
Abstract
Background. Validated clinical scales, such as the Canadian Acute Respiratory Illness and Flu Scale (CARIFS), have not been used to differentiate influenza (FLU) from other respiratory viruses. Methods. Secondary analysis of a prospective cohort presenting to the emergency department (ED) with an influenza-like infection from 2008 to 2010. Subjects were children aged 0 to 19 years who had a venipuncture and respiratory virus polymerase chain reaction. Demographics and CARIFS items were assessed during the ED visit; comparisons were made between FLU and non-FLU subjects. Results. The 203 subjects had median age 30.5 months; 61.6% were male. Comorbid conditions (51.2%) were common. FLU was identified in 26.6%, and were older than non-FLU patients (69.7 vs 47.9 months, P = .02). Demographic, household factors, and mean CARIFS score did not differ between FLU (33.7), and non-FLU (32.0) (mean difference 1.6, 95% CI: −2.0 to 5.2) groups. Conclusions. CARIFS cannot discriminate between FLU and non-FLU infection in ED children with influenza-like infection.
Background
Each year, influenza (FLU) infection reaches epidemic proportions, affecting numerous children across the United States. The majority of illness produced by influenza are mild and nonspecific, resembling that of other common respiratory viruses, such as rhinovirus or parainfluenza virus. However, influenza infection carries significant disease burden in the pediatric population: in addition to infecting between 10% and 40% of US children in the winter seasons, more than 20 000 children are hospitalized, with nearly 100 deaths attributable to influenza each year.1,2 In addition, it is estimated that the annual economic burden of influenza is substantial, with expenditure of approximately $12 billion in the United States.3,4
Typically, symptoms of influenza may include high fever, upper and/or lower respiratory symptoms, as well as general malaise, or so-called “influenza-like illness (ILI).1,2,5 While the clinical presentation of ILI is nonspecific, in peak influenza season the prevalence of influenza A or B infection among patients with ILI is approximately 40%. 5 As a result of high disease prevalence, empiric antiviral therapy is often instituted in children presenting early in the course of disease. Early treatment with neuraminidase inhibitors, such as oseltamivir, has been associated with reductions in symptom duration, risk of complications (such as secondary pneumonia and secondary bacterial infections) and frequency of hospitalizations, emergency department (ED), and clinic visits.6-8 Use of neuraminidase inhibitors is especially important in children with asthma and other high-risk respiratory conditions, as it decreases rates of related complications from influenza infection. Therefore, early identification and treatment has great potential to improve morbidity and mortality in children infected with influenza.
Both clinical and laboratory methods have been used to identify children infected with influenza. Point-of-care viral testing has demonstrated a positive impact children with influenza, through shortening the duration of illness, and avoiding unnecessary additional testing.9,10 However, rapid detection tests for influenza are expensive, of variable accuracy, and not universally available in healthcare sites. To date, attempts to develop a clinical prediction based on symptoms present at the time of initial evaluation have proven unreliable in diagnosis of influenza.11-15 However, none of these prior studies have attempted to use a validated clinical scale to differentiated and detect influenza from other respiratory viruses.
The Canadian Acute Respiratory Illness and Flu Scale (CARIFS) is a validated scale that measures disease severity in children with acute respiratory infections. 3 This brief scale assesses a combination of clinical symptoms and functional impairments that can be rapidly completed during a healthcare visit. CARIFS can be assessed in toddlers and older children, and can be completed by parents during healthcare encounters. 3 Evaluations of CARIFS have been performed in children with undifferentiated upper respiratory illness; no specific examination of the scale in patients with ILI has been previously attempted. Therefore, the objective of this investigation was to determine whether CARIFS scores could distinguish influenza illness from that of other respiratory viruses in children presenting for ILI in a pediatric ED. It is our hypothesis that children with influenza infection will have worse severity scores compared with those infected with noninfluenza viruses.
