
Abstract
Objective. To identify patient and hospital characteristics associated with the choice of treatment for pediatric patients who present in the acute setting with peritonsillar abscess/cellulitis (PTA/PTC). Study Design. A retrospective cohort study was performed using Healthcare Cost and Utilization Project emergency department, ambulatory, and inpatient state databases for the years 2010 and 2011. Children aged 0 to 17 years were identified using International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) diagnosis code for PTA/PTC. The main outcome of interest was treatment received, which included medical therapy alone, incision and drainage (IND) or tonsillectomy. Multiple logistic regression analyses were conducted to model non-clinical factors associated with treatment received after adjusting for age, hospital state, race, primary expected payer, existing chronic condition(s), and type of hospital. Results. We identified 2994 patients who presented with PTA/PTC. The most common treatment choice was medical therapy alone (30.8%), followed by IND (30.5%) and tonsillectomy (9.4%). There were significant associations between treatment choice and race, primary payer status, and type of hospital (P < .05). We found that Hispanic patients, those with Medicaid as their primary expected payer, and those treated at a designated children’s hospital were 3 nonclinical factors independently associated with an increase in likelihood of receiving tonsillectomy as treatment. Conclusion. There are important nonclinical factors associated with treatment of children who present in the acute setting with PTA/PTC. Additional research is recommended to understand these observed differences in care and how they may affect health outcomes.
Peritonsillar abscess/cellulitis (PTA/PTC) is one of the most common deep neck infections in children and adolescences.1,2 There is an estimation of 13 500 cases in the United States annually. 1 The classical presentation for PTA/PTC includes severe sore throat, fever, and a “hot potato” or muffled voice. Although a sudden onset of severe respiratory distress is rare, delayed intervention of PTA/PTC can allow for disease progression to compromised airways and life-threatening situations. 3
There are several treatment choices available for the pediatric patient diagnosed with PTA/PTC. Considerable evidence supports incision and drainage (IND) and/or antibiotics as appropriate treatment1-5; however, other authors advocate for immediate tonsillectomy.4,5 Although each treatment choice has its own supporting body of research, to our knowledge, demographic and socioeconomic factors associated with treatment choices have not been well described. In our study, we sought to identify nonclinical factors associated with treatment choice for PTA/PTC.
Methods
Data Source
This study used 3 sets of data distributed by the Healthcare Cost and Utilization Project (HCUP), sponsored by the Agency for Healthcare Research and Quality (AHRQ) from 2010 to 2011 from California, Florida, and New York: (1) State Inpatient Database (SID), 6 (2) State Ambulatory Surgery Database (SASD), 7 and (3) State Emergency Department Database (SEDD), 8 The SID captures all hospital discharges, the SEDD captures all emergency department discharges, and the SASD captures all outpatient discharges involving surgeries performed on the same day in which patients are admitted and released in a given state. All data sets represent a population-based sample and capture patient characteristics, diagnoses, and procedures performed, discharge disposition, and a linkage variable to track patients’ health care utilization across encounters. Hospital-level data were obtained through the linkage with the 2011 American Hospital Association survey database. 9
Study Population and Design
Hospital discharges for pediatric patients aged 0 to 17 years were identified using International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) diagnosis code for peritonsillar abscess and peritonsillar cellulitis (475). Each discharge file contains an encrypted variable created by HCUP to represent a unique patient, allowing us to identify multiple records in the SID, SASD, and SEDD that belong to the same person. Additional variables within each discharge file, such as admission source and discharge disposition, also allow us to identify special scenarios such as transfer records or duplicate records. Specifically in the SID, there will be 2 different records if a patient is transferred from one hospital to another. However, since the coding of admission source and discharge disposition is not always consistent, we counted each unique patient only once based on treatment received.
Study Outcomes
Our primary outcome of interest was treatment received for PTA/PTC. Treatment choices were categorized as follows: medical therapy alone, IND, and tonsillectomy. Medical therapy alone is defined as general administration of IV fluids, antibiotics and/or steroids without any surgical procedures. Under this definition, medical therapy is often a part of standard care for patients who present with an acute infection. We differentiate patients who receive medical therapy alone from patients who receive surgical therapy in addition to medical therapy using ICD-9-CM and Current Procedural Terminology (CPT) 10 codes specific to those procedures (Table 1). Hence, patients who received IND were likely to have also received medical therapy. However, since we also sought to identify any differences in care between surgical choices, we differentiated those patients who received IND from those who received tonsillectomy. During our data analysis, we found a number of patients who received a diagnosis for peritonsillar abscess/cellulitis but had no recorded procedure for their discharge. They were labeled as “no code”
Codes Identifying Patient Population.
