
Abstract
Background. Acid-suppressing agents have been associated with increased Clostridium difficile infection (CDI) in adults. The objective of this study was to evaluate the association of acid-suppressing therapy with the development of CDI in the pediatric population. Methods. This was a retrospective case-control study. Children aged 1 through 17 years with a positive C difficile polymerase chain reaction (PCR) result obtained between June 1, 2008, and June 1, 2012, were randomly matched to a control population selected from patients with negative PCR. Results. A total of 458 children were included. No difference was observed in acid-suppressive therapy prior to PCR in CDI-positive versus -negative patients (n = 131 [57.2%] vs n = 121 [52.8%], P = .348). Among patients receiving acid-suppressing therapy prior to obtaining a PCR, no difference was observed in proton pump inhibitor use (45% vs 46.3%, P = .843), but histamine-2 receptor antagonist (H2RA) use was greater in the CDI-positive patients (32.8% vs 14.9%, P = .001). Logistic regression analysis demonstrated that H2RA therapy at home (odds ratio = 4.6; 95% confidence interval = 1.5-14.5) was an independent CDI predictor. Conclusion. In this pediatric population, CDI risk in children receiving home acid-suppressive therapy with H2RAs is nearly 4.5 times greater than that of children not receiving H2RA therapy. These results suggest the need for continued monitoring and study of H2RA therapy in children.
Background
In children, Clostridium difficile infection (CDI) is the most common cause of hospital-associated diarrhea. The incidence of CDI has increased over the past several years, with recent studies estimating it to be between 9% and 14% in hospitalized children.1-3 The clinical outcome of CDI in children varies widely, from asymptomatic colonization to severe colitis. 4 A growing number of children with CDI are being admitted to the intensive care unit and are experiencing a higher incidence of complications, including toxic megacolon or gastrointestinal perforation. There is also an increased length of hospitalization, contributing to increased health care costs. 5 The estimated CDI-associated mortality in pediatrics is approximately 4%. 6 Risk factors in the pediatric population have been identified and include exposure to antibiotics and immunosuppressants; comorbidities, such as cancer and cystic fibrosis; and hospitalization. 7
In adults, a major risk factor that has been recently identified is exposure to acid suppressants. 8 Proton pump inhibitors (PPIs) and histamine-2 receptor antagonists (H2RAs) have been shown to increase the risk of CDI by odds ratio (OR) = 1.74 (95% confidence interval [CI] 1.47-2.85; P < .001) and 1.44 (95% CI = 1.22-1.7), respectively.9,10 In 2012, the Food and Drug Administration, following several studies demonstrating a correlation between CDI and acid suppressants, issued a safety announcement declaring PPIs and H2RAs as CDI risk factors in adults. 11
Although some risk factors are similar between the adult and pediatric population, there has been contradictory information regarding the risk of CDI with the use of PPIs or H2RAs in children, despite overuse in the pediatric population.5,11-16 Because of the increasing incidence of CDI and inconclusive results regarding acid-suppressing agents being a risk factor in the pediatric population, the objective of this study was to evaluate the association between acid-suppressing therapy and CDI in the pediatric population.
Methods
This was a retrospective case-control study. Children aged 1 through 17 years who were admitted to our free-standing pediatric hospital between June 1, 2008, and June 1, 2012, were eligible for study inclusion. Patients were defined as having a CDI if they had a positive quantitative real-time polymerase chain reaction (qPCR) for the presence of toxin B from a diarrheal stool specimen and if they exhibited symptom(s), such as fever, diarrhea, and abdominal pain, as documented in the electronic medical record. 17 Patients with a positive qPCR were randomly matched using a random number generator 1:1 to a control selected from patients with the same inclusion criteria and a negative qPCR during the same period. Demographic data as well as information on the use of acid-suppressing agents prior to PCR, presence of CDI risk factors, and prior exposure to specific medications were extracted from medical records (eg, if the patient was receiving an acid-suppressing agent at home or if the patient was given one in the hospital in the past 3 months). Possible CDI risk factors, including hospitalization within the 3 months prior to study encounter, duration of hospitalization prior to PCR, comorbid conditions, prior antibiotic use, and use of oral steroids, immunosuppressants (defined as mycophenolate, tacrolimus, sirolimus, lefunomide, cyclosporine, methotrexate, anti-thymocyte globulin, azathioprine), prokinetic agents (defined as metoclopramide, cisapride, erythromycin), or chemotherapeutic agents were recorded. Exposure to all suppressing agents, antibiotics, steroids, and immunosuppressants was defined as the patient receiving therapy for at least 1 day prior to qPCR. Exposure to chemotherapy was defined as exposure within 3 months of the positive qPCR. Home acid suppression was defined as a patient having an acid-suppressing agent on their admission medication reconciliation form in the electronic medical record.
