
Abstract
Background. Research suggests that multimedia-based interventions possess advantages for disseminating safe and effective methods of behavior management to parents in pediatric primary care; however, little is known about their utilization in real-life settings. In order to maximize the impact of multimedia resources, more knowledge regarding dissemination and implementation is needed. Objective. To examine provider and parental perception and utilization of videos designed to communicate evidence-based parenting strategies for disruptive behavior. Videos were available in clinic and online. Results. Both provider and parent perceptions of the videos were largely positive. However, of 240 parents surveyed, only 33% were aware of the availability of videos subsequent to a well-child visit. Parents were unlikely to view the videos if they did not do so as part of their child’s health care visit. Conclusion. Multimedia interventions for behavior management are likely to be well received, but systematic methods of implementation are needed. Further study of dissemination of multimedia interventions is merited.
Disruptive behavior problems of early childhood (eg, noncompliance, tantrums, aggression) are common and parents are most likely to seek professional advice regarding these difficulties from their child’s primary care physician (PCP). 1 As a result, pediatric PCPs report addressing behavioral concerns more frequently than ear infections. 2 The vast majority of PCPs make nonmedical recommendations for behavioral health, 3 but doing so is disproportionally time consuming 4 and possibly inadequately reimbursed. 5 Half of pediatricians report allowing extra time for visits involving behavioral health issues 3 and time limitations lead to avoidance of behavioral counseling. 5 In addition to time barriers, most PCPs endorse a lack of behavioral health training. 3 Correspondingly, there is great variation in PCPs approaches to managing behavioral issues6,7 and interventions may lack an empirical basis. 8 Thus, it is unsurprising that anticipatory guidance regarding discipline is one of the most common unmet needs reported by parents. 9
Partially in response to these limitations, recent health care reform stresses the integration of mental and behavioral health services in primary care; however, barriers to integration persist, including a lack of qualified providers in many communities. 10 Furthermore, mental health professionals operating in primary care are often consumed by the most complicated cases, and less intense needs may go unaddressed. As such, the need exists to enhance behavioral services in primary care through methods that may not require face-to-face contact with a mental health professional.
Fortunately, many behavioral problems commonly presenting in primary care do not require mental health services to be successfully addressed. Lower intensity interventions such as informational written guidelines with nursing support 11 and multimedia presentations12,13 provide benefits beyond usual care. Scholer et al 13 have studied a brief primary care multimedia intervention designed to help parents manage child aggression and have found the intervention to be well received, successful in altering parents’ discipline plans,14,15 and perceived by parents as helpful 1 year later. 12 Multimedia-based interventions may be especially useful for addressing low-intensity but high-frequency early childhood behavior difficulties, as they hold potential to provide evidence-based information in a manner that is consistent, resource efficient, and engaging. Indeed, the near ubiquity of web-based technology has prompted an increase in digital parent-training methods. 16
While previous research indicates that disseminating evidence-based behavioral interventions in primary care via multimedia is promising, little is known regarding how such tools are used by clinicians or engaged in by parents in real-life settings. The preponderance of research has taken place in university-based clinics or within the confines of structured experimental procedures. Furthermore, previous research has focused on parent-reported outcomes, but little attention has been given to evaluating PCPs’ acceptance and utilization of multimedia resources. In order for multimedia-based interventions to be widely used, adaptation to heterogeneous clinicians and settings is likely necessary. Furthermore, as digital technology proliferates, options for delivering media are multiplying, and some delivery platforms may provide advantages over others. An important next step toward more widespread dissemination of such interventions is better understanding how PCPs use multimedia resources under naturalistic conditions and what factors affect parental engagement in such materials.
To learn more about the use of multimedia-based delivery of evidence-based information for disruptive behavior problems of early childhood, we conducted a utilization and acceptance study of a novel video-based intervention in a private pediatric primary care setting. The goal was to investigate acceptance and utilization of the intervention by parents and providers with minimal direction from researchers in order to identify factors affecting dissemination.
Methods
Setting and Design
The setting was a large, private, patient-centered medical home located in an urban community in the Pacific Northwest. The practice consisted of 15 pediatricians, 2 certified physician assistants, 1 pediatric nurse practitioner, and other support staff. The clinic used the Ages and Stages Questionnaire, Third Edition 17 for developmental screening and Bright Futures, Third Edition 18 well-child materials. Approximately 7 PCPs staffed the clinic on any given day. A clinical psychologist (S.M.) served as an integrated behavioral health consultant 3 days per week. Data were collected via survey of patients’ parents and medical staff members. Surveys were conducted over a 4-month period beginning in September 2014. All procedures were approved by the Human Subjects Institutional Review Board at Oregon Health & Science University.
