
Abstract
Objective. Pulse oximetry screening (POS) is becoming the standard of care in screening for critical congenital heart disease (CCHD). Our objective was to characterize the historical diagnostic pattern in a rural tertiary care children’s hospital and explore how universal POS might affect morbidity, mortality, and care delivery. Patients and Methods. We identified patients <6 months of age in the Vermont Children’s Hospital echocardiogram database with CCHD diagnosed between 2002 and 2011. Charts were reviewed to characterize timing of diagnosis, course, and outcome. The medical examiner was consulted to identify deaths due to undetected CCHD during the study period. Results. Of 60 329 live births, 73 (0.12 %) were diagnosed with CCHD. Of these, 31 (42%) were diagnosed prenatally, 34 (47%) were diagnosed by clinical examination in the nursery, 7 (9.6%) were diagnosed after nursery discharge, and 1 (1.4%) was born at home. The 8 patients not diagnosed by prenatal ultrasound or in the nursery were considered cases of undetected CCHD. Three had normal oxygen saturation (>95%) at diagnosis. Three presented with cardiovascular compromise. None died and all were well at the most recent follow-up. Review of autopsy reports from patients <6 months found no deaths from undetected CCHD during the study period. Conclusions. Over a 10-year period at our institution, universal POS could have identified 5 patients with undetected CCHD, possibly avoiding the need for resuscitation in 3. Examination of local diagnostic data may affect the cost/benefit considerations of universal POS initiatives in a setting of limited healthcare resources.
Introduction
Congenital heart disease is the most common birth defect, occurring in nearly 1 of every 100 live births per year in the United States and accounts for nearly 30% of infant death due to congenital anomalies.1,2 Critical congenital heart disease (CCHD) is a subset of congenital heart disease that typically requires surgery or catheter-based intervention during early infancy. CCHD occurs in approximately 1.5 of every 1000 live births. 3 Prior to the advent of pulse oximetry screening (POS), CCHD was detected by prenatal ultrasound or clinical examination in the newborn period. Rates of prenatal detection vary greatly, ranging from 3.3% to 60%, and are influenced by access to care as well as level of operator training.4-6 Some infants with CCHD may not exhibit signs or symptoms while in the newborn nursery, leading to discharge prior to diagnosis in 13% to 48% of cases. 7 Failure to diagnose CCHD prior to discharge may place some infants at increased risk of morbidity and mortality. 8
Universal POS was reported as a screening method for CCHD more than 10 years ago. 9 The goal of universal POS is to close the “diagnostic gap” described by Riede et al 5 by identifying infants with CCHD not detected by prenatal ultrasound or clinical examination. Universal POS was shown in several large European studies to be effective in screening for CCHD in the newborn period.4-6 A recent meta-analysis of 229 421 infants showed that universal POS had a sensitivity of 76.5%, a specificity of 99.9%, and a false positive rate of 0.14%. 10 In the face of mounting evidence for the efficacy of universal POS, as well as advocacy efforts from parental groups, CCHD was added to the US Recommended Screening Panel for newborns in 2011. The American Academy of Pediatrics, in conjunction with the American Heart Association, also endorsed universal POS for CCHD screening for all newborns. 11
In response to mandates from national organizations, many states have adopted legislation requiring universal POS. According to the Centers for Disease Control and Prevention, only 8 states (including Vermont) have not taken any official action on implementation of universal POS. 12 Concerns about implementation, reporting, and cost have been identified as barriers to adoption of universal POS. 13 The economic burden of false positives may be especially significant in rural areas with limited pediatric cardiology services, given the need for neonatal transport to obtain echocardiography.
As states mandate universal POS for CCHD, understanding the range of potential benefits and costs may help inform policy decisions. Initial population-based studies on implementation of universal POS in the United States have focused on population-dense areas with widespread access to tertiary pediatric care, including pediatric cardiology services. 14 Little is known about implementation in rural areas. The objective of our study was to characterize the historical diagnostic pattern in a rural children’s hospital and to explore how universal POS might affect morbidity, mortality, and health care costs.