Data Analysis
Control and CDI groups were compared using independent-samples t tests, χ2 analyses, and Mann-Whitney tests for nonparametric data. Logistic regression analysis of CDI was utilized using a forced entry method. Variables were included in the final regression model if the P value was <.25 after univariate analysis. P values <.05 were considered to be statistically significant. Statistical analyses were conducted using Statistical Package for Social Sciences version 19.0 (SPSS, Inc, Chicago, IL). The study was approved by the Indiana University Institutional Review Board.
Results
During the study period, 229 CDI-positive cases were identified as meeting inclusion criteria and were matched with 229 CDI-negative cases. Group characteristics are displayed in Table 1. Acid-suppressive therapy information for the 2 groups is displayed in Table 2. The most common PPI utilized in both groups was lansoprazole, whereas the most common H2RA was ranitidine. The most common comorbidities in both groups included respiratory disorders and neurological disorders. The most frequent comorbidity for the CDI-negative group was transplant and for the CDI-positive group, it was the comorbidity of cancer. Antibiotic exposure was observed in 66.8% of the CDI-positive group and 60.7% of the CDI-negative group (P = .174). Neither receipt of chemotherapy nor previous hospitalization was associated with CDI in this sample. Immunosuppressive therapy was present in 16.6% of the CDI-positive group versus 29.3% of the negative group (P = .001). Additional analyses of risk factors are displayed in Table 3. Following multivariate logistic regression analysis, H2RA therapy at home (OR = 4.6; 95% CI = 1.5-14.5) was independently associated with CDI.
Baseline Characteristics.
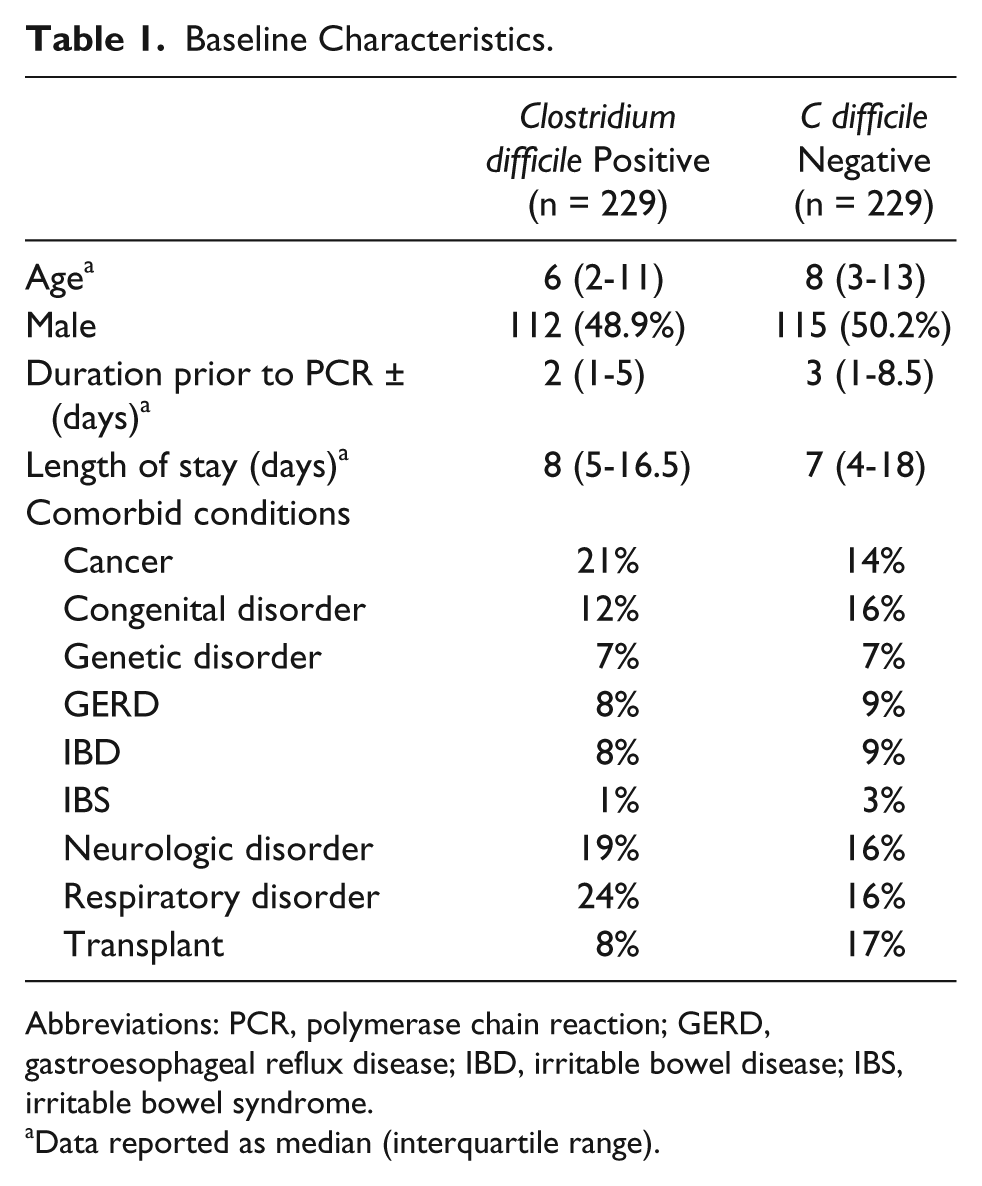
Abbreviations: PCR, polymerase chain reaction; GERD, gastroesophageal reflux disease; IBD, irritable bowel disease; IBS, irritable bowel syndrome.
Data reported as median (interquartile range).
Acid Suppression.
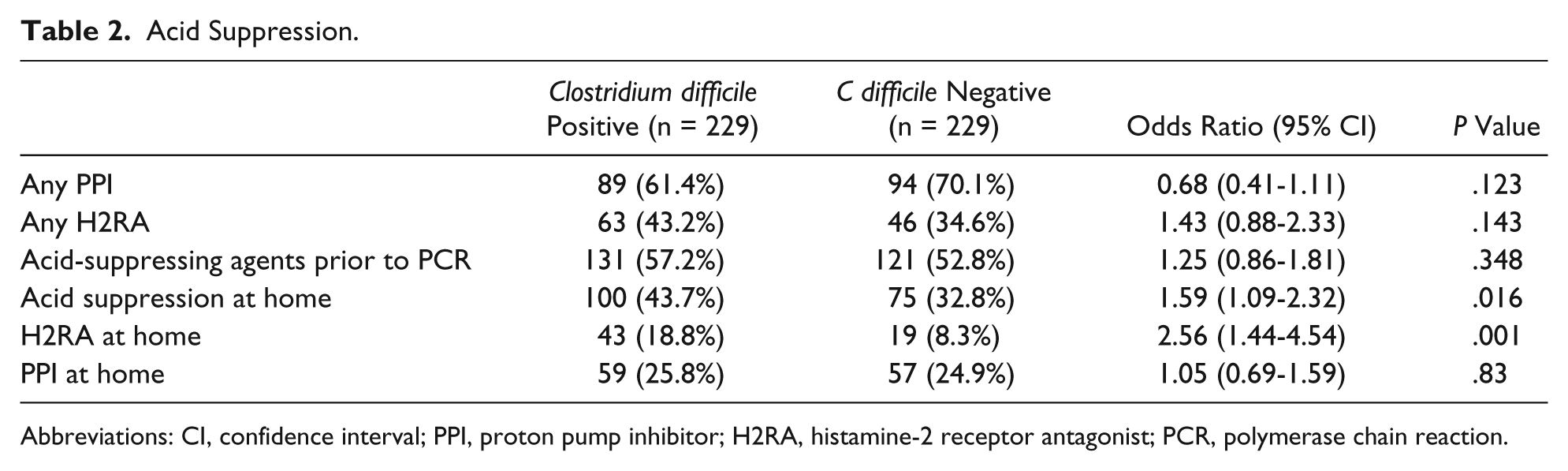
Abbreviations: CI, confidence interval; PPI, proton pump inhibitor; H2RA, histamine-2 receptor antagonist; PCR, polymerase chain reaction.
Other Potential CDI-Associated Factors.
