
Abstract

Case Report
A 22-month-old Caucasian boy, former term newborn, was transferred from an outside hospital for persistent respiratory distress. His medical history was significant for dysphagia controlled with thickened foods and 2 remote episodes of bronchiolitis. One week prior to presentation, his mother noted wheezing with intermittent increased work of breathing. During multiple visits to the physician, he was treated with antibiotics, β-agonists, and steroids with partial return of symptoms. On the day of admission, after lunch, he developed a persistent cough with wheezing. His mother denied any history of fever, rhinorrhea, vomiting, introduction of new foods, or known sick contacts during this time. He was taken to his primary care physician that same day, but was sent to the local emergency room due to his deteriorating respiratory status.
Hospital Course
On arrival to the outside hospital his vital signs were as follows: temperature 36.7°C, blood pressure 101/64 mm Hg, heart rate 187 bpm, respiratory rate 50, SpO2 89% on room air. He was given intravenous methylprednisolone and magnesium sulfate before initiation of continuous inhaled bronchodilators. With only minimal improvement in his respiratory status, the decision was made to escalate his care. He was transported to a tertiary pediatric intensive care unit (PICU) but en route became hypoxemic with seizures and required bag-mask ventilation. On arrival to the PICU, he was in obvious respiratory distress with nasal flaring and grunting. Physical examination revealed diffusely coarse breath sounds with minimal air movement bilaterally, a prolonged expiratory phase, and bilateral monophasic expiratory wheezing. Because of failure to respond to bronchodilators and altered mental status, immediate endotracheal intubation and mechanical ventilation were required. Initial chest radiograph (CXR) confirmed placement of support lines and tubes but showed hyperinflation of the left lung and rightward mediastinal shift with right lung partial atelectasis (Figure 1A). His laboratory investigations were significant for white blood cell count of 25 180/µL with neutrophil predominance, hemoglobin 12.6 g/dL, hematocrit 38%, platelets 515 000/µL, serum bicarbonate of 22 mmol/L, and calculated anion gap of 12. A multiplex respiratory pathogen panel (FilmArray Respiratory Panel, Biofire Diagnostics, Inc, Salt Lake City, UT) was positive for enterovirus/rhinovirus.
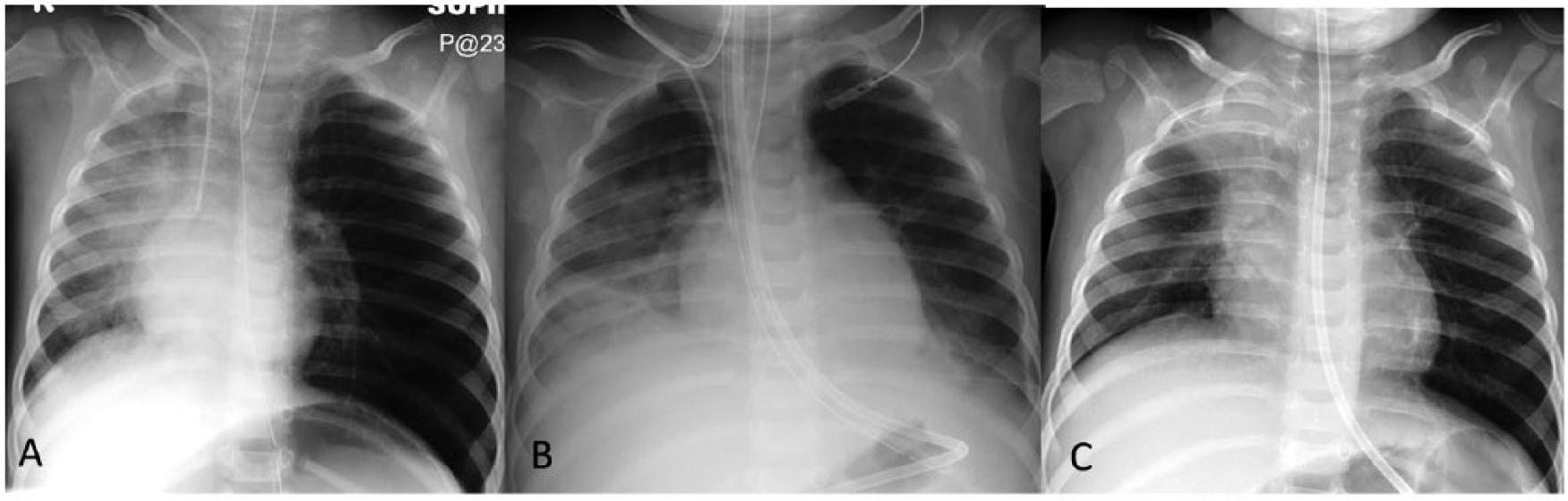
(A) Initial CXR shows left lung hyperinflation, flattened left hemidiaphgram, rightward mediastinal shift, partial atelectasis of the right lung, and gaseous distension of the stomach. (B) CXR on hospital day #4 with bibasilar infiltrates, left upper lung hyperinflation, and bilateral mild pleural effusions. (C) CXR post extubation with atelectasis in right upper lobe and resolution of left lung hyperinflation.