Methods
Study Design and Setting
Approval from the University of Vermont Institutional Review Board was obtained prior to the start of the study. We conducted a retrospective case series study of all patients diagnosed with CCHD at Vermont Children’s Hospital (VCH) over a 10-year period (January 1, 2002 until December 31, 2011). The case series was limited to patients with CCHD lesions identified by the American Academy of Pediatrics as primary targets for universal POS screening. These lesions are: hypoplastic left heart syndrome (HLHS), pulmonary atresia, tetralogy of Fallot (TOF), total anomalous pulmonary venous return (TAPVR), transposition of the great arteries (TGA), tricuspid atresia and truncus arteriosus.
The referral region covered by neonatal transport services at VCH includes 8 counties and 6 community hospitals in Vermont as well as 3 counties and 3 community hospitals in northern New York. The average distance between VCH and the community hospitals in the VCH referral region is 58.5 miles (range 28-105 miles). During the study period, data from the Vermont and New York Departments of Health reported 60 329 live births in the 11 counties that comprise the referral region.
Based on 2012 US census data, Vermont is 95.4% white, with 11.3% living below the poverty level, compared with national norms of 77.9% and 14.9%, respectively. The population density of Vermont is 67.9 persons per square mile, which ranks 32nd in the United States. 15 The patient population in northern New York served by VCH is similar in racial composition, with higher levels of poverty and even lower population density. 16 Limited transportation options, geographic obstacles, and severe winter weather represent significant barriers to care throughout the VCH referral region. Access to tertiary-level pediatric care is also limited, as VCH provides the only pediatric cardiology services in the region. Pediatric cardiac surgery services are not available at VCH.
Study Subjects
Infants were included if they were younger than 6 months, had echocardiography performed at VCH, and were diagnosed with 1 of the 7 primary CCHD lesions. Patients diagnosed prenatally at VCH were also included. Most infants were born at VCH or other community hospitals throughout the referral area. Infants diagnosed prenatally were referred for delivery at one of the regional surgical centers.
Main Outcome Measures
The main outcome measures were cardiovascular compromise or death. Cardiovascular compromise was defined by a history of fluid resuscitation (>20 cm3/kg of isotonic fluids), inotropic agents, or intubation at presentation. 17 The secondary outcome measures were timing of diagnosis (prenatal, during newborn nursery admission, and after discharge from newborn nursery), and incidence of CCHD over the 10-year study period.
Data Sources and Analysis
The VCH pediatric echocardiogram database was used to identify patients. The database includes both prenatal and postnatal echocardiogram data. Medical records were then reviewed to determine the timing of diagnosis and outcome. The state medical examiner and pediatric pathologist at VCH were contacted and infant mortality cases during the study period were reviewed to assess for patients who might have died prior to echocardiogram diagnosis of CCHD. We used standard descriptive statistics in the analysis of the data.
Results
Of the 60 329 live births that occurred within the VCH referral region during the study period, 73 (0.12%) were diagnosed with CCHD. TOF was the most common CCHD lesion, diagnosed in 23 patients, followed by TGA diagnosed in 18 patients (Figure 1). Of the patients with CCHD, 31 (42%) were diagnosed by prenatal ultrasound, 34 (47%) were diagnosed by clinical examination prior to nursery discharge, 7 (9.6%) were diagnosed after nursery discharge, and 1 (1.4%) was born at home.
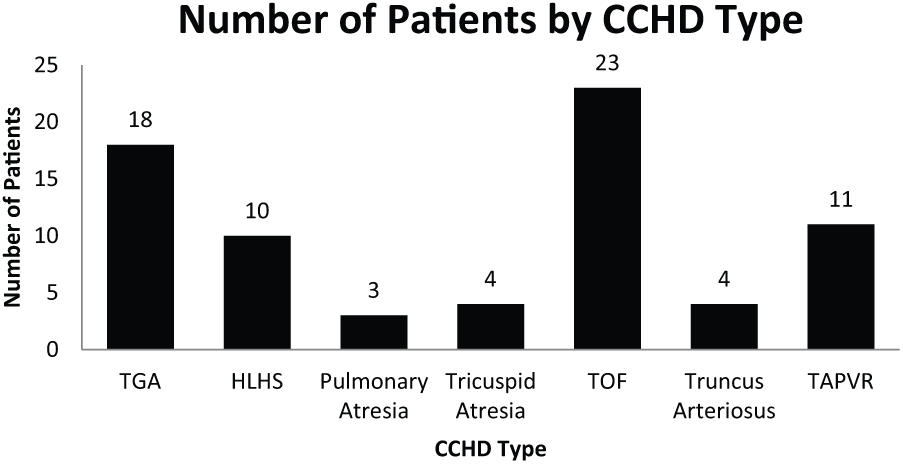
Critical congenital heart disease (CCHD) lesion type.
