
Abstract
Prior studies have found that close mother-child sleep proximity helps increase rates of breastfeeding, and breastfeeding itself is linked to better maternal and infant health. In this study, we examine whether breastfeeding and infant bed-sharing are related to daily rhythms of the stress-responsive hormone cortisol. We found that bed-sharing was related to flatter diurnal cortisol slopes, and there was a marginal effect for breastfeeding to predict steeper cortisol slopes. Furthermore, mothers who breastfeed but do not bed-share had the steepest diurnal cortisol slopes, whereas mothers who bed-shared and did not breastfeed had the flattest slopes (P < .05). These results were significant after controlling for subjective sleep quality, perceived stress, depression, socioeconomic status, race, and maternal age. Findings from this study indicate that infant parenting choices recommended for infants (breastfeeding and separate sleep surfaces for babies) may also be associated with more optimal stress hormone profiles for mothers.
Prior literature shows extensive benefits of breastfeeding for mothers and infants. Breastfeeding infants experience incrementally larger health benefits with increasing exclusivity and duration, including lower risks of respiratory tract infections, gastroenteritis, and asthma. 1 Maternal health benefits of breastfeeding include reduced depression, diabetes, cardiovascular disease, and cancer. Yet only 75% of American mothers initially breastfeed, with rates reduced to 43.8% at 6 months postpartum. 1 Although breastfeeding benefits are clear, how best to promote the breastfeeding relationship while maintaining postpartum maternal health in pragmatic terms is not clear cut. In particular, breastfeeding rates are often linked to increased sleep proximity between mother and infants.2,3 Approximately 11% of American mothers report bed-sharing. 4 Whereas breastfeeding reduces rates of SIDS, 1 mother and child sharing a bed are linked to increased rates of SIDS. 5 In this study, we examine how breastfeeding (a known stress reducer 6 ) and bed-sharing are associated with cortisol, a major physiological stress-responsive hormone, in mothers at 6 months postpartum. Findings from this study can address whether certain feeding and sleep-related parenting choices considered best for babies are also associated with more optimal maternal stress hormone profiles.
Breastfeeding and Cosleeping
Postpartum health status varies as a function of lactation; breastfeeding confers certain protective effects in human mothers. Maternal stress is reduced for breastfeeding mothers,7,8 and breastfeeding also improves maternal sleep.9,10 In sum, breastfeeding is considered beneficial to maternal health11,12 and adjustment, in addition to the known health benefits for babies.12,13
Cosleeping with infants (either in the same bed or same room as the baby) has been proposed as a mechanism to improve rates of breastfeeding 14 and breastfeeding duration 15 and to encourage more optimal infant sleep patterns. 16 One form of cosleeping, mother-infant bed sharing, is associated with reduced length of maternal nighttime awakenings 17 and increased sleep for breastfeeding mothers. 18 Despite these maternal benefits, bed-sharing is also associated with infant deaths because of overlying and entrapment. 19 Because of insufficient evidence that this practice can be ensured safe, the American Academy of Pediatrics recommends against baby bed-sharing. 5 Given the controversial nature of infant bed-sharing practices, combined with evidence that they may be beneficial for new mothers’ sleep and breastfeeding duration, 20 this study can help address whether bed-sharing may be beneficial for maternal stress physiology. In particular, we examine what the combination of breastfeeding and bed-sharing means for cortisol diurnal rhythms.
Normative Cortisol Basal Rhythms and Changes Over the Transition to Parenthood
Cortisol, a stress-sensitive hormone that is the main end product of the hypothalamic-pituitary-adrenal (HPA) axis, varies significantly across 24 hours, with peak levels approximately 30 minutes after waking and a gradual decline across the day, reaching a nadir shortly after bedtime and slowly rising through the night.21,22 Diurnal/basal HPA axis functioning is often measured by the rate of cortisol decline across the waking day (diurnal cortisol slope), which is affected by stress exposure 23 and is associated with a wide range of health outcomes. 24 Reduced rates of decline in cortisol across the day (flatter cortisol slopes) have been found in individuals with difficulty in interpersonal relationships and work and home demands 25 and predicts poor health outcomes, including cardiovascular risk and reduced cancer survivorship.26-32 HPA axis functioning is also associated with regulation of interconnected physiological systems, including immune, metabolic, and cardiovascular processes. 33 Furthermore, the functioning of this axis is responsive to social contexts, including positive social relationships, which are beneficial for health and stress regulation. 34
Becoming a mother provides both an exciting and exhausting new social relationship (between a parent and a child), as well as a host of necessary biological adjustments. Cortisol normatively rises over the course of pregnancy and drops precipitously following parturition. By postpartum week 12, the HPA axis activity normalizes to levels seen prior to pregnancy, 35 an attenuation that may be advantageous by reducing cortisol levels in infant milk. 36 Furthermore, breastfeeding mothers experience an attenuated HPA response to stressors.37-39 This altered reactivity may serve to promote the breastfeeding relationship by reducing the perception and impact of stressful exogenous environmental influences as well as redirecting mothers toward an effective and efficient breastfeeding relationship. 7
Prior studies indicate that physiological motherhood-related changes are linked to postpartum adjustments for both the mother (eg, depression) and the mother-infant (eg, responsiveness to infant cues) relationship. 40 In particular, maternal cortisol is associated with a range of maternal behaviors, including recognition of infant odor and intrusiveness.36,41,42 Findings of links between mothering and cortisol are evident,43-45 yet the research has ambiguous direction of effects, suggesting that more research is needed. In this study, we examine how cortisol diurnal rhythms are associated with 2 important parenting choices: infant feeding mode and sleeping arrangement.
