
Abstract

DiGeorge syndrome is characterized by thymic hypoplasia and diminished T-cell numbers, and is associated with a wide spectrum of phenotypic features that include cardiac anomalies, dysmorphic facial features and hypocalcemia. Limited data exist about immunologic characteristics of pediatric patients with partial DiGeorge syndrome. The objective of our study was to better characterize the immune parameters and correlate these values to vaccine responses of patients with partial DiGeorge syndrome.
Methods
This was a retrospective study of pediatric patients attending University of Minnesota Masonic Children’s Hospital from 2006 to 2012. Patients with a diagnosis of DiGeorge syndrome were identified, their charts reviewed and immunologic data were abstracted. To be included in the study, they were required to have received the Haemophilus influenzae type B (Hib) vaccine, pneumococcal conjugate vaccine (either 7-valent or 13-valent), diphtheria vaccine, and tetanus vaccine. Immunologic testing done at, or closest to, the time of vaccine titer measurements were included. Patients who did not have titers for the above-mentioned vaccines nor complete immunologic testing, including T- and B-cell subsets, lymphocyte mitogen proliferation, and immunoglobulin levels, were excluded. This study was approved by the University of Minnesota Institutional Review Board.
Results
A total of 107 pediatric patients with DiGeorge syndrome were identified, of which complete immunologic and vaccine titer records were available for 12 (Table 1). Of the 12 patients, 6 (50%) were male. Mean age at which vaccine titers were checked was 3 years 10 months. All patients had protective responses to diphtheria and tetanus vaccines. Overall mean Hib titer was considered protective, though three patients had nonprotective Hib titers. Three patients had protective titers to more than half of the pneumococcal serotypes tested. All but one patient had normal T, B, and NK cell levels; that patient had a moderate decrease in CD4 and CD8 counts, but normal immune globulin levels for age. All but one patient had normal immune globulin levels; the remaining patient had borderline levels of IgG and low levels of IgA and IgM, but T, B, and NK cell levels were within normal range for age. Ten out of 12 patients had normal lymphocyte responses to phytohemagglutinin.
Characteristics of Immunologic Studies in 12 Pediatric Patients With Partial DiGeorge Syndrome.
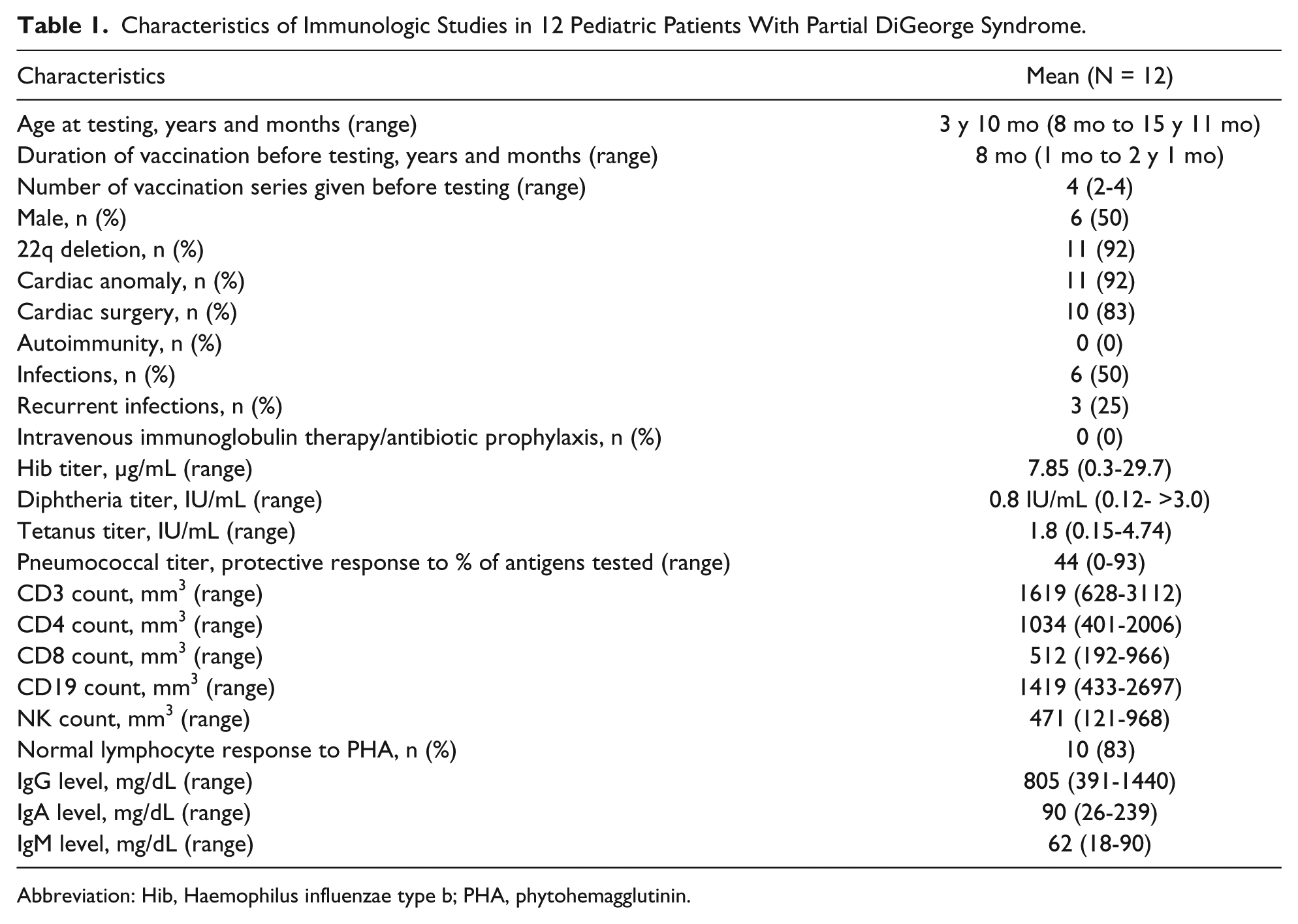
Abbreviation: Hib, Haemophilus influenzae type b; PHA, phytohemagglutinin.