The 8 patients with CCHD not diagnosed by prenatal ultrasound or clinical exam in the newborn nursery were considered cases of undetected CCHD. The diagnoses included TOF in 4 patients, TAPVR in 2 patients, HLHS in 1 patient and TGA in 1 patient. Of the 4 patients with TOF, 3 had normal oxygen saturation (>95%) documented at the time of diagnosis. The mean age at diagnosis for the patients with TOF was 53 days (range 7-182 days) and the mean age at surgery was 146 days (range 114-190 days). Three patients with undetected CCHD (1 with HLHS, 1 with TAPVR, and 1 with TGA) presented with evidence of cardiovascular compromise as defined by IV fluid resuscitation, intubation, or administration of inotropic agents. The mean pH at presentation of the patients presenting with cardiovascular compromise was 7.28 (range 7.08-7.53). None of the patients with undetected CCHD died. All underwent corrective surgery and were well at the most recent follow-up (Table 1).
Patients With Undetected CCHD.
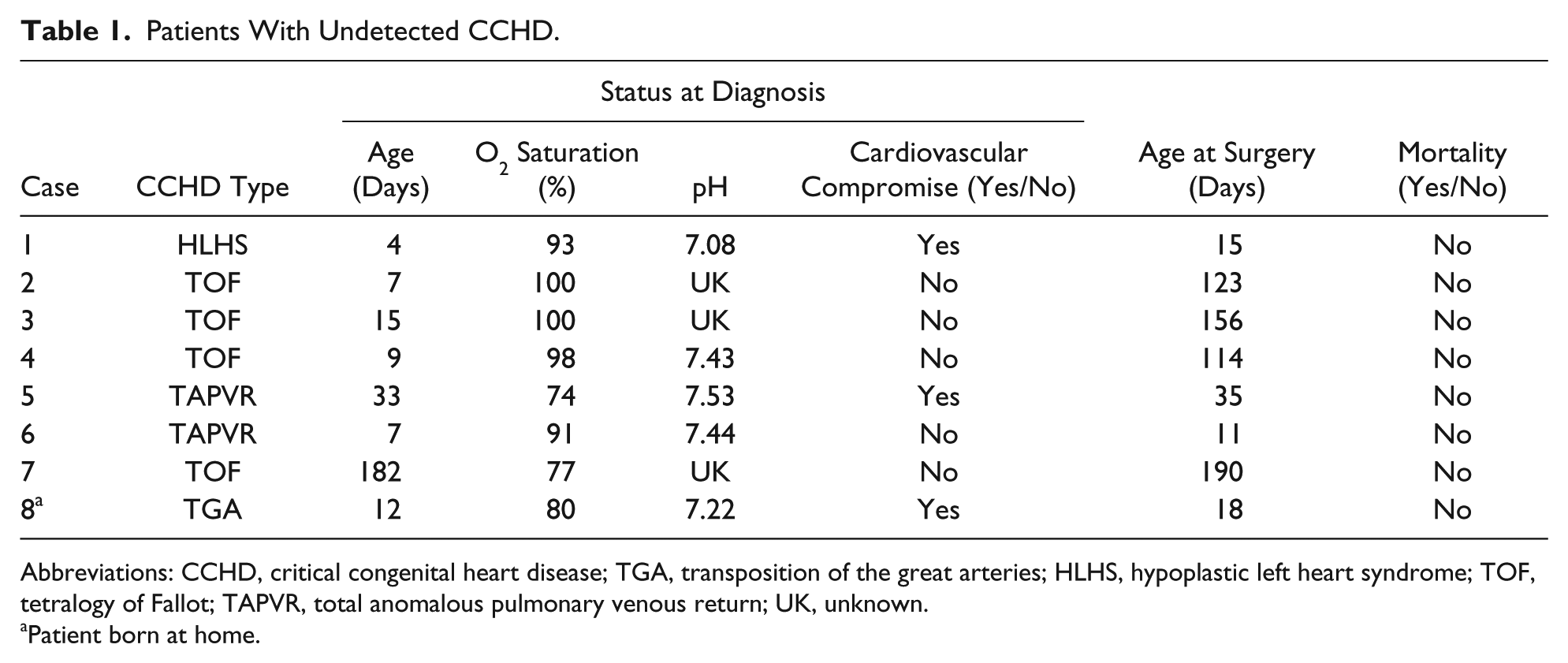
Abbreviations: CCHD, critical congenital heart disease; TGA, transposition of the great arteries; HLHS, hypoplastic left heart syndrome; TOF, tetralogy of Fallot; TAPVR, total anomalous pulmonary venous return; UK, unknown.