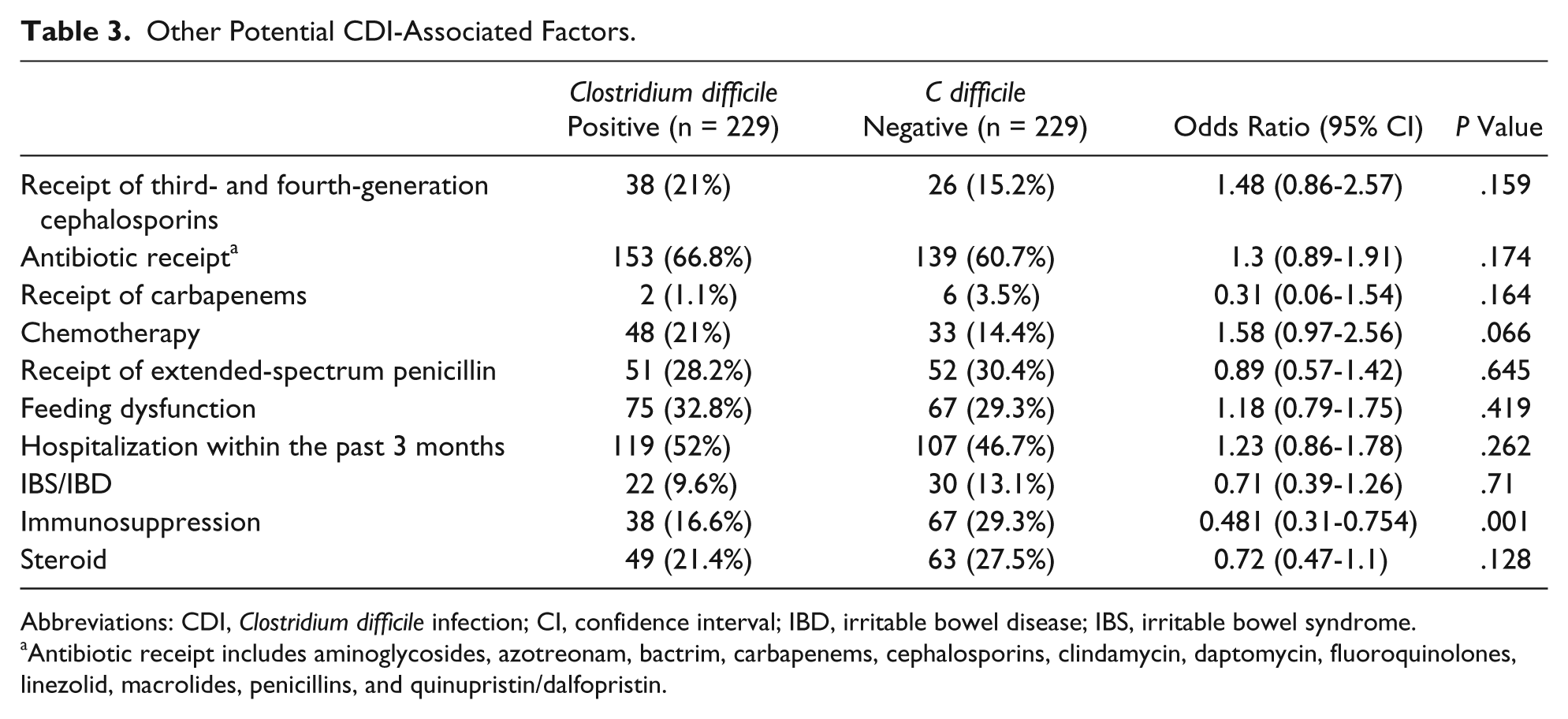
Abbreviations: CDI, Clostridium difficile infection; CI, confidence interval; IBD, irritable bowel disease; IBS, irritable bowel syndrome.
Antibiotic receipt includes aminoglycosides, azotreonam, bactrim, carbapenems, cephalosporins, clindamycin, daptomycin, fluoroquinolones, linezolid, macrolides, penicillins, and quinupristin/dalfopristin.
A subgroup analysis performed on patients receiving acid-suppressing agents prior to PCR showed that more CDI patients received home acid-suppressive therapy (76.3% vs 60.3%, P = .006). Home PPI use did not differ (45% vs 46.3%, P = .843) between CDI-positive and -negative patients. The odds of CDI increased nearly 3 times for patients receiving any H2RA therapy at home (OR = 2.8; 95% CI = 1.5-5.2). Other CDI-associated factors were similar between groups in this subgroup analysis.