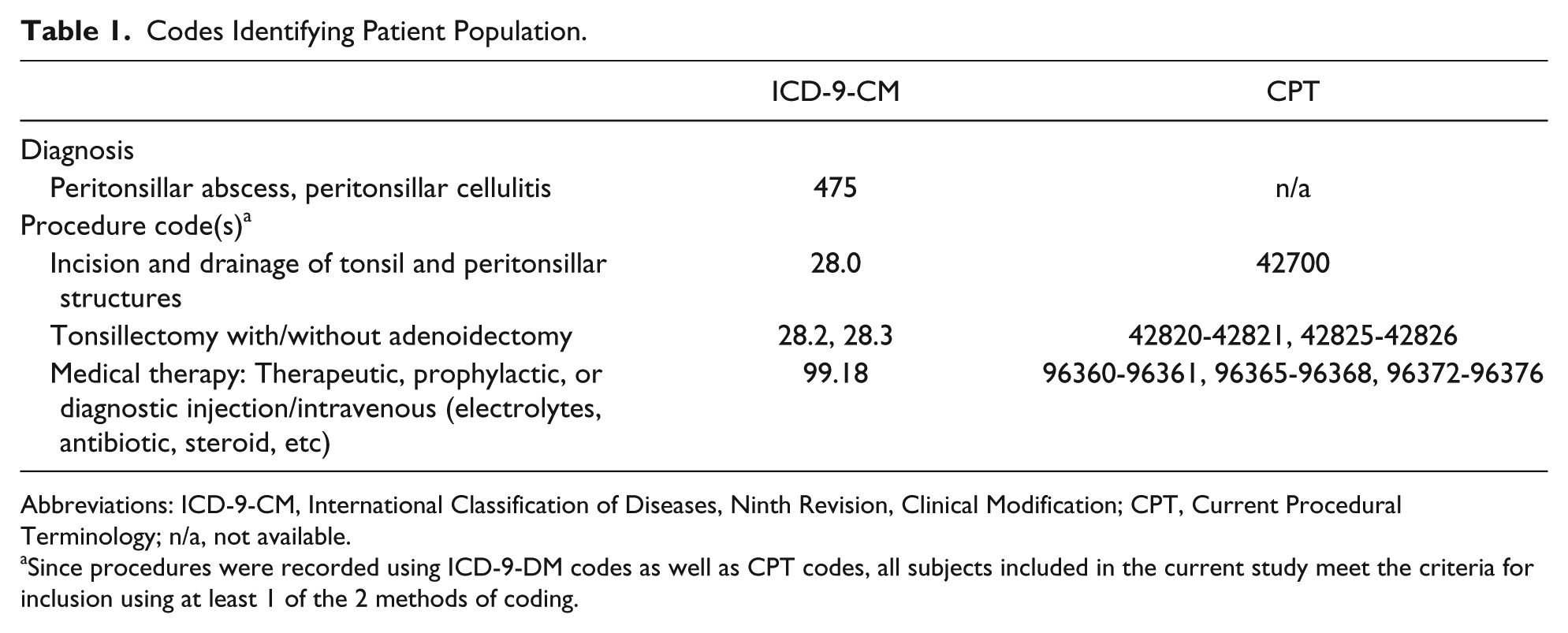
Abbreviations: ICD-9-CM, International Classification of Diseases, Ninth Revision, Clinical Modification; CPT, Current Procedural Terminology; n/a, not available.
Since procedures were recorded using ICD-9-DM codes as well as CPT codes, all subjects included in the current study meet the criteria for inclusion using at least 1 of the 2 methods of coding.
Demographic variables included the following: age, gender, race, primary expected payer, existing chronic condition(s), 11 discharge status, and length of stay if the patient was hospitalized. Race was categorized as follows: white, Hispanic, Black, and other, which include subjects with missing race; primary expected payer was categorized as follows: private insurance, Medicaid and self-pay. In our current study, less than 20 patients were identified with Medicare as their primary expected payer and were thus excluded from analysis based on data use agreement.