Of the 3 patients who had nonprotective Hib titers, immune parameters were within normal range (average CD3 count 2281 mm3, CD4 count 1536 mm3, CD8 count 606 mm3, NK count 947 mm3, IgG 712 mg/dL, IgA 33 mg/dL, IgM 58 mg/dL). Two of the 3 had normal lymphocyte responses to phytohemagglutinin, the third had low-normal response. One of the 3 also did not have a protective response to any of the pneumococcal serotypes, although she had normal T, B, and NK cell levels, normal immune globulin levels and normal response to phytohemagglutinin.
Discussion
Slow declines in T cell population with preservation of T cell function, as well as hypogammaglobulinemia, have been observed in patients with 22q deletion syndrome,1,2 although exceptions have been noted. 3 However vaccination, including live vaccines, is well tolerated, generates appropriate antibody responses and has a similar incidence of adverse effects.4,5
In our study, the majority of children with partial DiGeorge syndrome had immunologic parameters within the normal range for age, as well as good responses to diphtheria and tetanus vaccines. Almost a third did not have a protective response to Hib vaccines, although their immunologic characteristics were within normal range. Protective response to pneumococcal vaccines was most problematic, with only 3 patients responding to at least half of the pneumococcal serotypes tested.
Interpreting humoral immunity can be challenging as vaccine responses can be affected by antibody repertoire, antigen-specific immune responses, immunologic memory, and specific avidities for antigens. 6 Protein-conjugated Hib and pneumococcal vaccines have been recognized to show variability in immunogenicity based on the protein carrier used in conjugate vaccines to elicit T-cell help from the mutant diphtheria protein CRM 197 (HbOC or polyribosylribitol phosphate, PRP-CRM), to meningococcal protein conjugate (PRP-OMP, outer membrane protein complex of Neisseria meningitidis), or tetanus toxoid (PRP-T).6-8 In patients with 22q deletion syndrome, poor responses to pneumococcal polysaccharide vaccine have been described. 9 This is in contrast to protein antigens or toxoids such as tetanus or diphtheria vaccines, which demonstrate no significant immunogenic variability. 6
There are several limitations to this study. Most studies demonstrating immune deficiency were noted in children over several years of age. 2 As the mean age in our study was 3 years 10 months, young age may have masked such observations. As this was a retrospective study, additional testing was not done in patients who did not respond to their vaccines to further evaluate their immune system, as has been described in other studies. 9 One study showed a statistically significant decrease in IgM+ IgD+ CD27+ B cells, which was associated with recurrent infections. 9 It would have been of interest to have determined whether the children in the current study with poor antibody production following certain immunizations had such a deficiency, since that subset of B cells may operate as memory B cells. 10 This study was also limited by the small number of patients available for analysis, as we restricted our analysis to those who had complete immunologic records, to allow for comparison of immunologic values and correlation with vaccine responses.
In conclusion, children with partial DiGeorge syndrome can generally generate good antibody responses to vaccines. As early diagnosis and management of invasive Hib and pneumococcal disease is important in achieving a good outcome, postvaccination serologies should be obtained to document protective responses as well as to identify patients for whom revaccination should be considered. Further studies to investigate whether diminished serum antibody to certain immunogens occurs in some children with DiGeorge syndrome due to a selective deficiency in T helper cells or to other mechanisms, and to investigate the antibody and T-cell receptor repertoires in those types of patients correlated with the degrees of specific immune responses, are warranted.
Footnotes
Authors’ Note
This work was presented at Pediatric Academic Societies Meeting in Vancouver, British Columbia, Canada, in May 2014.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: PI has received an investigator-initiated grant from Pfizer. SCM has no relevant conflicts to disclose.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.