Methods
Study Subjects and Setting
This was a secondary analysis of a prospective cohort study of children aged 0 to 19 years, presenting to an urban tertiary care children’s hospital ED from Fall 2008 to Spring 2010, during peak influenza seasons. Subjects were eligible for participation if they (1) had a clinical presentation of an ILI, as defined by the Centers for Disease Control and Prevention (fever ≥37.8°C plus cough and/or sore throat, without other known cause) 5 ; (2) if a venipuncture was performed as part of their ED routine care; and (3) if a nasopharyngeal aspirate was obtained in the ED for multiplex polymerase chain reaction (PCR) for respiratory viruses. There were no specific exclusion criteria other than failure to meet the above inclusion criteria. All treatment decisions, including venipuncture and respiratory viral testing, occurred at the discretion of the treatment team. Consent for participation was obtained prior to study procedures. The study was approved by the hospital’s institutional review board.
The Canadian Acute Respiratory Illness and Flu Scale (CARIFS)
Following consent, the subject’s parent or caregivers completed the CARIFS in the ED via a brief questionnaire. CARIFS includes items that assess clinical presentation, including symptomatology and functional measurements. Parental assessments of these items pertain to the previous 24-hour time frame. The scale assesses individual items on a 4-point ordinal scale (no problem = 0, minor problem = 1, moderate problem = 2, major problem = 3). Respondents were provided an option of “don’t know/not applicable”; per usual procedure these scores were imputed by calculating the mean score of all items, and multiplying this mean by the total number of items, yielding the total score. As a result, increasing CARIFS scores correlate with more severe disease. 3 CARIFS is an 18-item scale: for children older than 5 years, the full scale is used, for children younger than 5 years, 3 items (headache, sore throat, and muscle aches) are not used for assessment, per protocol. 3 For the purposes of this study, we used the validated 15-item CARIFS for children younger than 5 years based on the anticipated age distribution of the children eligible for inclusion in the study.
Data Collection
Demographics factors, including age, gender, race and ethnicity, and household exposures were collected. Household exposures included the number of people in household, daycare/school attendance, known ill contacts, presence of smokers in the home, and reported influenza vaccination status; these were prospectively recorded for study subjects during enrollment. Chart review was used to supplement parental questionnaire to determine missing demographic items. All data was entered into a standard data collection form, to ensure consistency.
Nasopharyngeal aspirates were tested for respiratory viruses using a real-time, multiplex PCR assay developed by our hospital’s clinical virology laboratory. 16 Specific viruses identified included influenza A and B, parainfluenza virus type 1-4, rhinovirus, human metapneumovirus, adenovirus, and respiratory syncytial virus. Multiplex viral respiratory PCR samples were collected during the ED visit, and results of testing were collected from the medical record after the ED visit was complete. For the purposes of analysis, subjects were subclassified as having FLU if influenza A or B was identified either alone or in combination with other viruses; all other subjects were considered to have noninfluenza infection (non-FLU).
Statistical Analysis
Data were summarized using standard descriptive statistics: categorical data were described using proportions and percentages, and continuous data were summarized using means and standard deviations. CARIFS scores were calculated per protocol, as stipulated by Jacobs et al, 3 and reported as means with standard deviations. Comparative analyses of CARIFS were conducted based on presence of FLU, or non-FLU infection. Item-level and total score analysis was performed, including comparisons between groups with and without influenza infection. CARIFS score items were analyzed using 2 methods: as a continuous variable and as a dichotomous variable. Total CARIFS scores were dichotomized combining item scores of 0 and 1 (no or minor problem), and item scores of 2 and 3 (moderate and major problem) into separate groups. Statistical comparisons were made using independent sample t tests for continuous variables; categorical variables were compared using chi-square test. Significance was set at the P < .05 level. Results were reported with 95% confidence intervals (CIs), where indicated. All statistical analyses were performed using the Statistical Package for the Social Sciences, version 20 (IBM SPSS, Chicago, IL).
Results
Subject Characteristics
During the study period, 203 children were eligible and enrolled in the study. The overall study population had a median age of 31.8 months (range 0.3-227.8; Inter quartile range 24.1-88.3), and 61.6% were male. The majority of subjects identified themselves as African American (50.2%), followed by white (42.4%), and other race (6.9%). The majority of subjects reported having a comorbid conditions (55.2%), predominantly asthma, which was present in 47 (23.2%). Daycare or school attendance (53.7%) was common among subjects, as were household contacts: on average 4.55 (95% CI 4.34-4.77) persons resided in each household. Exposure to ill contacts was frequent among the study population, reported by 43.4% of subjects. Overall, smokers were present in 27.6% of households and 52.7% of subjects reported receiving their annual influenza vaccination.