Purpose of the Current Study
Our goal is to better understand how parenting contexts, including breastfeeding and infant sleeping arrangements, are associated with maternal postpartum stress physiology. Whereas the physiological and neurological alterations of the immediate postpartum period have been studied in depth,46 -48 links between parenting and hormones in the later postpartum (6-12 months) period are not well known. Furthermore, most prior studies examining stress, physiology, and maternal behavior largely measure time-limited stressors and cortisol reactivity, often within laboratory settings. Our study uses data from a primary study of maternal allostatic load, or the multiple markers of maternal biological stress, of which cortisol diurnal decline comprises one marker. We examine basal cortisol rhythms in a naturalistic setting (participants’ homes); compared with clinical settings, an at-home biological collection better measures real-world parental biology. We also aim to investigate whether changes in cosleeping sleep routine are related to stress physiology. We, therefore, investigate the relationship between breastfeeding, infant bed-sharing, sleep routines, and the diurnal decline (slope) of cortisol for mothers at 6 months postpartum. We expect to find that breastfeeding is associated with cortisol profiles that are considered to be more ideal for health outcomes (steeper slope), whereas bed-sharing will be most beneficial for breastfeeding mothers, so that mothers who both bed-share and breastfeed will have the steepest slopes.
Methods
Data for these secondary analyses came from the Lake County, Illinois site of the Eunice Kennedy Shriver National Institute of Child Health and Human Development Child Community Health Network. Biological mothers were recruited at the birth of a child (first, second, or third) and followed at multiple time points postpartum. Mothers were between 18 and 40 years of age; had reported ethnic background of African-American/black, white/Caucasian, or Latina/Hispanic; and were able to participate in the primary study in a community setting. The study met all requirements for human subject protection as determined by the institutional review boards, including consent for salivary sampling and processing. The main focus of the primary study was to examine maternal biological stress during the transition to parenthood and subsequent pregnancies. As such, we were able to conduct secondary data analysis of these data with aims not initially intended as part of the primary study. For this secondary study, after excluding mothers for reasons of pregnancy, corticosteroid medication use, shift working, or missing wakeup or bedtime cortisol values, the total analytical sample size was 193 mothers (sample size before exclusions = 251).
Measures
Salivary Cortisol
During the 6-month postpartum interview, participants were given saliva sampling kits and asked to self-collect saliva the day after their interview. The kit included a morning and bedtime diary, vials, labels and straws for “passive drool” collection of saliva samples, and an instruction sheet. Participants self-collected saliva at wakeup, 30 minutes after waking, and at bedtime by expelling saliva through straws into sterile 2-mL cryogenic vials. They wrote down exact dates and times of samples on small labels, which they affixed to the vials. All completed samples and diaries were then sent via US postal service mail to the NorthShore Research Institute, where they were immediately logged in and frozen at −80°C. 49 They were then shipped to ZRT Laboratories in Beaverton, Oregon. Cortisol was reported in nanograms per milliliter but converted to micrograms per deciliter for data analysis. In original units, the reportable range was 0.3 to 140, with a limit of detection of 0.3. Interassay coefficients of variation were 7% (11.8) for high-range, 20% (3.0) for midrange, and 14% (0.3) for low-range cortisol samples.
Diurnal decline (slope) was calculated using the following formula for each participant: (Bedtime cortisol − Wakeup cortisol)/(Bedtime − Waketime).
Breastfeeding and Bed-Sharing
During the 6-month in-person interview, mothers were asked, “Are you breastfeeding now?” Those who answered affirmatively became part of the currently breastfeeding group. Of the 193 mothers who comprise the current sample, 55 mothers (27.9%) were still breastfeeding at 6 months postpartum.
To measure bed-sharing, the cortisol bedtime diary included a question about sleeping habits the night before collection: “Did any of the following share a bed with you last night for all or part of the night?” Mothers reporting sharing a bed with infants were considered to be bed-sharers. During the interview, a question, “Where does your baby sleep most of the time?” was considered typical if mothers answered “Adult bed or mattress” as a response. Of the 193 mothers, 71 (36.8%) shared a bed with their baby on the night before salivary collection, whereas only 43 (22.3%) typically shared a bed. In the major analysis, we considered bed-sharers as those who reported doing so in the salivary diary; however, Table 1 combines this information by investigating whether routine bed-sharers (reported on saliva diary and during interview) differed from nonroutine bed-sharers (reported on either the saliva diary or during interview but not both) and non–bed-sharers (no report of any bed-sharing). No information was collected comparing bed-sharing with room-sharing mothers.