Despite maximal medical management with steroids and bronchodilators for presumed status asthmaticus, he continued to be in respiratory failure. Daily CXRs were obtained and imaging on hospital day 4 showed bibasilar opacities and bilateral mild pleural effusions both greater on the right (Figure 1B). He remained on ventilatory support in pressure-regulated volume control mode with positive end-expiratory pressure of 10 cm H2O and documented PCO2 levels upwards of 70 mm Hg. Computed tomography (CT) of the chest (Figure 2A) showed endobronchial masses in the left main bronchus and right bronchus intermedius with consequent air trapping in the entire right middle and lower lobes and partial atelectasis of the right upper lobe. He underwent bedside flexible bronchoscopy confirming peanut remnants in the bilateral mainstem bronchi. He was taken urgently to the operating room for foreign body removal via rigid bronchoscopy after which he had a rapid and drastic improvement in his respiratory status. He was quickly weaned off ventilatory support and extubated to 3 L/min heated humidified high-flow nasal cannula. Shortly after extubation, he again began having frequent episodes of hypoxemia. CXR at that time showed persistent and increased right upper lobe atelectasis, and repeat bronchoscopy showed a remaining peanut particle covered by granulation tissue.
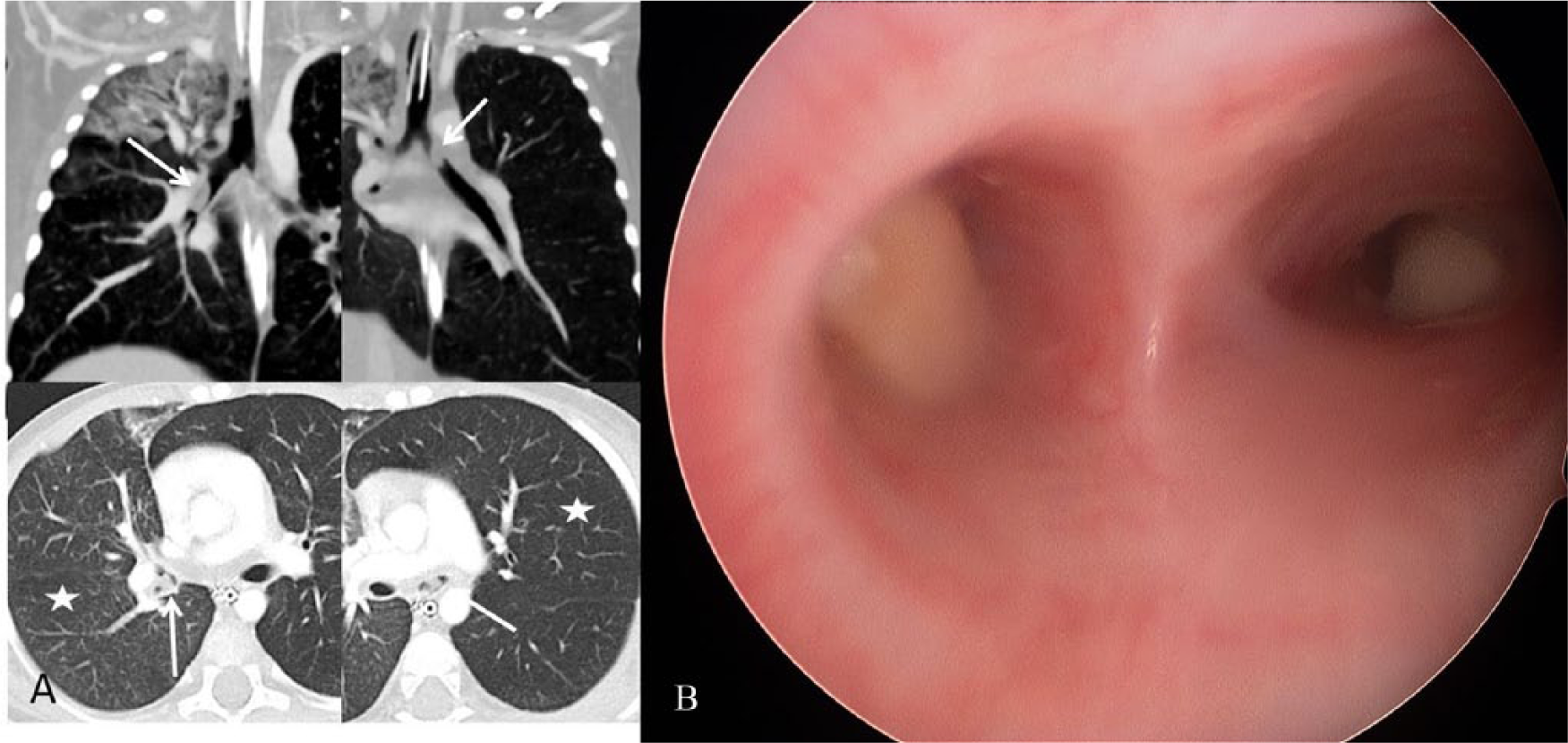
(A) Coronal mediastinal and axial lung window CT images show obstructing endobronchial masses (arrows) in right bronchus intermedius and left main bronchus with hyperinflation of left lung, right lower lobe and right middle lobe (stars). (B) Rigid bronchoscopy revealing peanut remnants in bilateral mainstem bronchi.