Statistical Analysis
Initial analyses were performed with χ2 test to assess differences in categorical demographic variables. After identifying clinically relevant variables and significant differences from univariate analysis, multiple logistic regression models were developed to identify independent predictors of treatment. The following variables were included in the model: age, hospital state, race, primary expected payer, existing chronic condition(s), and type of hospital. Adjusted odds ratios are reported with 95% confidence intervals. Results were considered statistically significant for P values <.05. Statistical analyses were done with Stata, version 12.1. 12
This study was deemed exempt by an official institutional review board.
Results
A total of 2994 patients were identified with PTA/PTC during our study period. Overall demographic data and stratification by treatment are presented in Tables 2 and 3, respectively. All reported differences in age, race, payer, chronic condition, and type of hospital were statistically significant with P < .001.
Study Population.
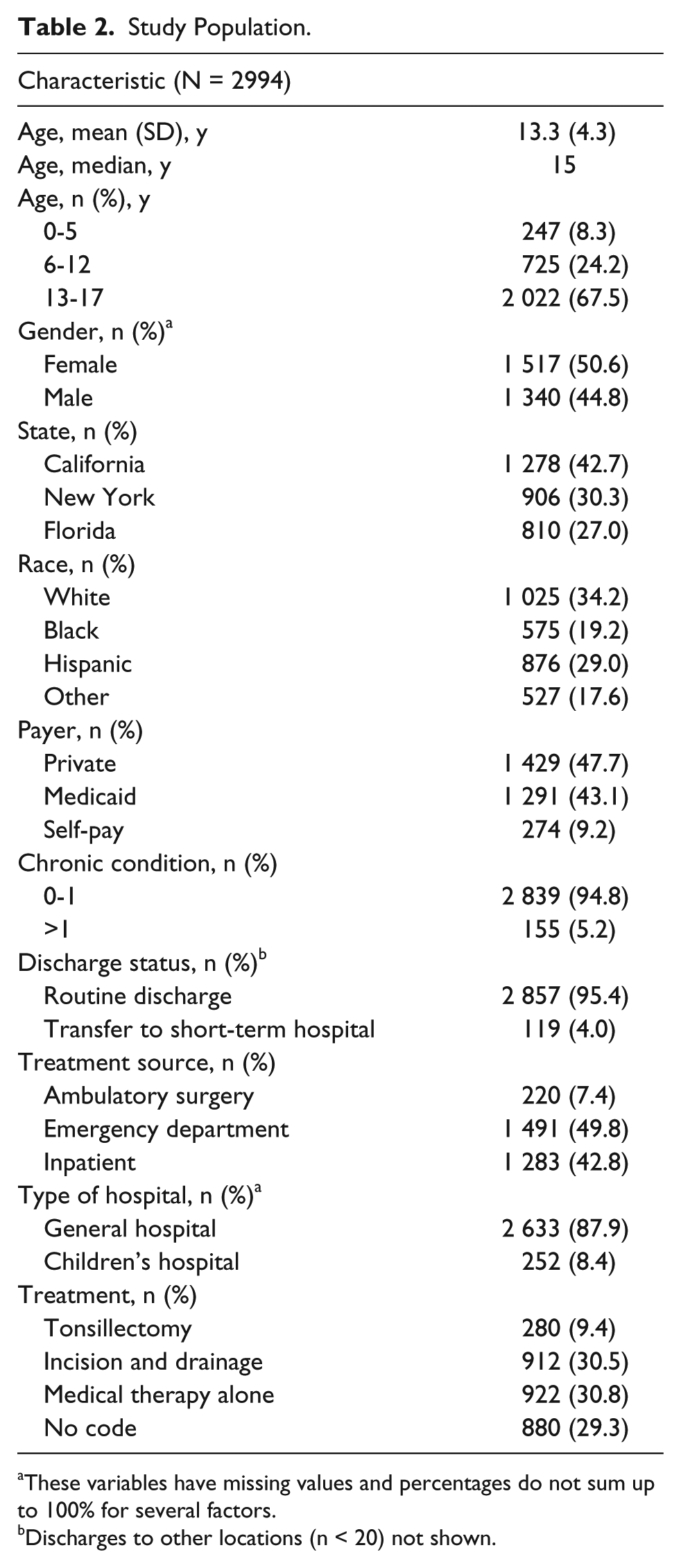
These variables have missing values and percentages do not sum up to 100% for several factors.