Sample Descriptives and ANOVA Testing for Breastfeeding and Bed-Sharing Groups (n = 193). a
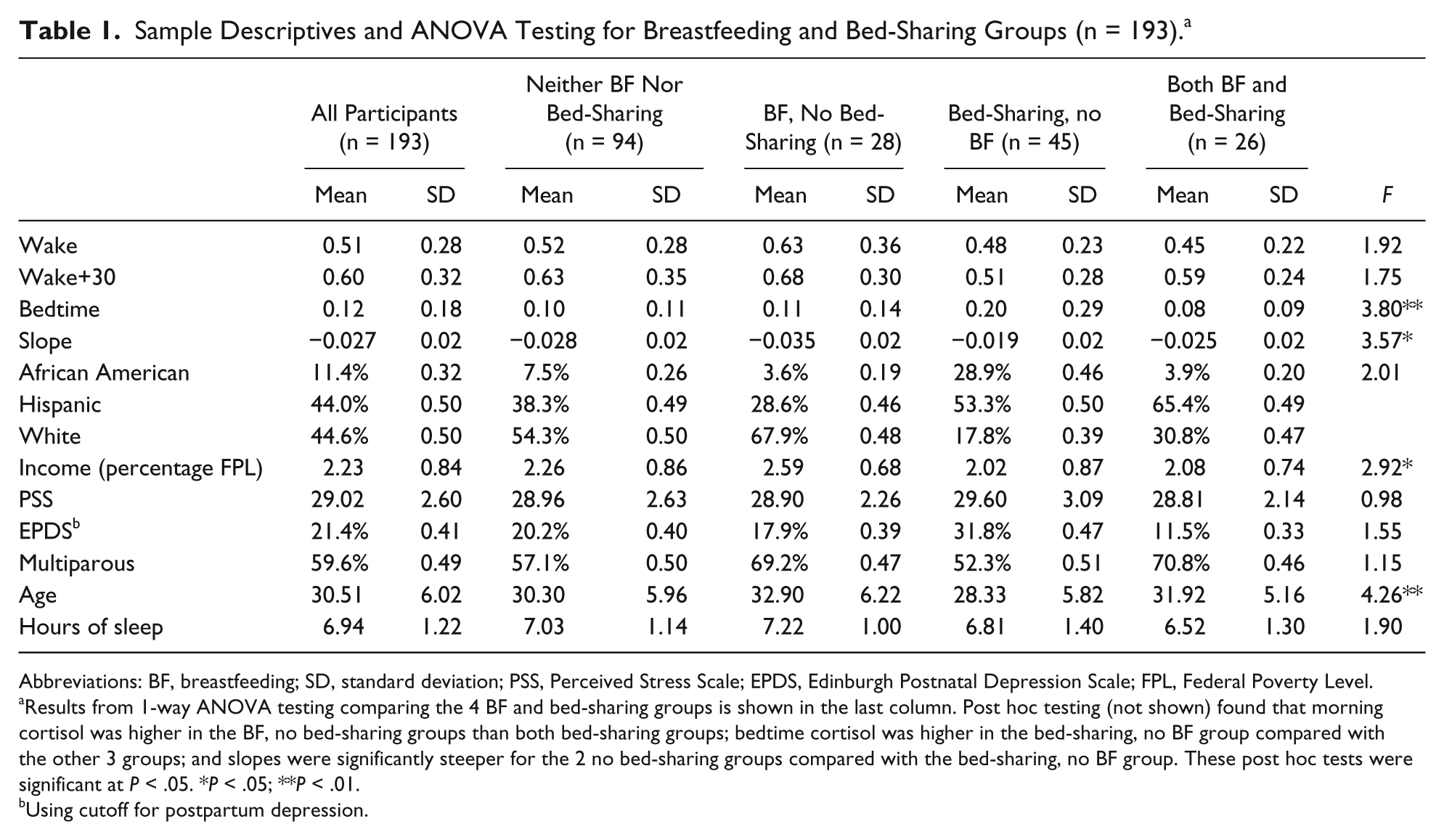
Abbreviations: BF, breastfeeding; SD, standard deviation; PSS, Perceived Stress Scale; EPDS, Edinburgh Postnatal Depression Scale; FPL, Federal Poverty Level.
Results from 1-way ANOVA testing comparing the 4 BF and bed-sharing groups is shown in the last column. Post hoc testing (not shown) found that morning cortisol was higher in the BF, no bed-sharing groups than both bed-sharing groups; bedtime cortisol was higher in the bed-sharing, no BF group compared with the other 3 groups; and slopes were significantly steeper for the 2 no bed-sharing groups compared with the bed-sharing, no BF group. These post hoc tests were significant at P < .05. *P < .05; **P < .01.
