
Abstract

Case Report
A 4-year-old boy of Guatemalan descent with no significant medical history developed gradual onset of scrotal edema, eye swelling, and cheeks “looking fatter” over the course of 2 weeks. A urine dipstick at his pediatrician’s office was negative for blood and protein and the pediatrician prescribed antihistamines for treatment of presumed allergic symptoms. His symptoms progressed over the next few days with worsening scrotal and body wall edema and intermittent diarrhea prompting a visit to the emergency department. In the emergency department, his mother reported an absence of vomiting, rash, arthritis, and fever but described a mild upper respiratory infection a few days before his edema was first noted. He had no allergies and routine immunizations were up-to-date. Family history was notable for paternal grandparents with end-stage kidney disease of unknown etiology. Physical examination revealed an afebrile child with a blood pressure of 110/73 mm Hg and diffuse anasarca. Workup showed 4+ proteinuria on dipstick and <1 g/dL serum albumin. Renal ultrasound described mild bilateral nephromegaly but was otherwise unremarkable. He was discharged on ranitidine and 2 mg/kg/d of oral prednisolone divided twice a day to treat idiopathic nephrotic syndrome of childhood with nephrology follow-up arranged as an outpatient.
Five days later, he re-presented to the emergency department with a 12-hour history of diffuse, progressively worsening abdominal pain. At his pediatric nephrology visit several days before, his mother described complete adherence to the steroids and ranitidine. In the emergency department, he had a normal appetite, no nausea or vomiting, but did continue to have diarrhea. Vital signs were as follows: temperature 38.1°C, pulse 145 beats/min, respirations 30 breaths/min, blood pressure 117/69 mm Hg, and weight 14.9 kg. Physical examination revealed a mildly distended, diffusely tender abdomen with increased tenderness to palpation in the right lower quadrant. Rebound tenderness was present. Generalized pitting edema was present from the feet to the trunk.
Laboratory workup was notable for a white blood cell count of 24.5 × 103/mm3 with 74% neutrophils, 21% lymphocytes, hemoglobin of 12.2g/dL, and platelet count 488 × 103/mm3. C-reactive protein was markedly elevated at 15.4 mg/dL. Serum albumin was 1.6 g/dL, blood urea nitrogen was 10 mg/dL and creatinine was 0.5 mg/dL; his electrolytes were within normal limits. Spot urinalysis showed 3+ protein but was otherwise unremarkable. Urine albumin to creatinine ratio was 11.8 mg/mg. He received intravenous ceftriaxone due to concern for spontaneous bacterial peritonitis and was transferred to our hospital for consultation with both pediatric surgery and nephrology. On arrival, an abdominal ultrasound revealed clear ileo-ileal intussusception with the sonographer noting maximal tenderness over the site of the lesion (Figure 1). An attending pediatric radiologist was called to perform an air enema. A repeat ultrasound done 3 hours from the initial study did not visualize the intussusception. The air enema procedure was thus aborted and he was admitted to the hospital for observation and serial examinations.