Discussion
The exact mechanism behind the increase in CDI risk with the use of PPIs or H2RAs has not been fully evaluated, though a common theory is that acid suppressants may have a direct negative effect on the patient’s immune function. Because normal gastric acid secretion acts as a barrier for enteric pathogens, a higher pH in the stomach is thought to lead to the proliferation of various species of bacteria including C difficile. 18 Current pediatric literature regarding PPI and H2RA use and development of CDI is limited and inconclusive. In 2009, a retrospective, case-control study of 68 patients found that children exposed to PPIs were 4.5 times more likely to become infected with C difficile than children who were not exposed to a PPIs. A statistically significant difference in the children exposed to an H2RA in that study was not found. Alternatively, a study conducted in 2011 by Pohl et al 12 found that the use of PPIs in 215 pediatric patients with cystic fibrosis was not a risk factor for CDI. Rexach et al 14 examined the epidemiology of C difficile in pediatrics and found that H2RAs were not a risk factor; PPIs were not evaluated in this study. Samady et al 7 evaluated predictors of C difficile in hospitalized children and found that PPIs were not a risk factor but did not examine H2RAs. Blank et al 13 analyzed the effect on children with cancer and found that children were less likely to develop CDI on a H2RA but more likely on a PPI. Most recently, Nylund et al 15 evaluated the use of H2RAs and PPIs through electronic medical records and found that both are risk factors for the development of CDI and recurrent CDI.
In this study, we found that children who receive H2RAs prior to hospitalization (documented as a home medication through admission medication reconciliation) were at nearly 3 times the risk of developing CDI. H2RAs can raise the gastric pH to greater than 5, which has been shown to increase the survival of the vegetative form of C difficile, which is the active growth phase of the organism. 19 For example, famotidine depending on the dosage form and dose, can increase gastric pH to greater than 4 for about 20 hours. 18 In contrast, children who were prescribed a H2RA only on hospitalization but prior to PCR were not at increased CDI risk, suggesting that short-term therapy may not be as clinically concerning. Although we did not account for average duration of acid-suppressive therapy, the average inpatient duration prior to PCR was recorded. The mean duration for CDI positive was approximately 8 days, and the mean duration for CDI negative was 5 days.
As evidence of severe clinical outcomes such as toxic megacolon, colectomy, sepsis, and death in children with CDI continues to accumulate, it becomes even more important to understand the risk factors contributing to CDI. 14 Results from this study should be considered when prescribing an acid-suppressing agent for a child. Acid-suppressing agents have been shown to be overused in the adult and pediatric populations.16,20 It is important for pediatricians to be aware of the risks associated with these agents and to prescribe them only when appropriate. Even more important, health care professionals should ensure that they question parents regarding the use of over-the-counter medications because parents may be giving their child an acid-suppressing agent for nonindicated reasons. The use of H2RAs in the pediatric population should be monitored and further evaluated to determine possible cause and effect.
Although this is a case control study, its retrospective design is a limitation. Home medications were not always documented in the patient charts; therefore, medication use prior to qPCR was not always able to be captured. Though fewer CDI-positive patients were exposed to immunosuppressant therapy in this study, this is likely caused by an increased sampling bias and should not be misinterpreted. Additionally, acid-suppressing agents are also available over-the-counter, and often, parents and caregivers forget to tell health care professionals what medications they are taking over-the-counter. This could have affected the study because more patients may or may not have been on an H2RA or PPI. Selection bias was accounted for by randomly matching a CDI-positive participant with a CDI-negative participant, but the participants were not matched for confounding variables such as medication use and comorbidities.
Conclusion
Use of acid-suppressing agents prior to hospitalization significantly increased the risk of developing CDI. However, although we were unable to compare the exact duration of patients receiving acid suppression at home, initiation of acid-suppressive therapy following hospital admission did not increase the risk of infection. Additionally, of the children receiving acid-suppressing agents prior to hospitalization, those taking H2RAs (as compared with those who were not taking H2RAs) had a nearly 4.5 times higher rate of risk of infection with C difficile. The use of H2RAs in the pediatric population should be monitored and further evaluated prospectively to determine possible cause and effect.
Author Contributions
All authors have made substantial contributions to conception and design, and/or acquisition of data, and/or analysis and interpretation of data; participated in drafting the article or revising it critically for important intellectual content; and gave final approval of the version to be submitted and any revised version.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.