Using cutoff for postpartum depression.
To disaggregate the effect of breastfeeding with the effect of a bed-sharing arrangement, 4 mutually exclusive categories were created: breastfeeding, bed-sharing (n = 26; 13.5% of sample); breastfeeding, not bed-sharing (n = 28; 14.5% of sample); not breastfeeding, bed-sharing (n = 45; 23.3% of sample); and not breastfeeding, not bed-sharing (n = 94; 48.7% of sample).
Covariates
In addition to the variables listed above, we examined a number of demographic, health behavior, and psychosocial variables collected either during the in-person interview or as part of the salivary diary. Table 2 shows descriptive statistics for the sample. The participant sample comprised 22 (11.4%) African American, 86 (44.6%) Caucasian, and 85 (44.0%) Hispanic mothers. Other demographic variables included income level (percentage poverty level), age, language use (Spanish, English), and parity. Health behavior variables included smoking, hours of sleep the night prior to salivary collection, and medication use on the day of sampling. Psychosocial variables included the Edinburgh Postnatal Depression Scale (EPDS) 50 and the Perceived Stress Scale (PSS). 51 As part of the larger study, all mothers who met criteria for postpartum depression 50 were contacted by a study social worker and given referrals.
OLS Regression Predicting Cortisol Slope. a
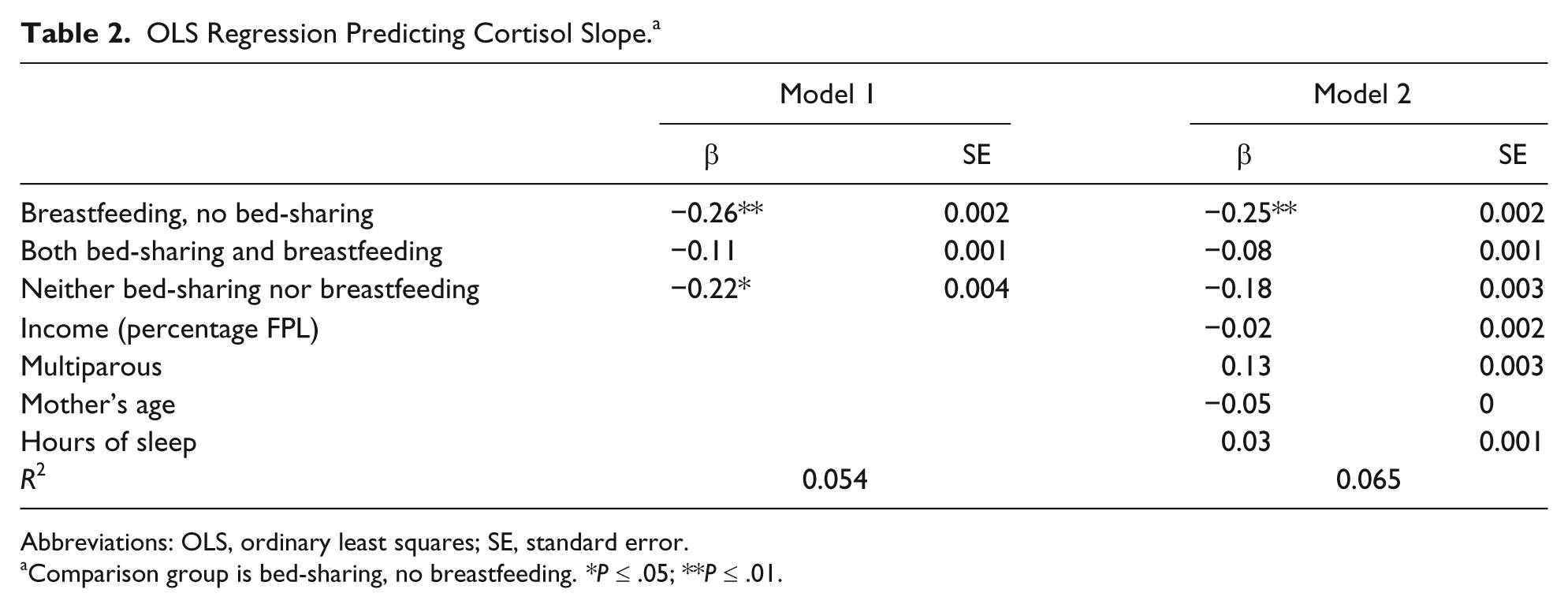
Abbreviations: OLS, ordinary least squares; SE, standard error.
Comparison group is bed-sharing, no breastfeeding. *P ≤ .05; **P ≤ .01.