Viral Epidemiology
Of the 203 study subjects, 117 (57.6%) had a single virus identified, 24 (11.8%) had multiple viruses, while 62 (30.5%) did not have any respiratory viruses identified. Of the 117 subjects with a single identified respiratory virus, influenza was most frequent in 42 (35.8%), followed by rhinovirus in 30 (23.9%), human metapneumovirus in 16 (13.7%), respirarory syncytial virus in 13 (11.1%), adenovirus in 12 (10.3%), and parainfluenza in 5 patients (4.3%). The FLU population was composed of 54 (26.6%; 95% CI 20.5-32.7) total subjects in whom influenza A or B virus was identified; 12 (5.9%; 95% CI 2.7-9.1) of these subjects had influenza in addition to a coinfecting virus. When comparing the FLU study population with non-FLU patients, subjects with documented FLU infection tended to be older in age, and were more likely to have exposure to an ill contact (Table 1). Other demographic and household exposures did not significantly differ between the 2 groups.
Demographic and Household Exposures in Subjects With and Without Influenza (FLU).
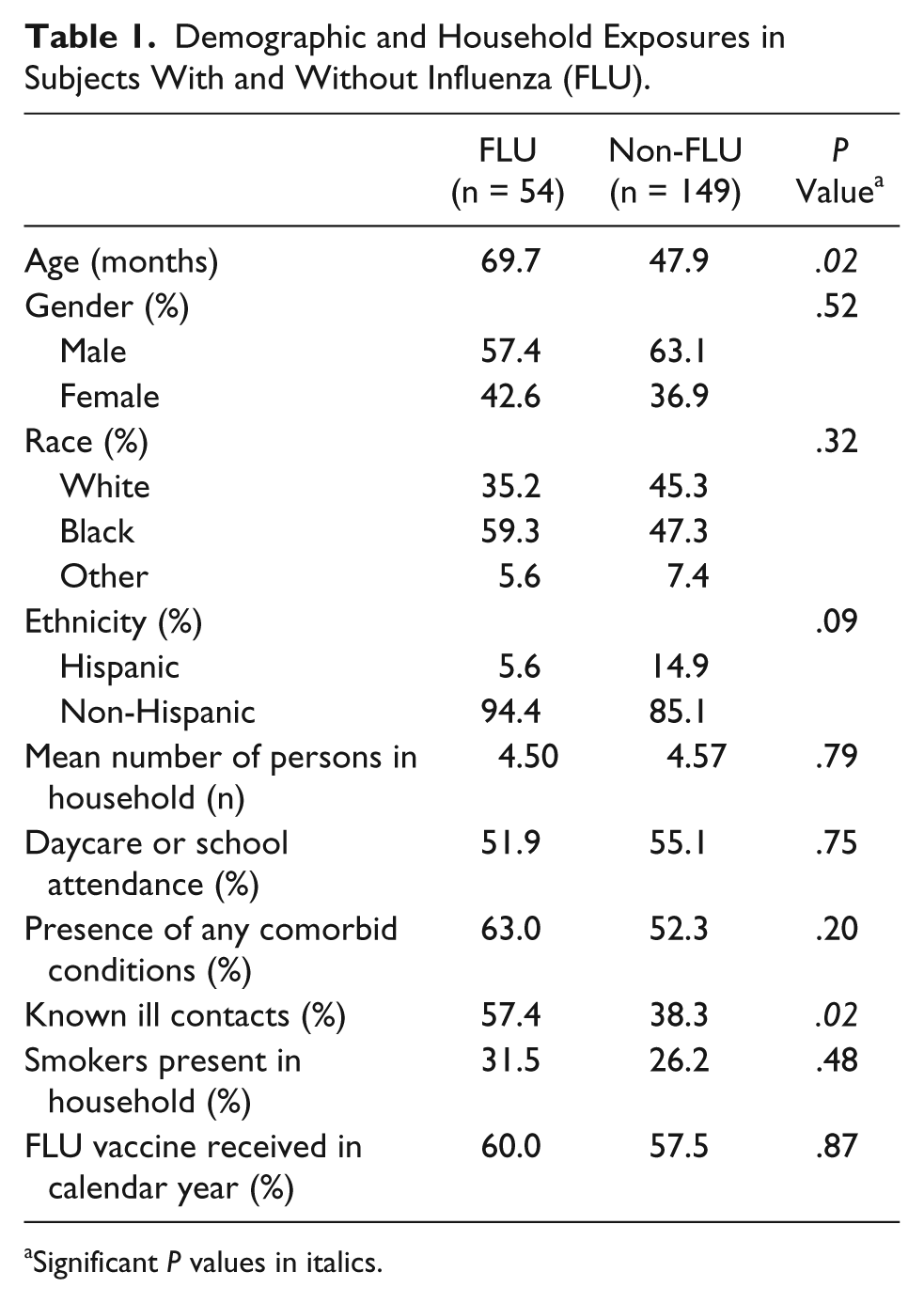
Significant P values in italics.