Participants
Parents were eligible if they spoke English and attended a well-child visit with a child between the ages of 18 months and 5 years. Eligibility was determined by a research assistant by reviewing daily clinic schedules. Medical providers were eligible participants if they conducted well-child visits at the study site during the data collection period.
Video Package Intervention
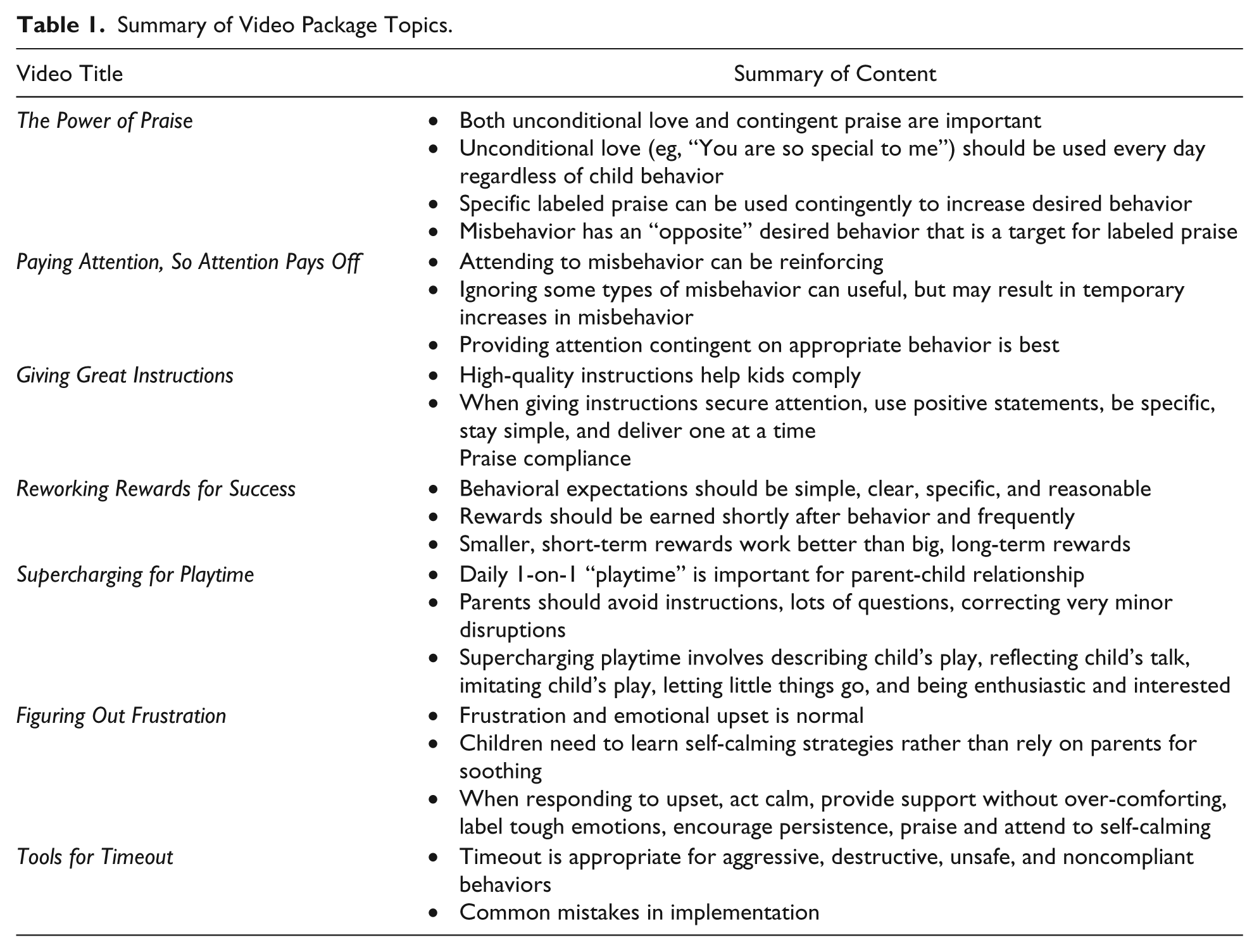
A series of 7 video tutorials was created for the purposes of the study. Videos were approximately 4 to 5 minutes in duration and featured adult and child actors, narration, graphics, and text. Each consisted of a rationale, examples of common mistakes/suboptimal skills, and examples of effective strategy implementation. Whereas the work of Scholer et al12-15,19,20 has focused on multimedia intervention for aggression, this package targeted parenting strategies that are effective across a spectrum of disruptive behaviors. Topics were derived from common elements of evidence-based psychosocial treatments for children’s disruptive behaviors. 21 Table 1 summarizes the content of the videos. Videos were available on iPads during clinic visits. They were also hosted online through the practice’s website in order to be available for viewing subsequent to clinic visits. Corresponding handouts summarizing strategy components were also made available for use by clinicians and online. Flyers with a brief description of the videos were posted in each exam room. Finally, business cards listing video topics and website information were available for PCPs to distribute to parents in order to recommend viewing at home.
