
Abstract
The outcomes of patients admitted to the hospital following a sport-related concussion are largely unknown. Medical records of patients admitted to the pediatric trauma service between 2008 and 2011 after sustaining a sport-related concussion were reviewed. In all, 59 participants were in the high-velocity activities group, and 21 in the field or court sport group. Abnormal CT scans were found in 14 patients in the high-velocity group and 2 in the field or court sport group. The majority of participants in the field or court sport group were football players, all of whom had normal CT scans. Headache was predictive of an abnormal CT scan. Among the patients, 56% clinically improved and were discharged the following day. Patients with field or court sport–related concussion admitted to a pediatric trauma service appear to be at low risk for clinically significant intracranial pathology and do well in the acute setting.
Introduction
Traumatic brain injury (TBI), defined as an alteration in brain function or other evidence of brain pathology caused by external forces, is a leading cause of morbidity and mortality in the pediatric population.1-3 Mild TBI (mTBI) or concussion is defined as a trauma-related, short-lived, and generally completely reversible impairment of neurological function that resolves spontaneously, usually without neuroimaging abnormalities. 4 However, there is a 10% risk for intracranial abnormalities in patients identified as having a mTBI, and a 1% risk of hemorrhage requiring immediate neurosurgical interventions.5,6 The acute management of mTBI requires recognition of these abnormalities in a timely manner because a delay may increase morbidity and mortality.
Athletics is a large part of childhood. Approximately 60% of high school students participate in at least 1 organized sport, and many younger children are active in multiple sports. 7 Participation in recreational sports is also common in the pediatric population, further increasing the number of children involved in sports. From 2001 to 2005, an estimated 502 000 emergency department (ED) visits for concussion occurred in children from the ages of 8 to 19 years. 8 Research regarding sport-related concussion has increased significantly since 1999, and several organizations have published position statements regarding the identification, management, and prevention of sport-related TBI.4,9-11
Between 15% and 70% of children who present to an ED with a head injury will undergo neuroimaging with a CT scan, though >90% will not have a significant abnormality.12-14 The lifetime risk of cancer attributable to radiation from CT scans has received increasing attention, and recent reports have cautioned against the liberal use of CT scans, particularly in children.15,16 Recently published guidelines suggest mandatory CT scans for pediatric patients with mTBI and Glasgow Coma Scale (GCS) score <15. 17 However, the low yield of CT scans in this situation has raised questions regarding both the utility and cost-effectiveness of this practice. 17
A review of the literature did not reveal any articles on the outcomes of patients with sport-related concussion admitted to the hospital. The purpose of this study was to evaluate clinical presentation, neuroimaging findings, and short-term outcomes of patients with sport-related mTBI admitted to a pediatric trauma service.
Methods
Participants
All children with a discharge diagnosis of mTBI or concussion who were admitted to the pediatric trauma service at a level 1 trauma center between January 1, 2008, and April 30, 2011, were identified from the pediatric trauma registry using ICD-9 codes. The study included patients who presented directly to the ED as well as patients who were transferred after evaluation at an outside hospital. Patients included were those admitted with recreation or sport-related brain injury, 6 to 18 years old, and with a GCS score of ≥13 at the time of presentation to the pediatric trauma center. If a patient met inclusion criteria with multiple injury events during the review period, data were obtained only from the most recent admission. A retrospective chart review was performed, and data were collected from the trauma database and patient medical records. Data included age, gender, school grade (when available), date of injury, mechanism of injury, GCS score, presenting symptoms, neuroimaging findings (if obtained), treatment while in the hospital, symptoms on discharge from the hospital, return to play recommendations/activity restrictions, and outcomes following hospital discharge. Mechanism of injury was categorized as having occurred during a high-velocity activity or during a field or court sport event. High-velocity activities included skiing, snowboarding, horseback riding, motorcross, skateboarding, ATV/motorcycle, and biking, whereas field and sport court activities encompassed football, basketball, wrestling, gymnastics, and others (golf, rugby, and dodgeball). Neuroimaging was documented as normal or abnormal. Abnormal was defined as a finding that was a direct result of the presenting trauma. A total of 80 pediatric patients were identified and included in the study.
The Penn State Hershey Medical Center institutional review board approved the protocol before data collection.