Discharges to other locations (n < 20) not shown.
Characteristics Stratified By Treatment.
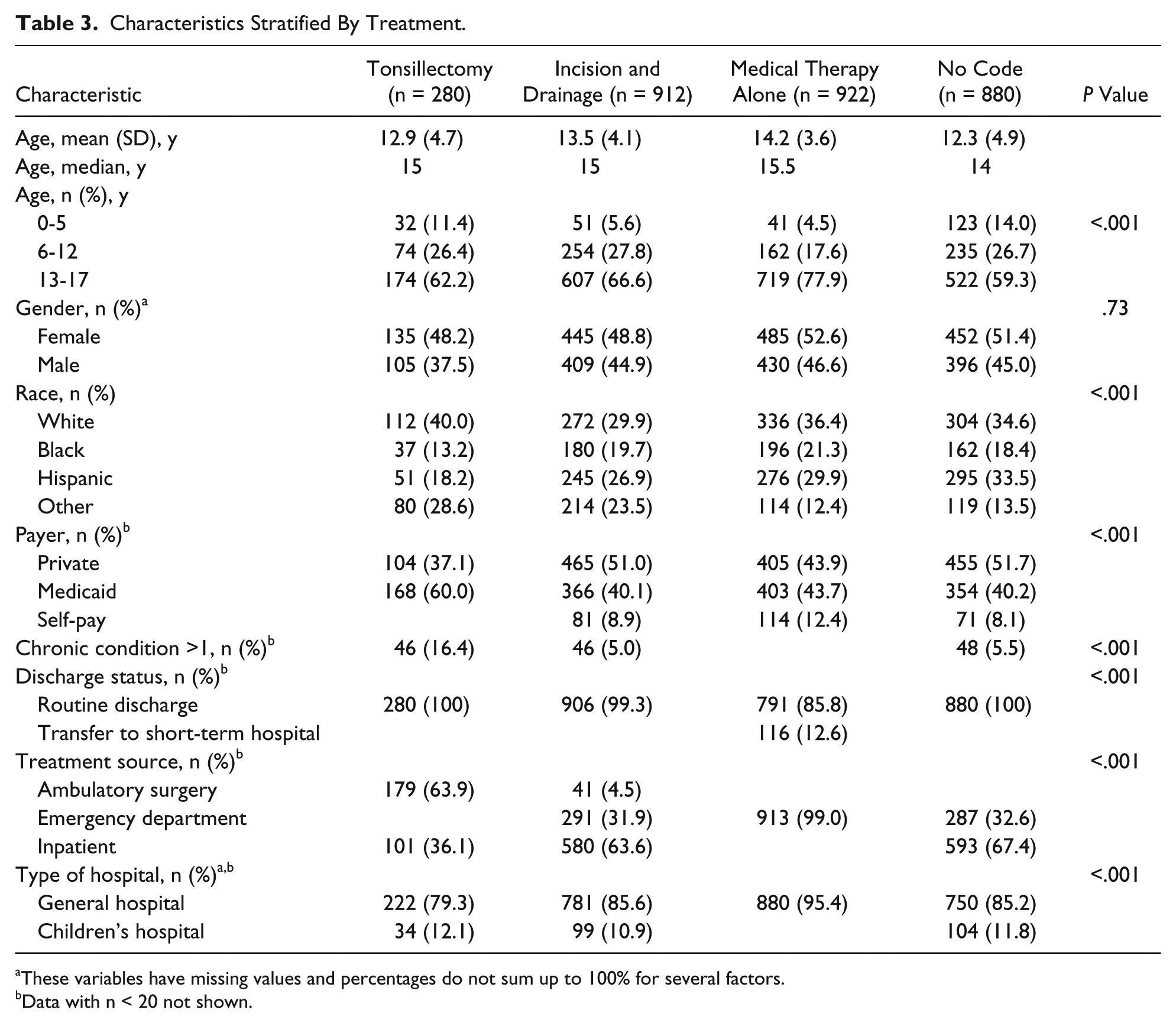
These variables have missing values and percentages do not sum up to 100% for several factors.
Data with n < 20 not shown.