Summary of Video Package Topics.
Medical Staff Participation
Implementation was designed to approximate what would occur in a practice setting with minimal direction from researchers. The first author met with physicians as a group to provide a rationale for the study and briefly describe the video package. No specific claims about the effectiveness of the videos were made, but they were described as containing evidence-based information with likely preventative and first-line intervention benefits. Additionally, a “cheat sheet” outlining examples of patient presentations that would indicate appropriateness of a given video was provided. PCPs were asked to use the videos in whatever manner they deemed useful. They were told that parents would be surveyed about their perceptions of the videos.
Medical assistants were asked to make parents of children in study age group aware of the availability of the videos on rooming them for well-child visits. The consulting psychologist provided reminders, encouragement, and feedback to medical assistants throughout the study duration on an informal basis. Parents were able to watch none, some, or all the videos at their discretion, or the PCP may have recommended watching particular videos.
Data Collection
Initial Parent Surveys
Eligible parents were contacted via telephone within 1 week of their child’s well-child visit to invite participation. All participants were asked about overall satisfaction with their child’s visit, how well concerns or questions were answered, if any behavioral concerns existed, and if the videos were mentioned during the visit. Parents who were not made aware of the videos during their visit were provided a short description and asked if they would have liked to have known about them. For parents who reported being made aware of the videos, additional questions included whether the provider recommended a specific video, whether any of the videos were viewed during the visit, how the videos affected the visit, and how likely they were to access the videos on the practice website. Those who reported viewing at least one video were asked about the helpfulness of the information, and likeliness of using recommended strategies. All responses were either “yes/no” or on a 5-point Likert-type scale.
One-Month Follow-up Parent Surveys
Parents who indicated awareness of the videos package during the initial survey were asked for permission to contact them in 1 month for a follow-up survey. The follow-up survey assessed engagement with and perception of the videos. Those who never watched any videos were asked the main reason for not watching and whether they planned to watch in the future. Parents who endorsed watching a video were asked which videos they remembered viewing, if they tried out the recommended strategies, and if they would like to see more videos available in the future. Those who did not try the recommended strategies were asked reasons why and whether they would in the future. Parents who did try recommended strategies were asked how helpful they had been, whether they had observed any positive child behavior changes, and whether they would continue to use the strategies. All responses were either “yes/no” or on a 5-point Likert-type scale, except those that asked about parents reasons for not engaging with the resource, which were multiple choice, including a free response option.
Provider Surveys
Provider surveys were conducted once the videos had been available in the clinic for 3 months. Provider surveys were distributed through email containing a link to an online questionnaire. The questionnaire consisted of 5-point scale items assessing the provider’s awareness of the video tool, frequency of recommending the tool, perceived usefulness, perceived effects of time-constraints, and perception of parental reactions to the videos. In addition, 2 open-ended questions asked what the provider liked most about the videos and what would make them a better resource.
Statistical Analysis
Univariate descriptive statistics were calculated to characterize demographic information and survey responses. Differences between categorical groups were examined via χ2 test for independence for dichotomous dependent variables and the Mann-Whitney U test for ordinal dependent variables. Spearman’s ρ was calculated to test for significant correlations between ordinal variables. All analyses were carried out using IBM SPSS Statistics version 22. 22
Results
A total of 248 parents were successfully contacted via phone, of which 240 (97%) agreed to complete the survey. Median age of the children was 37 months (interquartile range: 24, 52). One hundred and twenty-four (52%) were girls.