Our initial testing for these covariates showed that breastfeeding and/or bed-sharing rates differed by race/ethnicity, federal poverty level, parity, age, and hours of sleep but not by EPDS, PSS, medication use, and smoking status. We, therefore, only retained the significant covariates in the current analysis. None of the excluded variables was significantly associated with breastfeeding, bed-sharing, or categories of breastfeeding and bed-sharing in any models. Additionally, when included in models (not shown) with breastfeeding and bed-sharing categories, race/ethnicity was not significantly predictive of cortisol slope; so we did not retain the race/ethnicity variables in the models shown. We, therefore, covaried a number of factors that may have influenced selection into sleeping patterns and breastfeeding and retained all significant variables.
Analytic Plan
Data were analyzed using the statistical software SPSS (version 20). Missing data for morning or evening cortisol were not replaced, and participants with missing morning or evening cortisol data were excluded from analysis. Using a 2-way ANOVA, we examined differences in cortisol slope by breastfeeding and bed-sharing. Then, using ordinary least-squares regression, we examined whether BF/bed-sharing groups of mothers showed differing cortisol diurnal declines, even after addition of sleep, parity, and demographic covariates. Finally, to disaggregate the effects of typical and atypical sleep arrangements, we used 1 and 2-way ANOVAs to examine whether cortisol slopes for nonroutine bed-sharing mothers differed from that of either routine bed-sharing mothers or non–bed-sharing mothers.
Results
Average cortisol levels were 0.51 µg/dL for wakeup, 0.12 µg/dL for bedtime, and −0.027 µg/dL for slope, thereby showing the normative diurnal profile of high cortisol levels on waking, lowest levels at bedtime, and declining levels across the waking day. A 2-way ANOVA with breastfeeding and bed-sharing (not shown) found main effects for bed-sharing [F (1, 192) = 7.184; P < .01] and marginal effects for breastfeeding [F (1, 192) = 3.403; P < .10], with bed-sharing associated with flatter cortisol declines and breastfeeding (marginally) with steeper cortisol declines, but no significant interaction between the two.