Performance of CARIFS
The overall mean CARIFS score for the cohort was 32.5 ± 11.6. Comparison of mean CARIFS score between the FLU group (33.7 ± 10.7) and the non-FLU group (32.0 ± 11.9) was not significantly different (mean difference 1.6, 95% CI: −2.0 to 5.2). Mean CARIFS score did not differ for subject with influenza virus alone (33.4 ± 10.0), compared those with a single other virus identified (32.5 ± 12.5), to those with multiple viruses (32.1 ± 11.4), or no virus identified (31.9 ± 11.4) (F = 0.15; P = .93).
Examination of individual CARIFS items for the overall study cohort is presented in Table 2. Fever, cough, feeling unwell, tired were identified as most problematic among the study cohort, while vomiting was least commonly reported. When individual CARIFS items were compared between FLU and non-FLU groups, reports of fever and being tired were significantly higher in patients with FLU (Table 3).
Categorical and Mean Item-Level Scores for Symptoms in the Overall Study Cohort Assessed Using CARIFS.
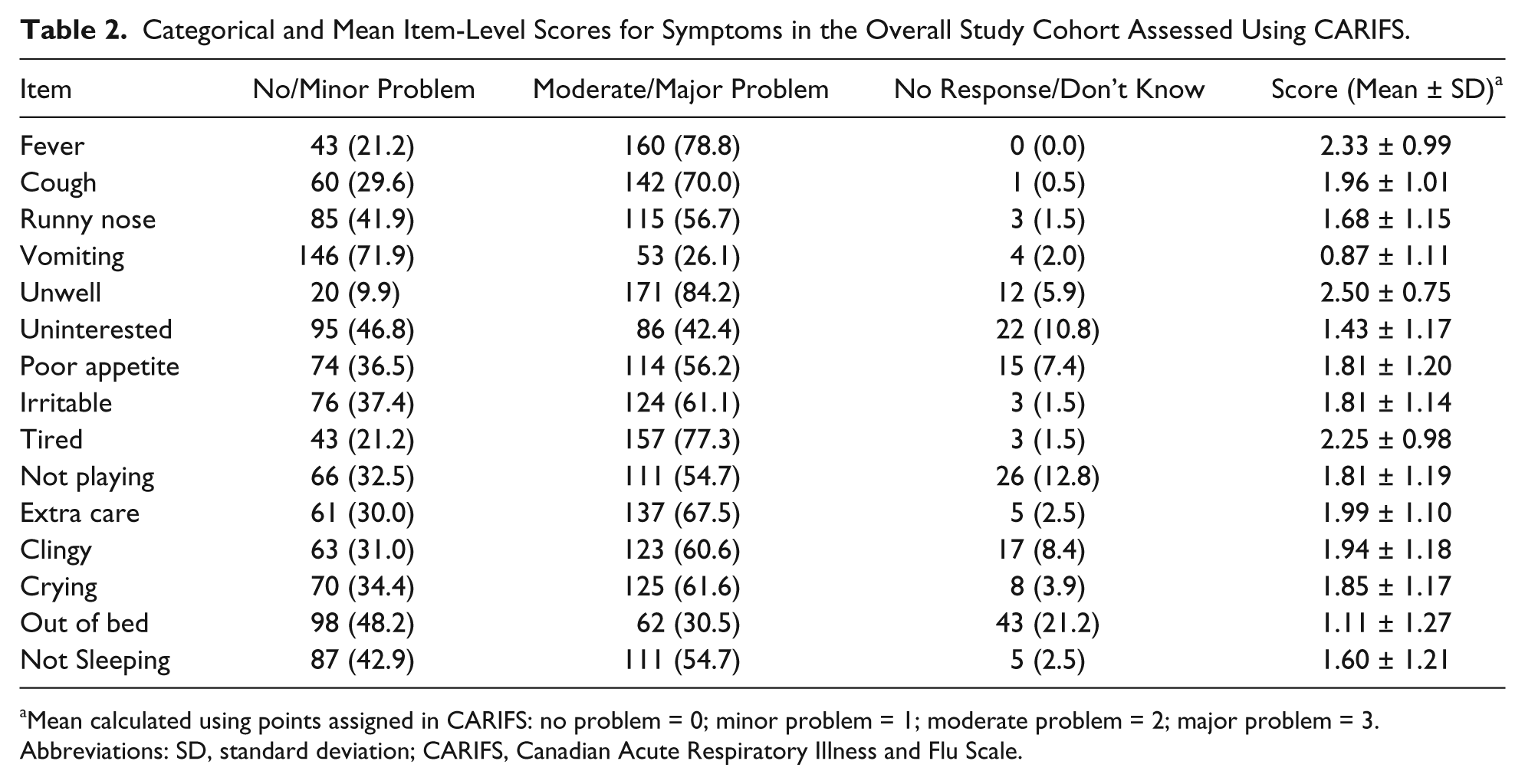
Mean calculated using points assigned in CARIFS: no problem = 0; minor problem = 1; moderate problem = 2; major problem = 3.
Abbreviations: SD, standard deviation; CARIFS, Canadian Acute Respiratory Illness and Flu Scale.
Item-Level Comparisons for CARIFS in Subjects With and Without Influenza (FLU).
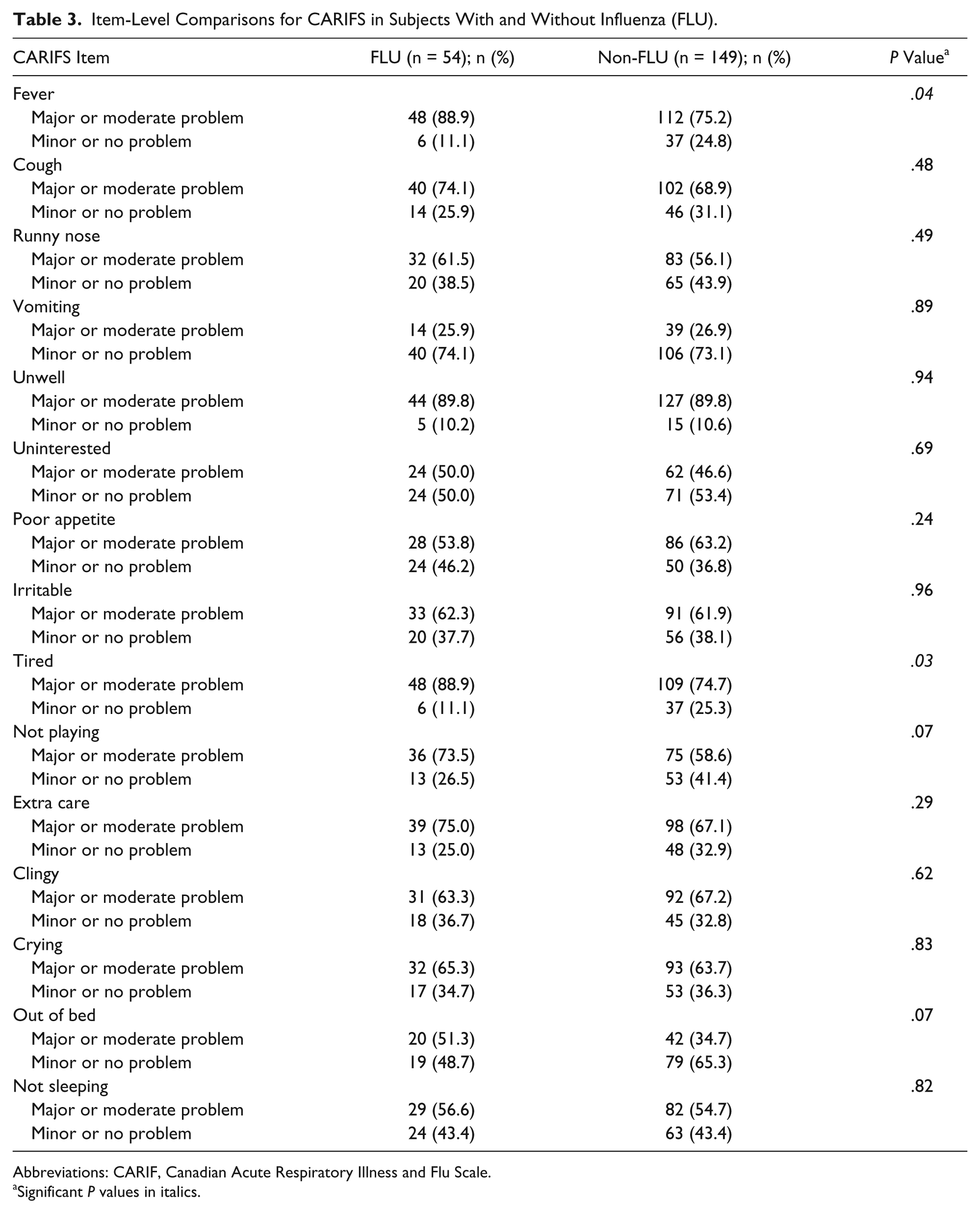
Abbreviations: CARIF, Canadian Acute Respiratory Illness and Flu Scale.
Significant P values in italics.
Discussion
This study is the first to examine the performance of a validated scale, CARIFS, to identify patients with influenza infection based on clinical features at the time of presentation to an ED for care for ILI. Our results suggest that, despite its development specifically for acute respiratory viral illnesses, CARIFS is unable to discriminate between infection from influenza and those with other respiratory viruses. Although methods for diagnosis of influenza early in the course of illnesses are required for initiation of appropriate therapy, it appears that clinical presentation is of limited utility for early identification. Thus, the further implementation of alternative methods of influenza diagnosis, such point-of-care testing, appear to be of greater value in determining candidates for institution of antiviral therapy.