Patients aged 13 to 17 years represented the majority group diagnosed with PTA/PTC, followed by 6- to 12-year-olds and 0- to 5-year-olds (67.5%, 24.2%, and 8.3%, respectively, P < .001). Overall, 9.4% of patients received tonsillectomy, 30.5% received IND, 30.8% received medical therapy alone, and 29.4% of patients had no procedural codes recorded for their diagnosis of PTA/PTC.
The majority of patients in our study population were white, followed by Hispanic, Black, and then other races (34.2%, 29.0%, 19.2%, and 17.6%, respectively). Black patients represented the lowest proportion of patients who received surgical methods of treatment: tonsillectomy and IND (13.2% and 19.7%, respectively). Additionally, despite Hispanic patients representing the second largest proportion of patients, this group received a smaller proportion of tonsillectomy procedures compared to whites and other races (18.2% vs 40.0% white, 28.6% other races).
The private payer group represented the largest proportion of patients, followed by Medicaid and self-pay (47.7%, 43.1%, 9.2%, respectively). Despite this trend, Medicaid patients represented the greatest proportion of patients receiving tonsillectomy (60.0% vs 37.1% private payer, with the self-payer group having too small a sample size to report). The medical therapy group had the largest proportion of patients who were self-payers compared with other treatment groups (12.4% vs 8.9% IND, 8.1% no code, with the tonsillectomy group having too small a sample size to report).
The majority of patients in our study were seen at a general hospital (87.9%) compared with a children’s hospital (8.4%). The tonsillectomy group had a larger proportion of patients seen at a children’s hospital compared with other treatment groups (12.1% vs 10.9% IND, and 11.8% no code, with the medical therapy group having too small a sample size to report). Alternatively, the medical therapy group had a larger proportion of patients seen at a general hospital compared with other treatment groups (95.4% vs 79.3% tonsillectomy, 85.6% IND, 85.2% no code).
In the adjusted logistic regression model (Table 4), being Hispanic was independently associated with a decreased likelihood of receiving a tonsillectomy procedure compared with being white (odds ratio [OR] 0.60, 95% confidence interval [CI] 1.26-2.55; P < .05). Additionally, there was a 2-fold increase in likelihood of receiving a tonsillectomy for the Medicaid group compared with the private payer group (OR 2.07, 95% CI 1.53-2.80; P < .001); the opposite trend was seen with the self-pay group, who were significantly less likely to receive a tonsillectomy compared to the private payer group (OR 0.47, 95% CI 0.22-0.99; P < .05). Correspondingly, self-pay was also independently associated with an increased likelihood of receiving medical therapy alone (OR 1.60, 95% CI 1.20-2.14; P < .01). Compared with children seen at a general adult hospital, those seen at a designated children’s hospital were more likely to receive tonsillectomy (OR 1.70, 95% CI 1.12-2.65; P < .05) and less likely to receive medical therapy alone (OR 0.16, 95% CI 0.09-0.27; P < .001). Having more than 1 chronic condition was also associated with an increased likelihood of receiving tonsillectomy (OR 4.80, 95% CI 3.16-7.29; P < .001). There were also significant differences in care between the 3 states, with Florida (OR 1.58, 95% CI 1.26-1.98; P < .001) and New York (OR 1.65, 95% CI 1.34-2.04, P < .001) both more likely to administer medical therapy alone compared with California.
Characteristics Associated With Treatment Choice.