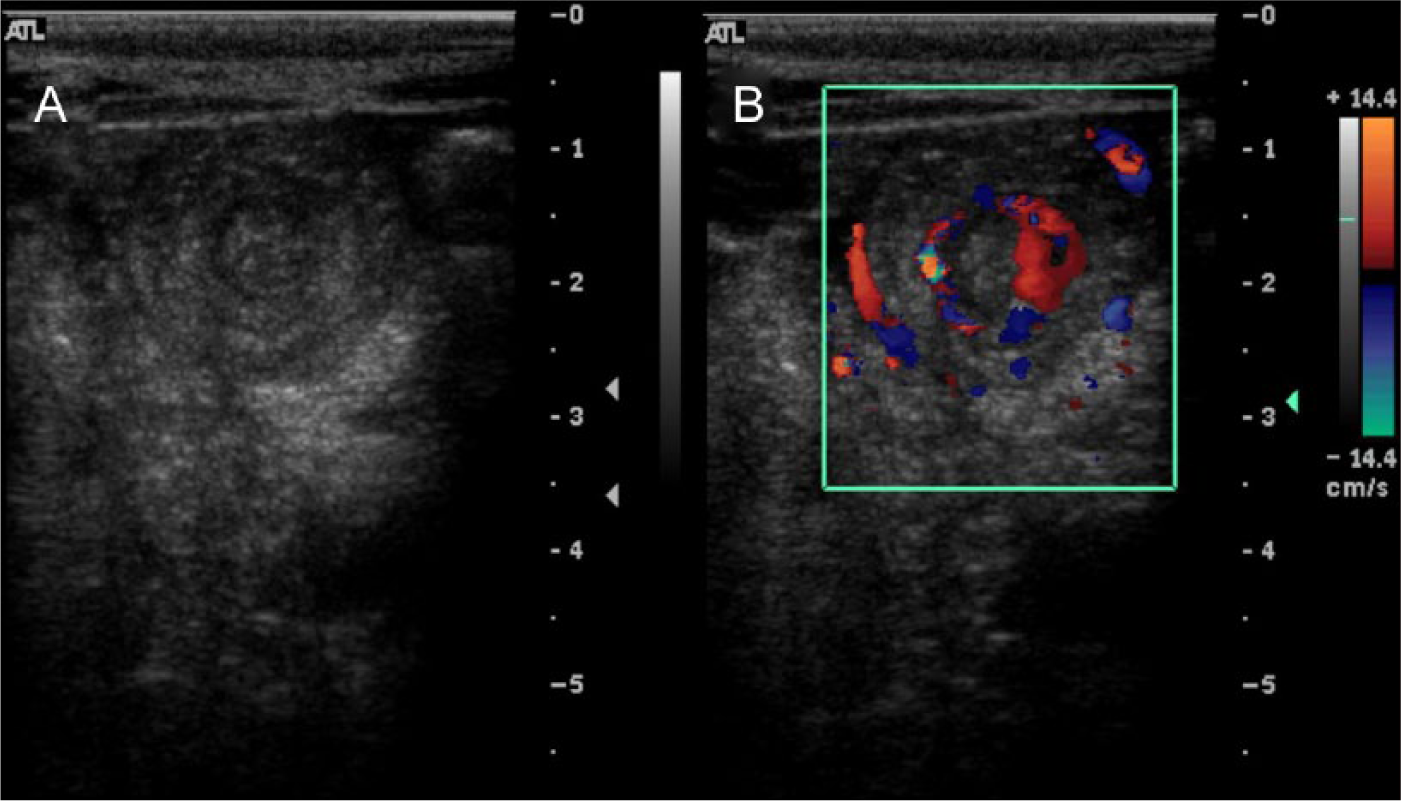
Ultrasound images demonstrating small bowel intussusception. (A) A small bowel intussusception showing a “target” sign. Free fluid is also visible in the image. (B) Color Doppler of the same area demonstrating blood flow.
Final Diagnosis
Intussusception.
Hospital Course
Following admission, he was continued on intravenous fluids, intravenous ranitidine, and intravenous methylprednisolone at 2 mg/kg/d. Antimicrobials were not continued. Serial abdominal examinations performed over the next 24 hours revealed decreasing tenderness. A follow-up ultrasound likewise showed no evidence of intussusception. Repeat laboratory studies showed a resolving lymphocytosis and improved C-reactive protein of 3.9 mg/dL. Blood and urine cultures were negative. He was pain-free at discharge on hospital day 2 and was prescribed a steroid taper. Over the next 1.5 years of follow-up, he developed 2 relapses of nephrotic syndrome, which were steroid responsive, but he had no recurrence of intussusception.