In the pediatric population, influenza infection produces substantial disease burden, leading to increased health care utilization and morbidity among the general population, and even mortality in high-risk children.1,17 Since antiviral treatment must be prescribed early in the disease course to be beneficial,6,8 early detection of influenza is crucial in guiding treatment decisions, and potentially affecting outcomes. Traditionally, the diagnosis of influenza is secured using laboratory methods, including PCR or isolation in culture. For early diagnostic utility, however, these methods are limited, as processing and results are not available during the patient encounter. Several rapid influenza tests have been developed, which could potentially be implemented at the point-of-care, and consequently identify candidates for antiviral treatment.9,10 At present, point-of-care influenza tests possess variable accuracy, and are not routinely available in EDs, with cost being one of the limitations.11,13,18 Therefore, clinical symptoms have traditionally been used to predict whether or not children have influenza. However, to date, no constellation of symptoms in influenza infection has been identified, with acceptable diagnostic accuracy, to permit widespread utility for institution of early antiviral therapy.11,12,14
The findings of our study, which evaluated a validated scale of respiratory viral illness, CARIFS, did not prove to have sufficient discriminative ability for influenza among children with ILI. While statistical differences did exist in a few item level analyses, the overall CARIFS score was similar across patients with all respiratory viruses. Report of fever and overall tiredness was higher in patients with influenza; however, such nonspecific symptoms are likely to be of little clinical value in the ED. Several other reports of functional status were greater with influenza, though not significantly. Therefore application of CARIFS and its components mirror the findings of several other clinical evaluations of influenza, in that differentiation of this virus from other respiratory viral infections is exceedingly difficult.11,12