Across the groups defined by infant sleeping and feeding choices (Table 1), significant differences were found, using a 1-way ANOVA and Tukey’s honestly significant difference post hoc analyses, for bedtime cortisol and cortisol slope across the day. There were no significant differences in morning cortisol by group. The bed-sharing, non-BF women had higher bedtime cortisol compared with the neither BF nor bed-sharing women (95% confidence interval [CI] for mean difference = 0.013, 0.178; P < .05) and the both BF and bed-sharing women (95% CI for mean difference = 0.005, 0.229; P < .05). Bedtime cortisol was not significantly different between the bed-sharing, non-BF women and the BF, non–bed-sharing women. The bed-sharing non-BF women also had flatter slopes compared with the BF, non–bed-sharing women (95% CI for mean difference = 0.023, 0.027; P < .05) and marginally flatter slopes compared with the neither BF nor bed-sharing women (95% CI for mean difference = −0.0004, 0.018; P < .10). Cortisol slope was not significantly different between the bed-sharing non-BF women and the both bed-sharing and breastfeeding women. These mean differences suggest that it is not breastfeeding or bed-sharing alone but, rather, the combination of these factors that is associated with cortisol diurnal rhythms. The cortisol differences are shown graphically in Figure 1 and numerically in Table 1.
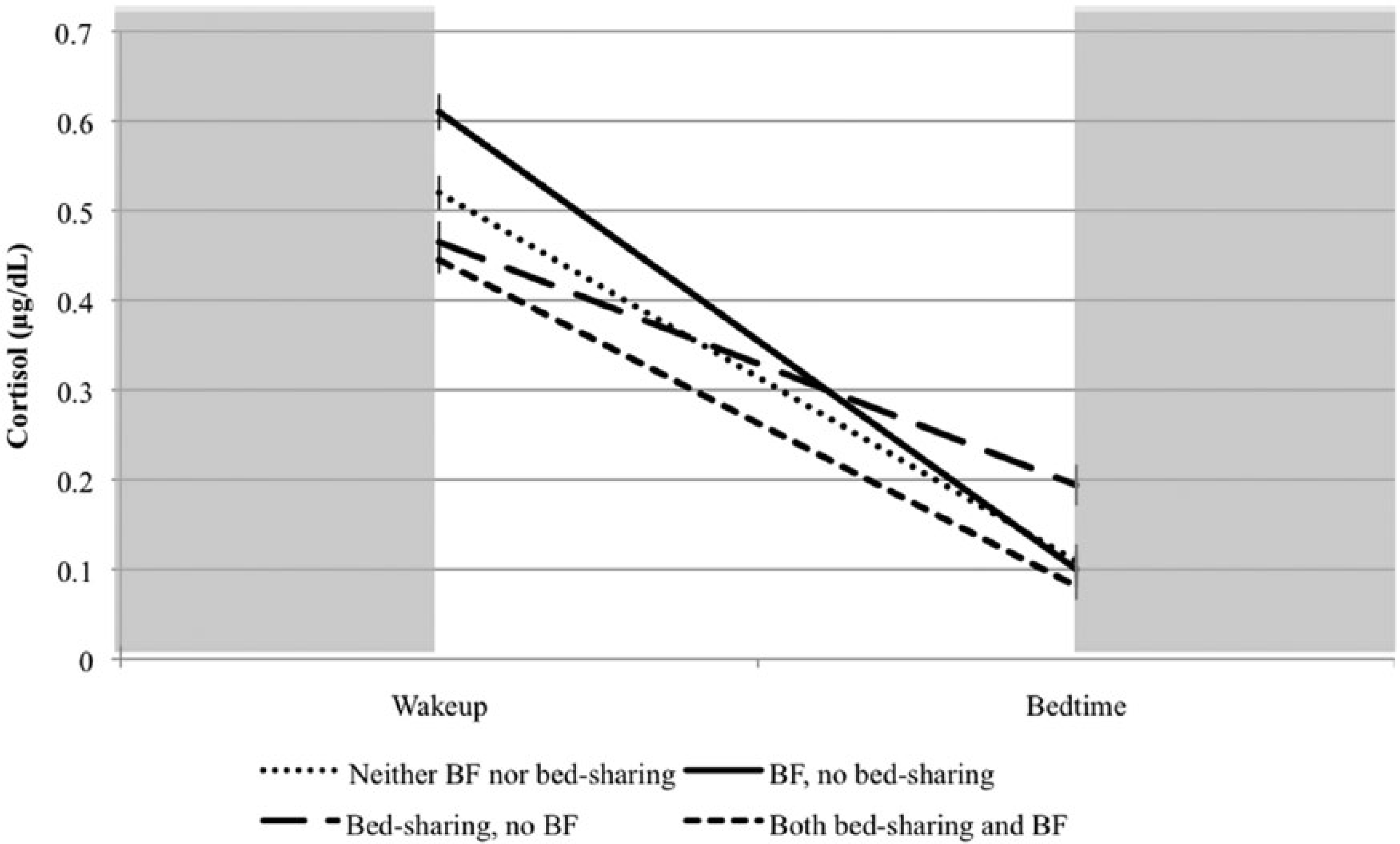
Cortisol change across the day, by breastfeeding (BF) and bed-sharing (shaded area represents sleep).
To examine infant feeding and sleeping choice categories (excluded group: bed-sharing, no BF), net of demographic, subjective sleep quality, and parity variables, we used an ordinary least-squares regression to predict cortisol slope (Table 2). The BF, no-bed-sharing group had steeper slopes than the bed-sharing, no BF group in both the unconditional model (model 1: β = −0.26, P < .01) and the conditional model (model 2: β = −0.25, P < .01), whereas the neither bed-sharing, nor BF group had steeper slopes than the bed-sharing, no BF group in the unconditional model (β = −0.22; P < .05) and marginally in the conditional model (β = −0.18; P < .10). The BF, bed-sharing group did not significantly differ in slope from the bed-sharing, no BF group (P > .05). Furthermore, no covariates predicted cortisol slope (even when race/ethnicity was added to the model; results not shown here).
Finally, we investigated how a change in bed-sharing routine was related to cortisol slopes. Most mothers reported the same infant sleeping arrangements in the diary and at the interview, across all 4 BF and bed-sharing conditions (ranging from 65% to 85.7% similarity). In Table 3, a 1-way ANOVA indicates that cortisol slopes were steeper for mothers who did not report bed-sharing, compared with both nonroutine and routine bed-sharers. Furthermore, a 2-way ANOVA suggests that bed-sharing differences persist even after accounting for breastfeeding.