Parent-Reported Exposure to Intervention
Table 2 summarizes parents’ responses to the initial survey. Parents were highly satisfied with the well-child visit and felt concerns and questions were well addressed. Concerns about child behaviors or emotions were endorsed by 51 (21%) parents, and while the mean rating of how well concerns were met for this group was high (M = 4.76; SD = 0.51), it was significantly lower than that of parents without behavioral concerns, U(238) = 4257.0, P = .02. Of the 240 parents surveyed, 79 (33%) recalled being informed about the multimedia intervention during the well-child visit; in only 14 instances (6%) did a provider reportedly recommend a specific video. Parents with concerns about their child’s behavior were no more likely to be aware of the videos, χ2(1, N = 240) = 0.166, P = .684. Of those who were not made aware of the videos, 60.9% stated they would have liked to have been informed about them. Parents who had behavioral concerns were significantly more likely to report a desire to have been informed about the resource, χ2(1, N = 161) = 12.713, P < .001. Among parents who were aware of the videos, 52% had watched at least one. Parents with behavioral concerns were significantly more likely to have watched χ2(1, N = 79) = 6.254, P = .012. Among 39 parents who recalled watching a specific video, the percentage who reported watching the timeout topic was highest (51%) followed by emotional frustration (36%), rewards (18%), praise (13%), strategic attending (13%), enhanced play (13%), and effective instruction delivery (5%).
Parent and Provider Ratings of Well-Child Visits and Video Package a .
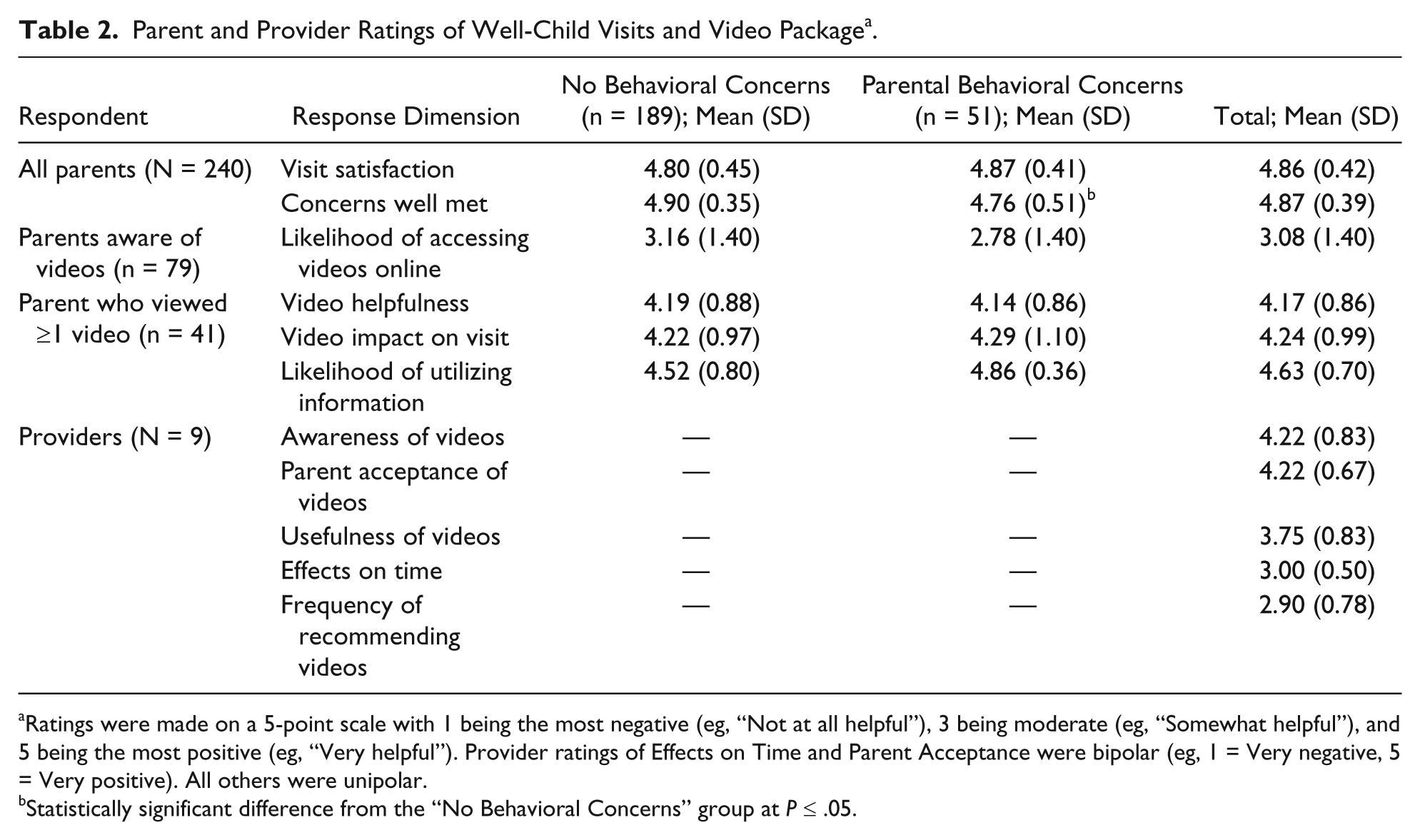
Ratings were made on a 5-point scale with 1 being the most negative (eg, “Not at all helpful”), 3 being moderate (eg, “Somewhat helpful”), and 5 being the most positive (eg, “Very helpful”). Provider ratings of Effects on Time and Parent Acceptance were bipolar (eg, 1 = Very negative, 5 = Very positive). All others were unipolar.