Previous studies of clinical detection of influenza from other respiratory viruses have produced variable results, but differed from our study in several ways. We evaluated the performance of the CARIFS scale in an acutely ill population, as children required a venipuncture and viral testing. While many prior studies focused on a more general population with ILI, it was hypothesized that evaluation of CARIFS in a more “severe” population would be more likely to demonstrate a clinical difference, and evaluate those more likely to benefit from easily antiviral therapy. Nonetheless, our findings were in concert with other studies, which determined that clinical evaluation alone is insufficient for detection of influenza. In addition, our study was restricted to the pediatric population presenting with ILI, while many prior evaluations were performed on adult patients, or patients of all ages.11,12,19 In these studies, acute onset of fever, cough, diaphoresis, myalgia, and headache were the among findings with the highest likelihood for influenza infection.11,13,14,19 Consistent with our study, fever appears to be a common presenting complaint in children with influenza. On the other hand, cephalgia and myalgias, which may be commonly reported in adults, are difficult to assess in children, particularly those that are preverbal, which comprise a large number of children seeking health care for ILI. Overall, even when evaluated in systematic reviews, clinical signs alone, or in combination, did not possess adequate ability to detect influenza infection.13,14
The utility of clinical symptoms has been specifically evaluated in children.12,18 Similar to our study, Friedman and Attia 18 examined clinical parameters in children with febrile respiratory illnesses presenting to pediatric ED. Using many common presenting symptoms, the authors concluded that the triad of cough, headache, and pharyngitis, in combination, had 80% sensitivity and 78% specificity for detecting influenza in children presenting with ILI. While these results are among the better test characteristics described, it should be noted that the false-positive rate exceeds 20%, which would subject a large number of children to unnecessary antiviral exposure. Unfortunately, since no statistical difference was found using CARIFS, we were not able to determine “threshold” values for calculation of test characteristics for influenza infection, though, in comparison to their findings, we similarly found a higher association of fever with influenza. As a result of a largely school-age study population in the study by Friedman and Attia 18 , the authors were able to incorporate headache in the study. In