Statistical Analysis
Descriptive statistics were prepared for patients, including GCS scores, the number of head CTs, and the number of CTs that were read as abnormal. Summaries included frequencies and percentages for categorical variables and means and standard deviations for continuous variables. Presenting symptoms such as loss of consciousness, headache, and vomiting were analyzed to determine whether they were predictive of an abnormal CT scan, using logistic regression. P values <.05 were considered statistically significant. Analyses were conducted using SAS version 9.2 (SAS Institute Inc, Cary, NC, USA).
Results
Of the 228 pediatric patients admitted to the pediatric trauma service with mTBI, 80 (35%) had a recreation or sport-related mTBI. Figure 1A shows the number of patients included per sport within the high-velocity activities group, and Figure 1B shows the number of patients included per sport within the field and court sports group. High-velocity activities accounted for 59 (74%) of those patients, whereas 21 (26%) had injuries from a field or court sport (Figure 1B). Table 1 shows the demographic and clinical characteristics of the high-velocity activities group and the field or court sport group.
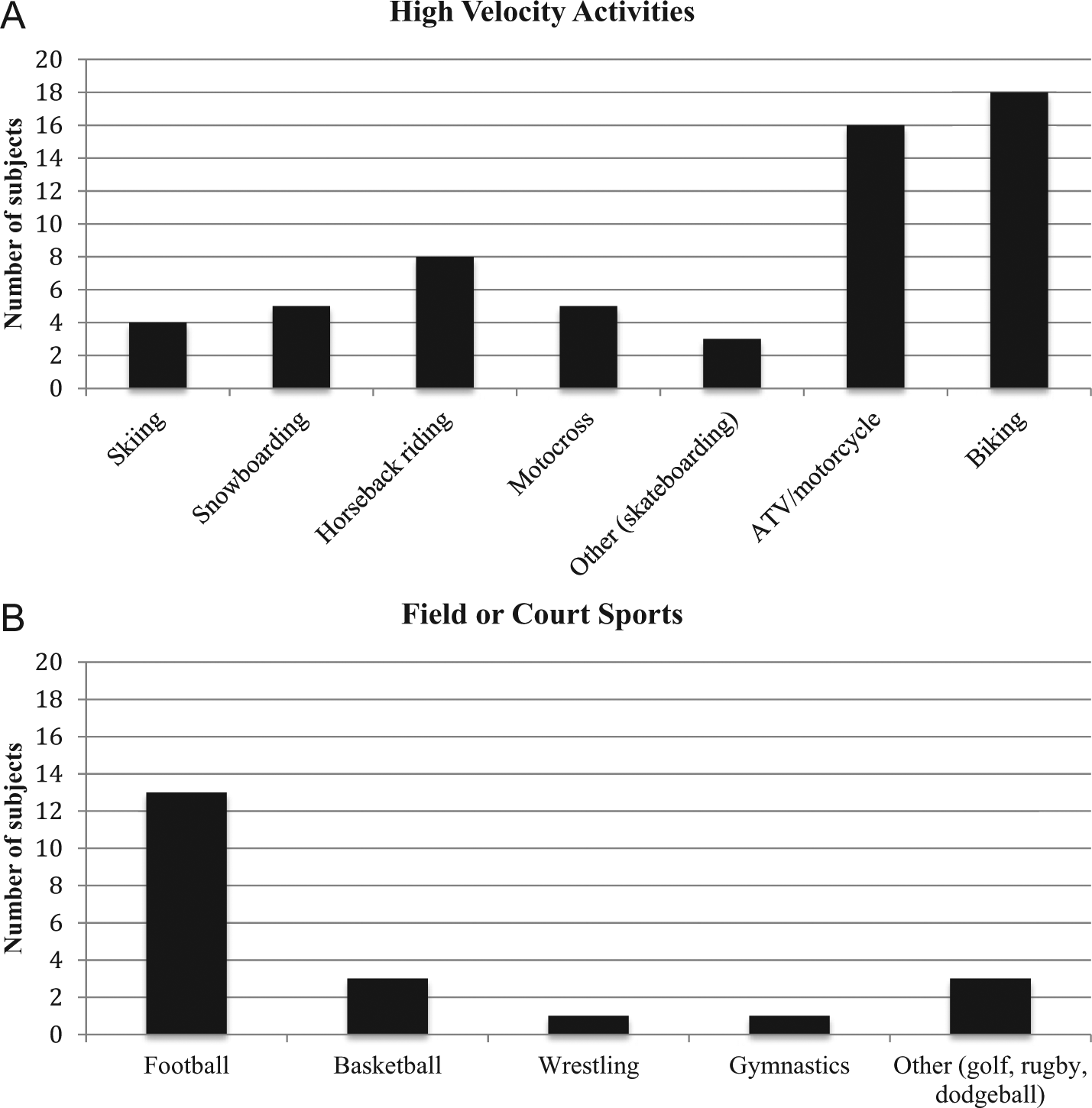
A. Distribution of activities within the high-velocity activities group. B. Distribution of activities within the field or court sports group.