Patient born at home.
The rate of prenatal diagnosis increased from 27% (10/37) prior to 2007, to 58% (21/36) subsequently. No patient with CCHD was discharged undiagnosed after 2006 (Figure 2). Review of the records of the state medical examiner and pediatric pathologist at VCH revealed no deaths in infants younger than 6 months due to undetected CCHD during the study period.
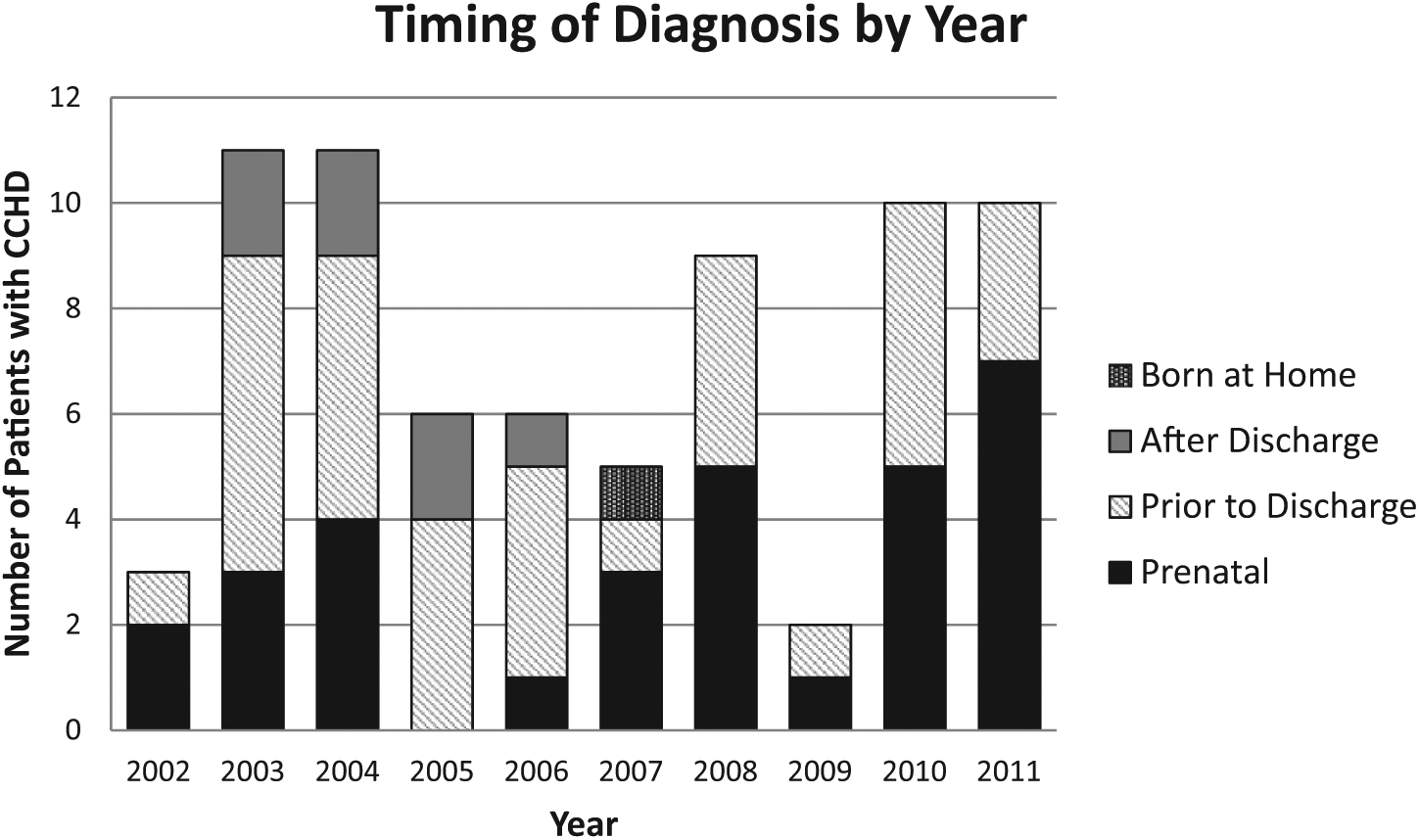
Timing of diagnosis by year.