Final Diagnosis
Aspiration of multiple foreign bodies with bilateral bronchial obstruction
Discussion
Foreign body aspiration (FBA) is a serious medical condition that if left untreated may lead to life-threatening complications such as asphyxiation and death. Although FBA can affect children of any age, up to 75% of cases occur in children less than 3 years of age, with a peak incidence of 1 to 2 years of age.1-3 Due to anatomical differences between the right and left mainstem bronchi, the majority of foreign bodies are found in the right mainstem bronchus (60%) and left mainstem bronchus (23%), although other locations include the larynx (2%), trachea (13%), and rarely bilateral bronchi (2%). 4
The initial evaluation of any patient presenting with respiratory distress should consist of a detailed clinical history and physical examination and ultimately be supported by radiologic evidence. The signs and symptoms of FBA depend on the site, size, composition, and period for which the foreign body has been lodged. 5 The diagnosis of FBA is not always easy, since, in most cases, parents do not witness the aspiration event; therefore, suspicion must be raised based on clinical history. Sudden onset of respiratory symptoms in a child who is not otherwise sick with a respiratory illness should raise concern. Wheezes, appreciated on chest examination, are defined as a musical or whistling lung sounds classified by timing (expiratory or inspiratory, mono- or biphasic), duration, complexity (monophonic or polyphonic), and pitch (low or high) and indicate narrowing of the airways. 6 Monophonic wheezing is more typical of local bronchial narrowing that occurs with a fixed obstruction such as a foreign body. Polyphonic wheezing is typical in patients with asthma and associated widespread airway obstruction. 7 Furthermore, wheezing should be categorized by the onset and duration of symptoms (acute vs chronic) as this can more easily identify the underlying cause of respiratory distress. Acute wheezing may reflect obstructive pathology such as FBA or lung disease such as asthma, bronchiolitis, or laryngotracheobronchitis, whereas recurrent wheezing generally signifies structural abnormalities. Wheezing that is not responsive to maximal bronchodilator therapy should alert the physician to nonasthmatic causes of wheezing such as infection, immune deficiencies, cardiac abnormalities, airway abnormalities, endobronchial obstruction, or underlying chronic disorders such as cystic fibrosis.
Radiological evaluation has been widely used to assist in the diagnosis of FBA. CXRs are primarily of use if the foreign body in question is radiopaque; however, the CXR is normal in 12% to 30% of cases and therefore does not exclude the diagnosis of FBA. The most common CXR findings in FBA are pulmonary air trapping, which manifests as hyperinflation, mediastinal shifting, atelectasis, and consolidation.2,3 Our patient had some of these findings on the initial CXR (Figure 1A) and persistent left lung hyperinflation with shifting atelectasis in the right lung for the first few days of intubation. CT scan with current low-dose techniques can be used for further evaluation of the radiographic findings, especially in patients with wheezing refractory to medical management. CT imaging can demonstrate obstructive endobronchial pathology of variable densities, evaluate enhancement pattern of the mass, identify associated lung pathology, and provide a roadmap for subsequent bronchoscopy. If obstructive pathology is found on CT imaging, conventional rigid bronchoscopy should be performed to confirm and remove the foreign body. 8 In our patient’s case, the recent history of wheezing that was intermittently treated with bronchodilators in conjunction with the presence of enterovirus/rhinovirus and lack of history of choking or peanut exposure were confounding variables that led the treatment team to believe that his wheezing was secondary to asthma unresponsive to bronchodilators. In retrospect, it was not until CT imaging showed an obstruction that his mother remembered he was eating peanuts prior to his initial coughing spell.
Conclusion
Timely diagnosis of foreign body aspiration is crucial to prevent life-threatening sequelae. Delays in diagnosis are usually associated with inattention to the signs and symptoms present in the clinical history of cough and choking, especially in children less than 3 years of age. Unfortunately, the treating physician often suspects more common causes of cough and wheezing such as asthma, especially when the aspiration event is unwitnessed or unsuspected. The longer the foreign body remains in the tracheobronchial tree, the higher the probability of complications all the while that valuable time is lost treating symptoms without the appropriate management. In conclusion, a high index of suspicion should be maintained for foreign body aspiration in patients presenting with acute onset cough, wheezing, and difficulty breathing.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.