ANOVA for Bed-Sharing Routine, Breastfeeding (BF), and Cortisol Slopes. a
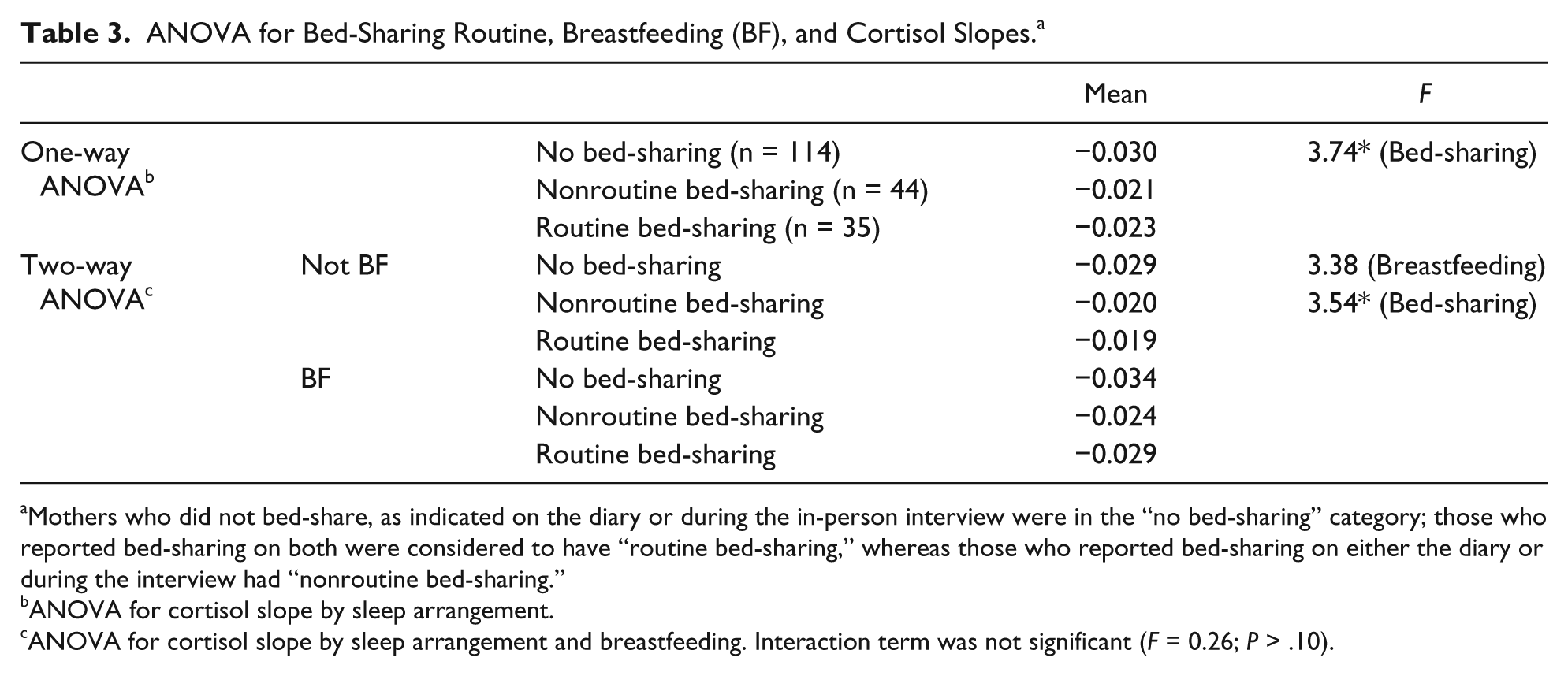
Mothers who did not bed-share, as indicated on the diary or during the in-person interview were in the “no bed-sharing” category; those who reported bed-sharing on both were considered to have “routine bed-sharing,” whereas those who reported bed-sharing on either the diary or during the interview had “nonroutine bed-sharing.”
ANOVA for cortisol slope by sleep arrangement.
ANOVA for cortisol slope by sleep arrangement and breastfeeding. Interaction term was not significant (F = 0.26; P > .10).
Discussion
This exploratory study examined cortisol diurnal rhythms and sleeping arrangements for birth mothers with 6-month-old infants. Our findings suggest that parenting choices considered positive for infant outcomes are associated with more optimal maternal stress hormone profiles. Specifically, cortisol slopes are steeper for women who did not bed-share, particularly when combined with breastfeeding. Whereas prior studies have found links between psychosocial adjustment and parenting behaviors with postpartum diurnal cortisol rhythms,52-54 this study reveals these associations, particularly between parenting behavior and the cortisol rhythm.
Breastfeeding, long considered the best way to nourish infants based on links to better child developmental and health outcomes,55,56 was associated with optimal stress hormone profiles for mothers in this study when combined with separate sleeping surfaces (no bed-sharing), but this benefit was not seen for breastfeeding mothers who bed-share. Prior studies have largely shown breastfeeding benefits for HPA reactivity to stressors.8,37,39 This study points toward benefits of separate sleeping surfaces, an effect that was significant regardless of breastfeeding status, but effects of not bed-sharing are strongest for breastfeeding mothers. Although we could not control for selection factors related to maternal choices to breastfeeding and bed-sharing, our findings remained significant after accounting for likely confounding variables such as poverty level and hours of sleep.
It is not clear what accounts for steeper cortisol slopes among non–bed-sharing mothers; although we control for sleep quantity (hours of sleep), one possibility is that sleep quality is improved in mothers who maintain separate sleeping surfaces from their infants, with improved sleep quality in turn predicting steeper cortisol slopes.
Examining sleeping routine provides further insights on bed-sharing and cortisol. Even when comparing mothers who reported a different sleep arrangement on the night before collection (compared with interview-reported sleep arrangement) with those who reported neither bed-sharing during the interview nor the night before collection, our results show that bed-sharing is associated with flatter slopes. Both groups of bed-sharing mothers had flatter slopes than non–bed-sharing mothers, regardless of whether they experienced a routine change. These findings suggest that bed-sharing may be associated with deleterious physiological stress profiles, although we do not know if these profiles persist long term or are reversible.