addition, half of the study population did not have a virus identified; as use of viral isolation in culture—a low yield gold standard—introduces large possibility of misclassification. Nonetheless, our results add to the body of literature suggesting that the predictive ability of clinical diagnosis for yields false-negative and false-positive results, and great potential for over- and undertreatment.
Our study is not without limitation. The possibility of spectrum bias exists, as we enrolled patients that had both a venipuncture and viral testing in the ED. While this may bias toward a more acute population, it also allowed us to evaluate patients with a higher likelihood of positive viral testing, and a population that is most likely to benefit from early antiviral therapy. 20 In addition, we chose to use the validated CARIFS scale for children younger than 5 years, to account for the demographic of the overall study population; subjects younger than 5 years comprised the majority (70.4%) of our study population, Importantly, CARIFS recommends this methodology, which maintains the validity of the scale 3 ; however, it is possible that our findings may not be applicable to children older than 5 years with ILI. Finally, the study was conducted in the ED of single high acuity, tertiary care center; therefore our findings may not be generalizable beyond that population.
Conclusion
Despite its properties as a validated measure for acute respiratory illnesses, CARIFS does not have the ability to discriminate influenza infection from that of other respiratory viruses in pediatric patients. These findings add to the current literature demonstrating the inability of clinical symptoms and presentation to accurately identify children with influenza, thus limiting use for institution of targeted antiviral therapy. Our findings support the currently used approach of evaluation of influenza-like illness in the context of local disease prevalence, when making therapeutic decisions regarding suspected influenza. Continued development of point-of-care testing, combined with clinical assessment, has the potential for accurate identification influenza in children in the ambulatory setting.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported in part by a Commonwealth Universal Research Enhancement Program (CURE) grant (RFP-05-07-11) from the Pennsylvania Department of Health.