Statistically significant difference from the “No Behavioral Concerns” group at P ≤ .05.
Initial Parent Perceptions and Expected Utilization of Videos
Ratings regarding various aspects of the videos were made on a 5-point scale with 1 being the most negative (eg, “Not at all helpful”) and 5 being the most positive (eg, “Very helpful”). A mean helpfulness rating of 4.14 (SD = 0.86) was reported by parents who watched at least 1 video. Parents similarly rated the videos as having a positive impact on the office visit (M = 4.24, SD = 0.99) and rated themselves as likely to use the information provided (M = 4.63, SD = 0.70). Likelihood of using the information was significantly and positively correlated with perceived helpfulness, rs(39) = .377, P = .015. Overall, parents rated their likelihood of seeking out the videos on the practices website relatively modestly (M = 3.08, SD = 1.42). Parent predicted likelihood of accessing the videos online did not differ based on the presence of parental concerns about child behavior, U(77) = 464.0, P = .31, or having viewed one of the videos, U(77) = 754.0, P = .80; nor was it significantly correlated with perceived helpfulness of the video information, rs(39) = .275, P = .08, or likelihood of using the information provided, rs(39) = −.06, P = .71.
Parent Follow-up Survey
Thirty of 79 (38%) eligible parents eventually completed the follow-up survey via telephone. One month since their child’s visit, 17 of 30 (57%) had ever viewed at least 1 video, but only 3 (10%) had done so via the Internet subsequent to the initial survey. Parents who had never watched the videos cited not having enough time (n = 8), not needing/wanting the advice (n = 3), and forgetting (n = 2) as reasons for not viewing the videos. Eleven of 14 (79%) parents who had not yet watched any videos indicated they would like to in the future, and 16 of 17 (94%) who watched at least 1 video endorsed wanting more resources like the videos at their PCP’s office.
Among those who had viewed a video by the time of the follow-up survey, 47% had not tried suggested strategies and cited lack of need (n = 3), already doing what was suggested (n = 3), and not having time (n = 2) as the reasons why. The nine (53%) who had attempted the suggestions rated them high in helpfulness (M = 4.44, SD = 0.53) and 100% indicated intention to continue using the recommended techniques. Seven (79%) reported observing positive changes in their child’s behavior.
Provider Surveys
Nine of 17 (53%) eligible medical providers completed the survey. As summarized in Table 2, on average, providers were well aware of the videos, felt parents responded positively, found the videos useful, and reported no effects on time constraints. Despite largely positive attitudes toward videos, providers reported recommending them with only moderate frequency. Reported frequency of recommendation was significantly correlated with perceived usefulness as a clinical tool, rs(7) = .732, P = .025. Provider responses to the open-ended questions, “What do you like most about the videos?” and “What would make the videos a better resource for you?” were examined for qualitative themes. Themes about what providers’ liked most included the videos being well-accepted by parents (n = 4), the brief and concise nature of the videos (n = 3), and utility in occupying parents during wait times (n = 2). With regard to improving the videos as resource, provider responses included better coordination with staff about integrating videos into workflow (n = 3), better provider familiarity with the material (n = 1), and having a wider variety of video topics (n = 1).