Discussion
Based on a retrospective, 10-year review at a rural, tertiary care children’s hospital, universal POS may have identified 5 patients with undetected CCHD, possibly avoiding the need for resuscitation in 3. The rate of undetected CCHD documented in our study was 13.3 per 100 000 live births. Other studies have documented rates of undetected CCHD ranging from 4 to 15 per 100 000 live births. 18 Half of the patients in our study with undetected CCHD had TOF. Since at least 3 of these patients had normal oxygen saturation at diagnosis, it is unlikely that they would have been detected by universal POS.
Only 1 infant with undetected CCHD was born at VCH. The remaining study patients with undetected CCHD were born at community hospitals in the VCH referral region, or, in 1 case, at home. Our findings are consistent with previous studies that have shown that CCHD is more likely to remain undetected at hospitals with level I or II nurseries. 19
Most universal POS proposals have been hospital-based, but unmonitored children born at home are likely at higher risk of having undetected CCHD. During the study period, there was an average of 146 home births per year in Vermont. Our patient with TGA born at home highlights the importance of accommodating home births in systems being developed for universal POS. The Vermont Department of Health has systems in place for other home-based newborn screening, including audiology and newborn blood spot testing, and will need to establish a mechanism for timely CCHD screening as well. 20
Vermont Children’s Hospital accounts for approximately 30% of the yearly births in the referral area, and is the only facility with access to in-house pediatric echocardiography. In comparison, a recent study in Wisconsin showed that almost 75% of the yearly births occurred in a facility with access to in-house pediatric echocardiography. 21 The majority of births that occur in the VCH referral region occur in small community hospitals with a low birth rate. Obtaining the same low false positive rate with universal POS documented in larger trials is unlikely in a system in which the test is performed infrequently. The high percentage of yearly births that occur in facilities without in-house pediatric echocardiography combined with the risk of a higher false positive rate in small community hospitals has major implications for the cost of universal POS for Vermont and other rural states.
All patients identified with positive POS at community hospitals in the VCH referral region require transport to VCH and admission to the neonatal intensive care unit. For an average neonatal transport and one day admission to the neonatal intensive care unit at VCH the minimum charge is $12 000, not including echocardiography or any additional testing. While the cost of these services likely varies by institution, it is significantly higher than the figures used in previous estimates of cost-effectiveness of universal POS.22,23 Additionally, the psychosocial impact on parents whose infants are transported to another center for further testing after a positive CCHD screen has not been thoroughly investigated, but is likely significant.
Our study has several limitations. The retrospective nature of the investigation means that some clinical details were unavailable. Also, the VCH referral region is not a completely closed system, and some patients with CCHD may have migrated to other centers. In addition, the relatively small number of births in our referral region and relatively high rate of prenatal diagnosis mean that generalization of our findings to other geographic or demographic areas may not be possible. Nonetheless, over a period of 10 years, we did not identify any mortality or serious long-term morbidity that would have been prevented by a universal POS program. Given finite resources, uncertain costs, and possibly limited benefits, the carefully considered implementation and critical reassessment of this or any universal screening program seems prudent.
Footnotes
Acknowledgements
We would like to thank the Pediatric Research in Inpatient Settings (PRIS) Network and participants in the PRIS Pediatric Hospital Medicine manuscript-writing workshop for critical input and guidance.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.