Demographic and Clinical Characteristics of the Field or Court Sports and High-Velocity Activities Groups.
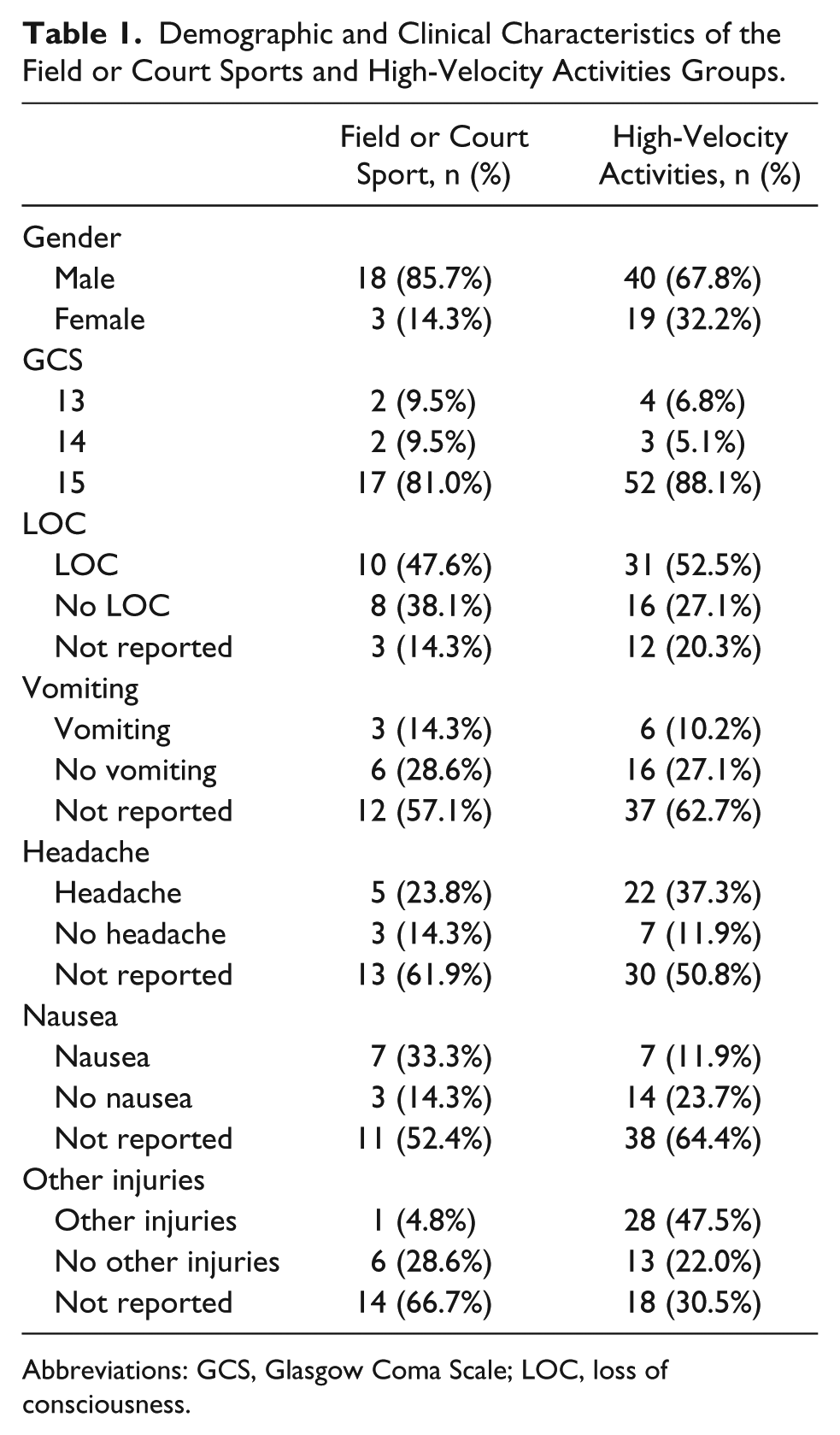
Abbreviations: GCS, Glasgow Coma Scale; LOC, loss of consciousness.