Discussion
Intussusception is one of the most common abdominal emergencies of infancy and early childhood, and is characterized by bowel wall invaginating into another segment of bowel. In untreated intussusception, the vascular supply of the affected segment may be compromised, leading to bowel ischemia which may be fatal. The classic symptomatology of intussusception is intermittent abdominal pain, vomiting, bloody stools (“currant jelly”), and a palpable right upper quadrant mass. The most common type of intussusception is ileocolic. Globally, the majority of pediatric cases occur in patients <1 year of age, with peak incidence occurring between the ages of 4 and 10 months. 1 The rate in North America is between 0.5 and 2.3 cases per 1000 per live births. 1
Intussusception has also been described as a rare but serious complication of nephrotic syndrome and may present atypically. The clinical differences compared to classic, idiopathic intussusception include atypical locations (ie, small bowel), absence of a palpable mass due ascites, older age at presentation, and absence of the classic triad of symptoms. 2 The first confirmed case of intussusception associated with nephrotic syndrome was diagnosed at autopsy in 1975, and subsequently a few case reports have been described in the literature. 3
The pathophysiologic mechanism for the development of intussusception is proposed to be 2-fold. Local inhomogeneity and/or mechanical linkage between 2 nonadjacent segments of bowel wall can predispose the bowel to initial kink formation via a “pivot and torque” mechanism, which can subsequently form an intussusception. 4 A variety of anatomic variants and pathologic lesions have been described as lead points. Common lesions implicated include tumors/polyps (particularly lymphoma), Meckel diverticulum, hematoma, vascular abnormalities, lymphoid hyperplasia, duplication cysts, and celiac disease. Pathologic lead points are identified only about 5% of the time in infants younger than 1 year, but the likelihood of detecting a lead point increases with age. 5
In nephrotic syndrome, which is characterized by generalized edema, patchy bowel wall edema may create a local milieu where the bowel is predisposed to intussusception via disturbance of coordinated peristaltic contraction.2,6 -8 The precise mechanism for the development of intussusception in nephrotic syndrome is incompletely elucidated, but may involve a combination of generalized bowel wall edema as well as local factors such as intramural lymphoid hyperplasia in the presence of ascites or infection. In a review of published cases of intussusception associated with nephrotic syndrome, Asai et al 2 noted that intussusception occurred most commonly when generalized edema had been present for 2 or more weeks. This was the case in our patient, who developed acute abdominal pain after approximately 3 weeks of edema.
Ultrasound is the preferred imaging modality to diagnose intussusception. The advantages of ultrasonography include high accuracy, the ability to detect lead points, absence of radiation, and the ability to monitor therapeutic reduction attempts in real time. 9 Computed tomography and magnetic resonance imaging are options when ultrasound is inconclusive, or in complex clinical situations where additional imaging may be informative such as when there is suspicion for lymphoma.
Treatment principles of intussusception generally emphasize attempting pneumatic or hydrostatic reduction, with surgery being reserved for unsuccessful nonoperative attempts. 9 There is a high success rate of radiologic reduction of idiopathic intussusception. Spontaneous resolution of intussusception is also well described, and occurs more commonly when the lesion is small (<2 cm), limited to the small bowel, and located in the central or left abdomen. 5 In contrast, the described cases of nephrotic syndrome–associated intussusception frequently have required surgical intervention for definitive treatment and have not reduced spontaneously. 2 Rare exceptions in the literature include 2 instances of successful air enema reduction and 1 report of medical management with albumin and furosemide with subsequent resolution.7,10 Possible reasons for this finding may be the occurrence of intussusception at atypical sites or a stiffer bowel wall in the setting of generalized edema, which may not be amenable to reduction with the pressures generated by an air or liquid enema.
To our knowledge, this patient is the first reported case of spontaneous resolution of intussusception in the setting of nephrotic syndrome. His initial clinical presentation of acute abdomen with elevated inflammatory markers required consideration of other life threatening conditions on the differential diagnosis, including acute appendicitis and spontaneous bacterial peritonitis. Other more common etiologies to consider when evaluating a child with abdominal pain and nephrotic syndrome include ascites resulting from rapid fluid accumulation, acute gastroenteritis, urinary tract infection, umbilical or inguinal hernias, referred pain from pneumonia, and thromboembolus related to the hypercoagulable state common in nephrotic syndrome. Ultrasonography proved extremely useful in this case. Not only did it allow for prompt identification of the lesion, but the radiographic resolution of the intussusception correlating with improvement in symptomatology, solidified the diagnosis, avoiding the need for additional diagnostic procedures.
Conclusion
While there are several more common causes of abdominal pain in children with nephrotic syndrome, the differential diagnosis of acute abdomen in this patient population should include intussusception. Intussusception among children with nephrotic syndrome may present atypically in terms of location and symptomatology. A high degree of suspicion for this diagnosis should be kept in mind when initially evaluating these patients. Finally, nephrotic syndrome–associated intussusception may resolve spontaneously and observation may be appropriate in certain clinical settings.
Author Contributions
GSK wrote the initial draft of this manuscript. TMB assisted with editing and supervised the project.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.