Discussion
The results have implications for both practice and research. In accordance to previous findings, the results of this study strengthen the conclusion that a strong majority of parents, particularly those who have concerns about their child’s behavior, will receive multimedia-based behavioral interventions positively. For clinicians, multimedia educational materials provide an effective 19 and resource-efficient tool for enhancing existing behavioral care. It is important to note parents highly value discussing concerns directly with their child’s provider, 20 so multimedia tools should be considered adjunct rather than primary approach.
While potential benefits of multimedia materials are apparent, much is to be determined with regard to how they are best disseminated and implemented. Our findings suggest that mere availability of multimedia resources is insufficient to ensure a significant proportion of parents contact them. Despite reasonable efforts to make PCPs and allied staff aware of the availability and utility of the intervention, as well as positive clinician and parent attitudes toward the interventions, only a third of parents reported being made aware of the video package at time of initial survey; still fewer had engaged in the materials. That parents with behavior concerns were not more likely to contact the videos is illustrative of the discrepancy between clinical need and practice. Linking multimedia tools to systematic behavioral screening may be one method for increasing delivery to those parents most likely to use resources.
When parents viewed the video materials, about half reported using the recommended strategies, and 100% of those who used the strategies reported intention to continue. This suggests that a substantial proportion of parents may derive benefits from such resources if only they can be initially engaged in them. Somewhat surprisingly, online availability of the multimedia materials did not appear to significantly improve parent engagement. As a group, parents indicated only mild likelihood of accessing materials online, and only 10% of those surveyed 1 month later had done so. This finding suggests effective dissemination may necessitate engagement of materials within the context of clinic visits. In one study, parents who were required to watch multimedia materials during well-child visits had equally positive experiences as those who chose to watch voluntarily, 23 so this approach may be viable.
Conversely, practices may have difficulty altering operations such that viewing of materials during visits is feasible and acceptable to providers. Alternatively, manipulation of other aspects of intervention delivery may affect parental engagement. For instance, the manner in which an intervention is presented (eg, specificity of recommendation, endorsement of content) may affect subsequent engagement. While general online availability appeared inconsequential in this study, other technological platforms, such as software that allows providers to push content directly to parents’ email or social media accounts, may provide additional benefits. More research is required to identify methods that are amenable to providers and engaging for parents.
While a small sample, the clinician-reported results provide some clues about factors that may impact utilization. First, beyond being effective and well-received by parents, clinical tools must be time-efficient. Any clinical resource that requires more than a few minutes is unlikely to be adopted in primary care. Second, to maximize impact, multimedia materials should be implemented systematically and must account for clinic-level characteristics such as existing work flow, resource allocation, and staff coordination. Anecdotally, there was substantial variation among PCPs and allied staff with regard to utilization, and while the reasons for this were not systematically studied, issues such as staff turnover and communication between PCPs and allied staff appeared to be prominent factors.
This study possesses some notable limitations. In an effort to maximize external validity by limiting researcher influence, procedures were not exactly controlled and internal validity suffered. Surveyed parents were self-selected and it may be that those who chose to watch the videos were also those most likely to respond positively. Like other studies on multimedia in primary care,12-15,19,20 this study relied on subjective parental report. It is safe to conclude that a majority of parents perceive multimedia interventions as beneficial, but it remains to be seen whether such interventions reliably alter parent (and ultimately child) behavior in the way intended. Use of psychometrically sound measures of change or direct observation procedures would significantly enhance the existing literature. As there was no control comparison in this study, it is difficult to say what, if any, advantages the multimedia had over usual care. While just 17% of those surveyed actually watched one of the videos, this may in fact be a significant improvement over treatment as usual. Randomized pragmatic trial methodologies 24 may be ideal for future study in balancing experimental control with external validity.
In sum, this study replicates previous findings that multimedia interventions are well accepted by parents, provides initial evidence that providers are also amenable to using these resources, and highlights the need for continued study of dissemination and implementation processes.
Author Contributions
ARR procured and managed grant funding; conceptualized, designed, and provided primary oversight for implementation of the study; oversaw acquisition of data and was responsible for analysis and interpretation; and drafted the initial manuscript. KAF contributed to procuring grant funding, study conceptualization and design, data interpretation, and manuscript revision. SM contributed to procuring grant funding, study conceptualization, implementation, and data acquisition. All authors reviewed and revised the manuscript and approved the final version.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the Cambia Health Foundation.