A GCS score of 15 was reported for 69 out of the 80 patients, including all but one of the patients with an abnormality on CT scan. A cranial CT scan was obtained on the day of injury for 72 of the 80 patients, 56 (78%) of which were read as normal. High-velocity activities resulted in 14 (27%) abnormal CT scans in 51 of those who received scans, whereas field or court sport activities resulted in only 2 (10%) abnormal scans out of 21 who received scans. Figure 2 shows the percentages of normal and abnormal CT scans in both the high-velocity activities and field or court sports groups. Although there was a higher percentage of abnormal CT scans in the high-velocity activities group as compared with the field or court sports group, the difference was not statistically significant (P = .13). In the high-velocity activities group, 2 of the 14 patients with abnormal CT scans underwent surgical treatment, one for an orbital fracture repair and the other for evacuation of an epidural hematoma. Neither of the 2 patients in the field or court sports group with abnormal CT scans underwent surgery.
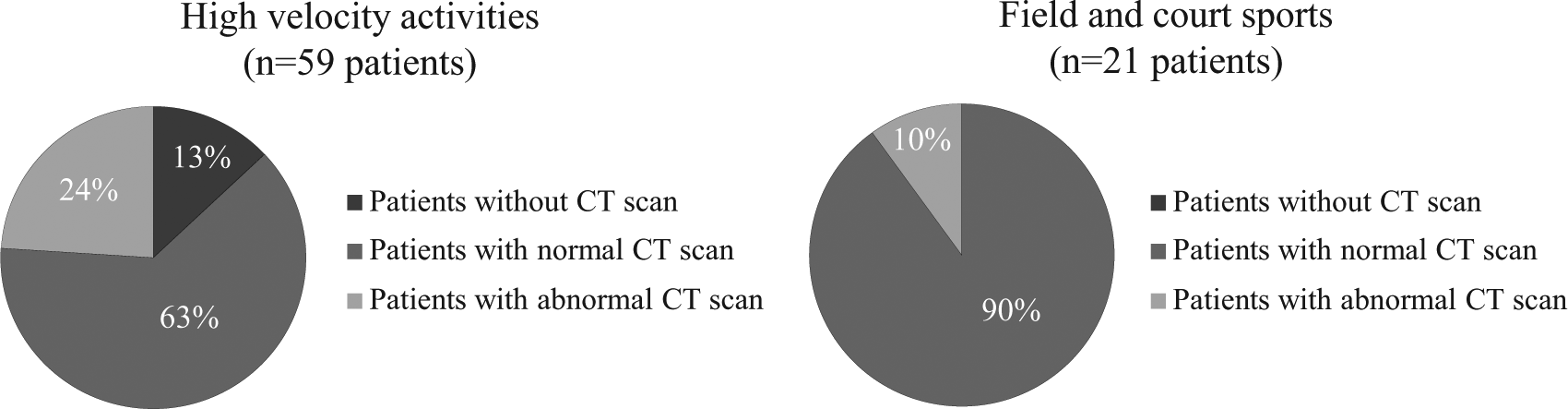
Distribution of CT scan results within the high-velocity activities and field or court sport groups.
