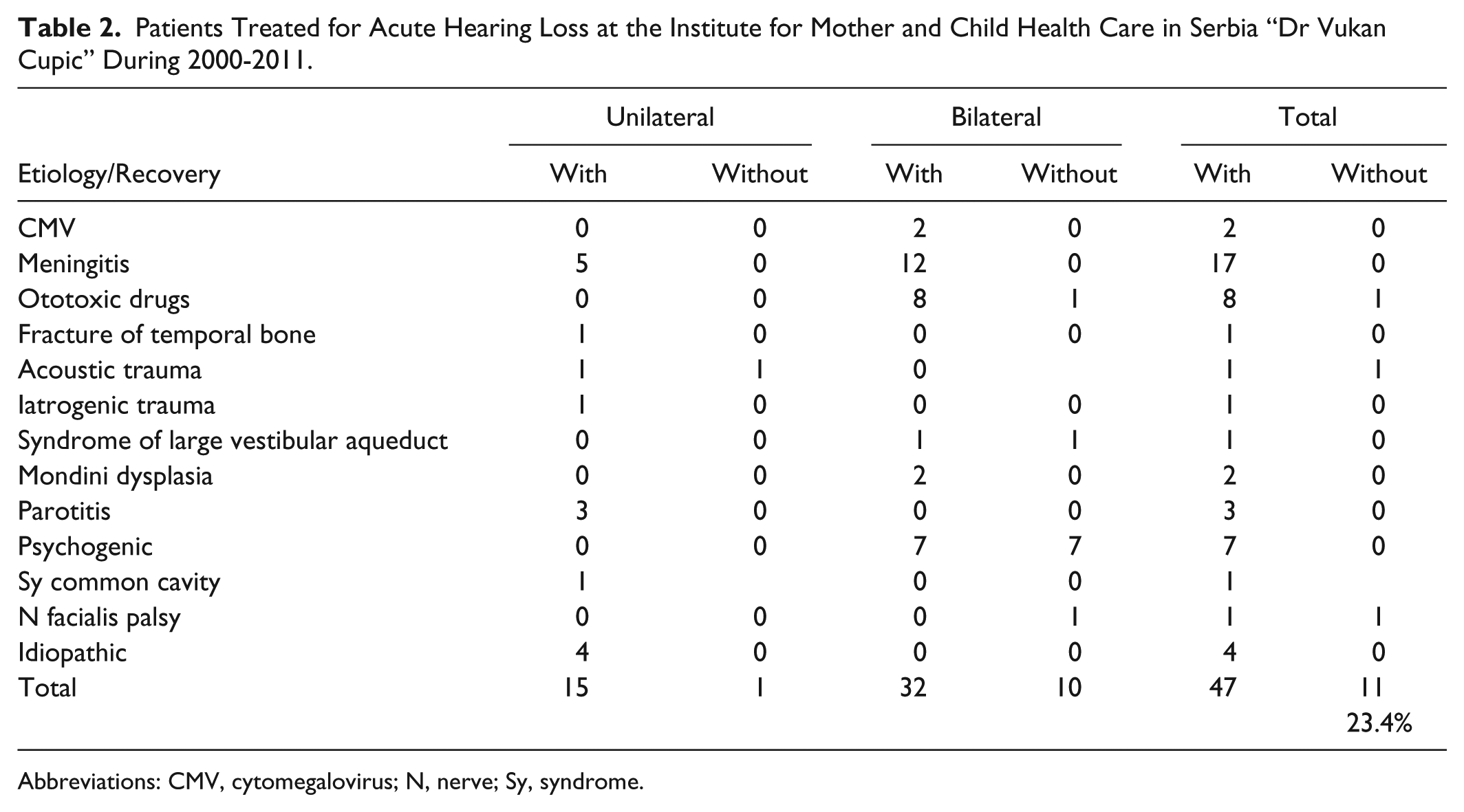
Abbreviations: CMV, cytomegalovirus; N, nerve; Sy, syndrome.
Conclusion
Sudden sensorineural hearing loss in children is a rare disease with different etiologies. Diagnosis involves a complex and interdisciplinary process, and therapy with medications does not always yield good results. Every child with suspected SHL should be directed to undergo audiological examination.
Key Points
Sudden sensorineural hearing loss in children is a rare disease with different etiologies. Causes of AHL can be numerous—congenital and acquired.
Diagnosis involves complex and interdisciplinary processes.
Therapy with medications does not always yield good results. Adverse prognostic factors are younger age and severity of SHL, hearing initially greater than 50 dB, the association of vertigo and SHL, and steep curve of the audiogram. Full recovery occurs in about 57% of patients and partial recovery in 36%
Questions
Problem in the inner ear (yes) Problem in structures surrounding the inner ear (yes) Problem in entire body (yes) Problem in immunological system (may be) Problem in hepatobiliary system (no)
It is not always possible to determine the time of occurrence of lesions (and make a connection with infection). If viruses or bacteria in the epipharyngeal mycosis exist, it does not mean that they are the cause (it may be just colonization). Serological tests do not confirm that infections damage the inner ear (may be they had some other target). Audiological tests indicate the existence of a functional deficit but not the location, extent, and duration of infection (no connection). Diagnosis of diseases of the membranous labyrinth cannot be confirmed by standard radiography (it is true but not for this question).
Younger age Severity of sensorineural hearing loss (correlation) Hearing initially greater than 50 dB (correct) The association of tinnitus with sensorineural hearing loss (it does not matter) Body temperature (irrelevant)
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.