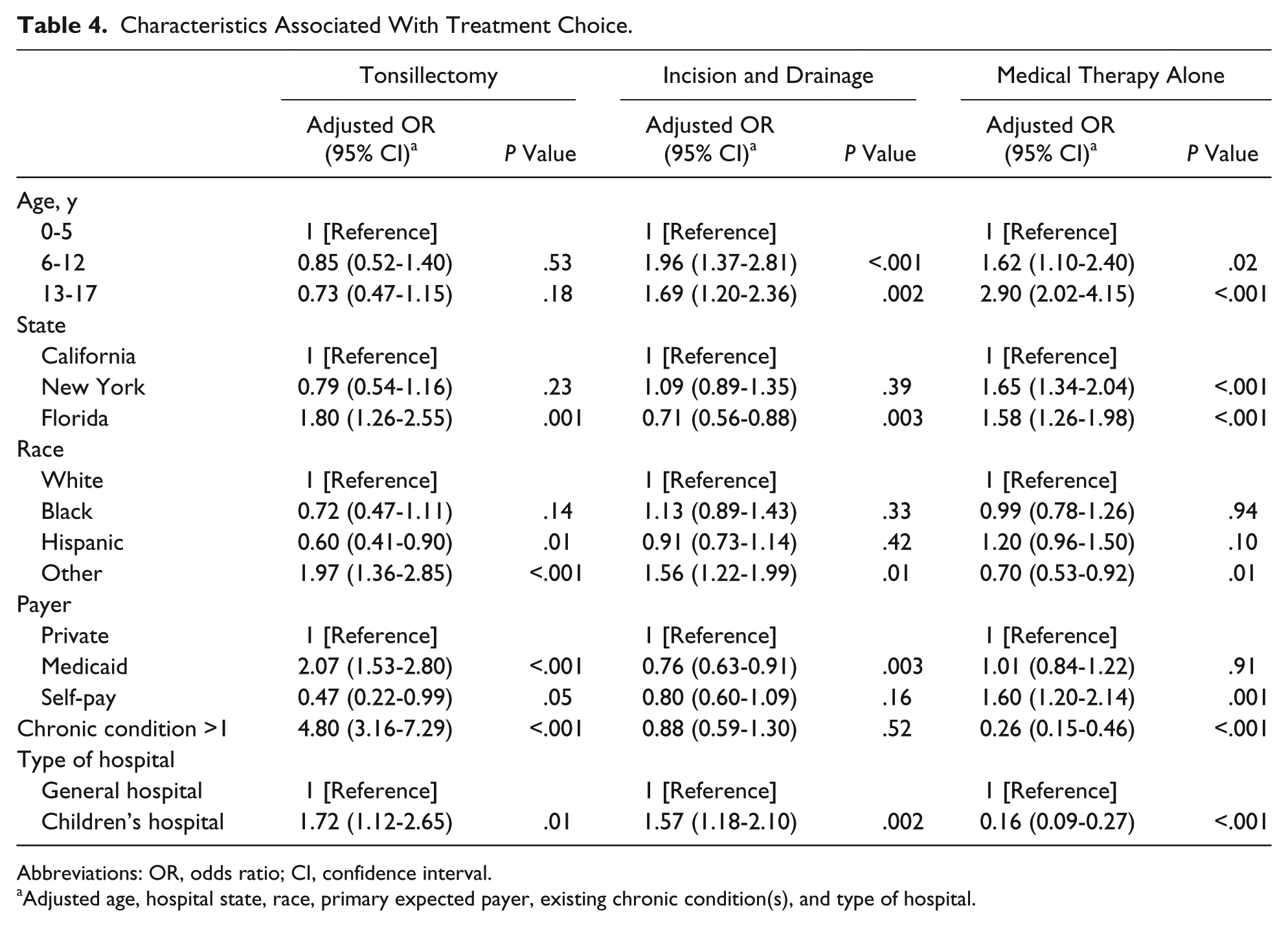
Abbreviations: OR, odds ratio; CI, confidence interval.
Adjusted age, hospital state, race, primary expected payer, existing chronic condition(s), and type of hospital.
Discussion
In this study, we report on variation in patient and hospital characteristics for treatment of children presenting with PTA/PTC in 3 large and diverse US states. We found significant variation in PTA/PTC treatment received based on nonclinical factors, including race and primary expected payer. Additionally, we found that hospital type was also associated with treatment received, with pediatric hospitals more likely to provide surgical treatment for PTA/PTC compared with general hospitals.
Our current study revealed that Hispanic patients were less likely to receive surgical therapy for PTA/PCA compared to whites after accounting for important confounding variables, consistent with previous literature.13,14 These differences in care received may be attributed to multiple factors, including patient preferences, provider practices, and language barriers.15,16 Alternatively, these differences may also have been due to clinical variations we could not control for given the level of detail our data provided.