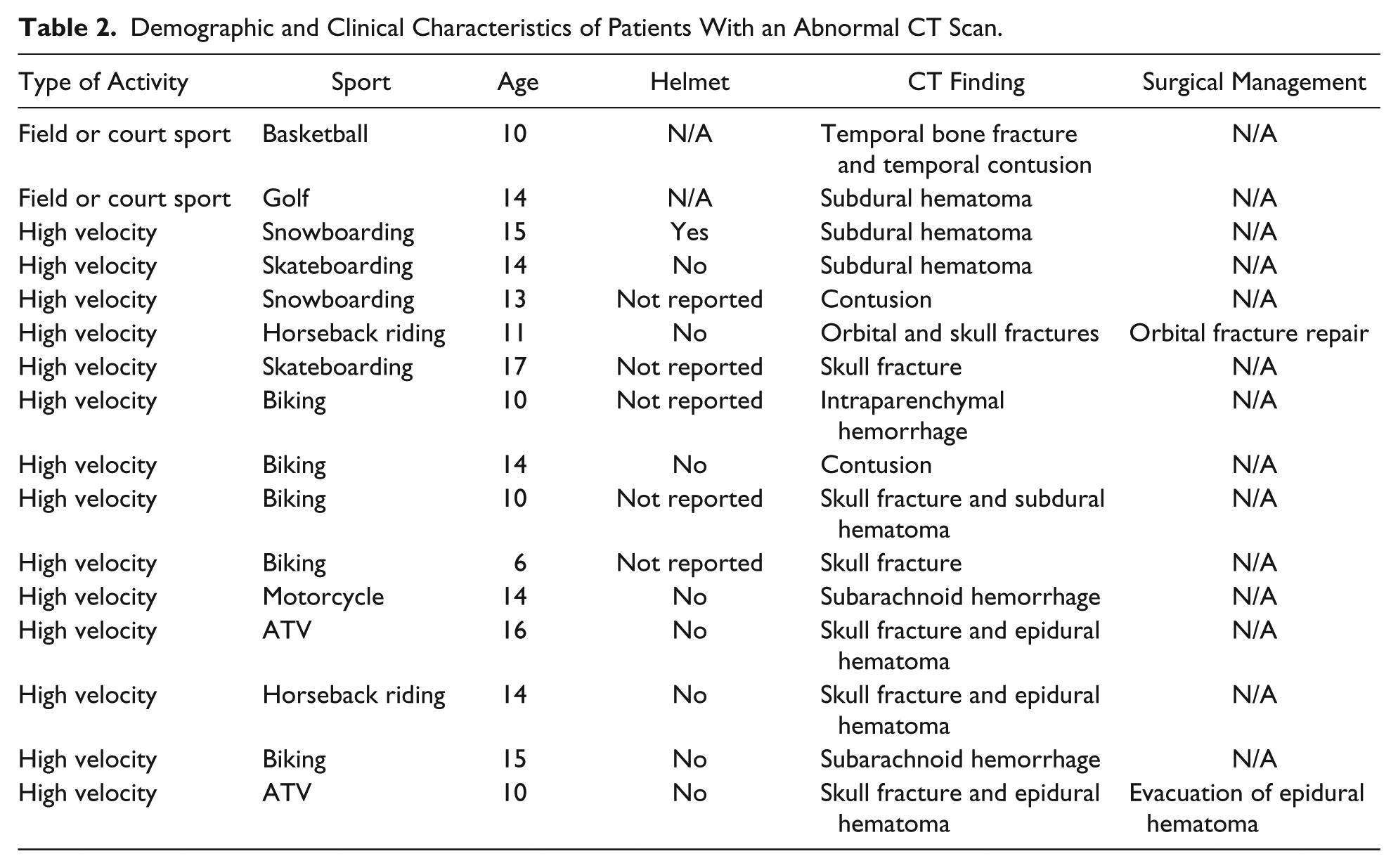
Table 2 shows the activities, CT scan results, and surgical management (if applicable) for the patients with abnormal CT scans. Of the patients in the high-velocity activities group, 29 (49%) clinically improved and were discharged after 1 day in the hospital, whereas 16 (76%) patients in the field or court sports group were discharged after 1 day. Whereas headache was predictive of an abnormal CT scan (P = .01), neither loss of consciousness (P = .16) nor vomiting (P = 1.0) were indicative of the presence of an abnormality on CT scan. The presence of other injuries was not indicative of an abnormal CT scan (P = .77).
Demographic and Clinical Characteristics of Patients With an Abnormal CT Scan.
Discussion
This study is the first to evaluate sport and recreation-related concussion in patients admitted to a pediatric trauma service. For the field and court sports group, our results are consistent with previous studies demonstrating the low risk of clinically significant intracranial abnormalities in the acute phase of mTBI.5,6 However, the patients in the high-velocity activities group had a higher frequency of intracranial abnormalities, with high-velocity activities accounting for 14 of the 16 abnormal CT scans. Both patients who required surgical intervention were from the high-velocity activities group.
CT imaging is a valuable tool that has been used with increasing frequency over the past 10 years for identification of intracranial abnormalities.16,18 However, there has recently been increasing concern regarding the risk of radiation-induced cancer, particularly in children, because of their increased period of risk and potentially greater sensitivity to radiation as compared with adults.15,19-23 A recent study found that cumulative doses of 50 to 60 mGy from CT scans in childhood may triple the risk of leukemia and brain cancer. 16 It was also noted, however, that because these cancers are rare, the absolute risks are small. It was estimated that 1 excess case of leukemia and 1 excess case of a brain tumor would occur per 10 000 head CT scans. 16 When evaluating any patient with a sport-related head injury, the potential of missing a significant intracranial injury must be weighed against the potential long-term risks of radiation exposure, and parents should also be a part of this decision. A recent report indicated that the majority of parents who were informed of the cancer risks regarding CT scans were still willing to consent for a head CT scan following head injury in their child. 24
The majority of sport-related TBI in children are concussions, from which most patients will recover, though there is mounting concern about the long-term effects of concussions, and especially repeated concussions. 4 One of the major features from the most recent consensus statement on concussion in sport indicates that concussion may result in neuropathological changes, but the acute clinical symptoms largely reflect a functional disturbance rather than a structural injury. 4 Thus, conventional neuroimaging is usually normal following a concussive injury; however, intracranial hemorrhage can occur in rare instances.7,10 A major challenge is the need to identify the rare life-threatening complications among a large cohort of patients with concussion. 17 Haydel and Shembekar 25 found a clinical decision rule could be used to determine if a CT scan should be obtained in children aged 5 years and older with mTBI and a normal level of consciousness. The presence of any of the following—headache, vomiting, intoxication, seizure, short-term memory deficits, or physical evidence of trauma above the clavicles—was significantly associated with an abnormal CT scan result. 25 However, the majority of the injuries in this study were not sport related. The current study found that whereas headache was predictive of an abnormal head CT scan, loss of consciousness and vomiting were not. It is unlikely that clinical decision rules with 100% sensitivity and acceptable specificity can be developed, and clinicians should use a combination of clinical decision rules and clinical judgment in the acute evaluation of mTBI. 26
Although there are clear guidelines for returning to sport following concussion, there are no guidelines following an intracranial hemorrhage or other structural abnormality. Although there is no evidence in the literature to determine when it is safe to return to sport following an intracranial hemorrhage, some experts feel that a complete resolution of the hematoma should occur prior to return to play. 27 A careful individualized approach involving the player, sports physician, and neurosurgeon for return to sport has been recommended.27,28
Although the comparison did not reach statistical significance, this study demonstrated a lower rate of abnormality on cranial CT scans in patients participating in field or court sports as compared with patients involved in high-velocity activities. It has been noted in the most recent Zurich concussion statement that the majority of athletes with sport-related concussion do not need neuroimaging. 4 These guidelines suggest that if the level of consciousness is a concern, the athlete should be imaged and observed in the hospital setting. 4
Helmets are one of the most widely used devices for prevention of TBI. Although there has been some concern that athletes are more likely to take bigger risks when wearing a helmet, research has shown that helmets reduce brain injury morbidity and mortality.29-31 This research has predominantly been done in sports such as biking, skiing, and snowboarding, whereas data from sports such as football are limited as a result of required use. 30 The idea of the protective effect of helmets, which help reduce the risk of intracranial injury, is borne out in this study. Of the athletes with abnormal CT scans whose injuries were sustained during sport activities where helmets are recommended, only 1 of 14 was reported to be wearing a helmet.
The highest number of patients among the field or court sports group was from football. High school football players have a higher likelihood of sustaining concussion as compared with other sports persons.32,33 In addition, medical personnel are often present at football games, making it more likely that medical attention is sought early on when symptoms might be at their highest level. Clinicians may feel that football involves more violent impacts compared with other sports, and a more conservative approach in management is often followed.
The study has several limitations. The sample size is relatively small, and the study was retrospective. Some clinical data points were absent in some of the participants. Moreover, participants were identified from a hospital trauma database, and it is possible that some patients meeting the study inclusion criteria were not entered into the database. The study includes only patients who were admitted to a level 1 trauma center, possibly increasing the number of patients with abnormal CT scans. Any children who were seen and discharged from the ED or were admitted to an outside hospital were excluded. It is possible that the participation rates in various sports and activities in this region may have affected the results. It was also unclear why patients with concussion and a high GCS with a normal CT scan were admitted to the hospital. It could have been that the primary reason for admission was for other injuries and not mTBI.
In conclusion, patients with field or court sport–related mTBI with GCS scores of 13 to 15 admitted to a pediatric trauma center appear to be at low risk for clinically significant intracranial structural abnormalities and do well in the acute setting. High-velocity activities appeared to have a greater risk for intracranial pathology. Future research should continue to assess these risks as well as the results of both short- and long-term outcomes for children with sport and recreation-related concussion.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by the National Institutes of Health (NS060722 and ES019672) and the Pennsylvania Department of Health Tobacco Settlement Funds (C06 RR016499). All analyses, interpretations, and conclusions are those of the authors and not the research sponsors. The authors have no financial relationships relevant to this article to disclose.