We also found that treatment received for PTA/PTC was associated with primary expected payer. While patients in the self-pay group were less likely to receive tonsillectomy and more likely to receive medical therapy alone, Medicaid patients were more likely to receive tonsillectomy compared to patients in the private payer group. This supports a recently published study that shows an independent association between payer status and hospital resource utilization, with Medicaid pediatric patients accruing greater total charges and longer hospital stays compared with patients with private payer insurance. 17 Consistent with other reports, it is possible these Medicaid patients have limited access to primary care and therefore presented to the acute setting with more severe clinical features on the PTA/PTC disease spectrum, which would then require surgical procedures beyond medical therapy alone.18-20 Additionally, physicians aware of this access issue may also choose to treat with tonsillectomy rather than refer them to outpatient care to prevent worse outcomes due to poor access to follow-up care. 21 It is also worth noting that it has been shown that otolaryngologists are more likely to provide consultation to children with private insurance compared to public coverage. 22 While the reasons for differences in tonsillectomy utilization between self-pay and Medicaid patients are likely to be multifactorial, a probable determinant includes Medicaid’s reimbursement for tonsillectomy. 23 Taken altogether, these studies reveal that primary payer status is a complex variable that influences treatment choices for children presenting with PTA/PTC.
Interestingly, in our comparison between general and children’s hospitals, we found that patients who were cared for at a designated children’s hospital were more likely to receive tonsillectomy and IND in addition to medical therapy. No other studies to our knowledge have reported these differences between care locations as it pertains to treatment of pediatric PTA/PTC. Prior research comparing pediatric trauma care at children’s hospitals and adult hospitals conclude that children’s hospitals are more likely to have the resources and expertise readily available to manage their specialized patient population. 24 This may translate to the acute, adult hospital setting where a pediatric otolaryngology consultation may not be immediately available to contribute to management decisions of PTA/PTC. Alternatively, it is also possible that, despite receiving fewer PTA/PTC cases, children’s hospitals are more likely to treat with tonsillectomy or IND because the cases they receive are more severe. Outpatient pediatricians may also refer severe cases directly to a children’s hospital. Our data were not able to provide the level of clinical detail required for this assessment.
Additionally, no other studies have reported cases in which treatment was not recorded for PTA/PTC. Cost variables included in the discharge files revealed that charges were billed for the visit, indicating that therapy was administered. However, the lack of procedural code documentation limits our ability to assess the type of therapy this cohort of patients received. Roughly half of these patients belonged to the private payer group (data not shown), which includes Blue Cross, commercial carriers, and private health maintenance organizations and preferred provider organizations; we speculate the possibility that these patients may have belonged to a health maintenance organization with capitation of services, which may have decreased incentive to document all services in detail. However, the lack of clinical details hinders further exploration. The reasons for the lack of documentation for the other half of patients belonging to either the self-pay group or Medicaid group remain unknown.
There were several limitations in our current study. First, our study used administrative data, which lacks fine clinical detail. As the ICD-9 diagnosis code for peritonsillar abscess also includes peritonsillar cellulitis, patients within our study suffered from a disease continuum from peritonsillar cellulitis to true abscess and we lack the clinical data to confirm the latter. For patients who presented with severe clinical symptoms and clear abscess formation, surgical therapy may have been clearly indicated; whereas for patients who presented with mild clinical symptoms, medical therapy may have been clearly indicated. However, we are most interested in the children who fall in the middle of this disease continuum, where the choice for therapy may not be immediate clear. The differences we observe in our current study suggest potential biases that warrant further research. Additionally, documentation standards vary across health care providers and facilities; a lack of consistent reporting may lead to misclassification bias. Similarly, our cohort of patient is based on admissions and we lack definitive information on patients initially seen in an outpatient setting by a primary care provider. It is likely that the cohort of patients presenting to the hospital are sicker than those who were able to seek primary care in their doctor’s office. However, even give these limitations, our study provides initial evidence regarding differences that may affect how patients who present with PTA/PTC are treated in the acute setting.
Our current study has implications on multiple levels. On a clinical practice level, our findings offer insight on different trends and preferences for treatment options that providers have chosen for various types of patients, in different environments. These offer opportunities for further questions and research into the variations that were seen. On a policy level, we must advocate for the improvement of electronic documentation with regard to both completeness and finer level of detail. This is particularly necessary in the vulnerable pediatric population who present to the acute setting with a common infection that puts them at risk for respiratory compromise. With better documentation and data, not only can we track trends over time for quality improvement, but we can also perform additional research focused on specific clinical characteristics associated with treatment. This could help us better understand the reasons for these differences in care and how they may affect health outcomes. Taken together, these steps will ultimately allow medical care providers to make more clinically informed decisions regarding treatment choices.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: All phases of this study were supported by Stanford University School of Medicine and Agency for Healthcare Research and Quality.