Study Limitations
In addition to selection factors that may influence choices to breastfeed or bed-share, infant characteristics such as temperament, sleeping patterns, infant feeding choices, and infant sleeping proximity were not evaluated in this current study; these factors could all affect parental physiology. Furthermore, there are a host of varied cosleeping contexts for families, and evaluation of these environments, including room-sharing (mother and infant share a room, not a bed) will further our understanding of maternal physiology and sleep environments. Breastfeeding was also assessed by asking whether mothers breastfed, not whether they exclusively breastfed or supplemented with formula or through bottle feeding.
This study assessed maternal physiology using a single biomarker, at one point in time using cross-sectional data, so causal directions and more comprehensive physiological profiles were not examined. Further research should aim to elucidate these connections, including the possible causal relationships between parenting contexts and maternal physiology. Furthermore, collection was over the course of a single day, not multiple days, and cortisol has significant intraindividual and interindividual day-to-day variability. Examining how physiological and parenting variables change over time, even over the course of a number of consecutive days, would provide further insights into both causal directions and strength of these associations between biology and social context.
Conclusion
This study provides evidence for links between maternal behavior and maternal physiology. In our study, breastfeeding, in addition to previously known attenuation of stress-induced cortisol reactivity, 37 is associated with steeper cortisol diurnal slopes, but only when combined with separate sleeping surfaces. These physiological alterations of high morning and low evening levels are not present when infants are bed-sharing. Although bed-sharing has been previously linked to increased breastfeeding duration, this study suggests that bed-sharing is associated with significantly flatter (less optimal) cortisol profiles for mothers. Our findings are tentative and require further study with larger and nonregional samples, using other biomarkers, and include assessments relating changes in biology to measures of maternal health. Further research should also examine whether highly controlled, safe cosleeping environments yield more positive physiological alterations. Nonetheless, this exploratory study points toward possible physiological benefits of parenting choices advocated by the American Academy of Pediatrics—extended breastfeeding with separate sleeping surfaces from infants.
Author Contributions
CDS helped supervise salivary data collection, participated in the concept and design of the study, carried out the initial analyses, drafted and revised the manuscript and approved the final manuscript as submitted. EKA helped conceptualize and design the overall study, critically reviewed the manuscript and approved the final manuscript as submitted. MUS helped conceptualize and design the overall study, coordinated data collection, critically reviewed the manuscript and approved the final manuscript as submitted. JBK participated in the concept and design of the study, critically reviewed the manuscript and approved the final manuscript as submitted. COM participated in the concept and design of the study, critically reviewed the manuscript and approved the final manuscript as submitted.
Footnotes
Acknowledgements
This article is designated a Core Paper of the Child Community Health Network (CCHN), because it reflects major ideas and work considered central to our network. Accordingly, the last designated author is the network itself preceded by the names of those on the writing team who directly prepared this article listed in the order the team judged best reflects their relative contributions. Members of each site are listed below. Baltimore, MD: Baltimore City Healthy Start, Johns Hopkins University. Community PI: M. Vance; Academic PI: C. S. Minkovitz; Co-Invs: P. O’Campo, P. Schafer; Project coordinators: N. Sankofa, K. Walton. Lake County, IL: Lake County Health Department and Community Health Center, the North Shore University Health System. Community PI: K. Wagenaar; Academic PI: M. Shalowitz; Co-Invs: E. Adam, G. Duncan*, A. Schoua-Glusberg, C. McKinney, T. McDade, C. Simon; Project Coordinator: E. Clark-Kauffman. Los Angeles, CA: Healthy African American Families, Cedars-Sinai Medical Center, University of California, Los Angeles. Community PI: L. Jones; Academic PI: C. Hobel; Co-PIs: C. Dunkel Schetter, M. C. Lu; Co-I: B. Chung; Project coordinators: F. Jones, D. Serafin, D. Young. North Carolina: East Carolina University, NC Division of Public Health, NC Eastern Baby Love Plus Consortium, University of North Carolina, Chapel Hill. Community PIs: S. Evans, J. Ruffin, R. Woolard; Academic PI: J. Thorp; Co-Is J. DeClerque, C. Dolbier, C. Lorenz; Project coordinators: L. S. Sahadeo, K. Salisbury. Washington, DC: Virginia Tech Carilion Research Institute, Virginia Tech, Washington Hospital Center, Developing Families Center. Community PI: L. Patchen; Academic PI: S. L. Ramey; Academic Co-PI: R. G. Lanzi; Co-Invs: L. V. Klerman, M. Miodovnik, C. T. Ramey, L. Randolph; Project coordinator: N. Timraz; Community coordinator: R. German. Data Coordination and Analysis Center DCAC (Pennsylvania State University). PI: V. M. Chinchilli; Co-Invs: R, Belue, G. Brown Faulkner*, M, Hillemeier, I. Paul, M. L. Shaffer; Project coordinator: G. Snyder; Biostatisticians: E. Lehman, C. Stetter; Data managers: J. Schmidt, K. Cerullo, S. Whisler; Programmers: J. Fisher, J, Boyer, M. Payton. National Institutes of Health. Program scientists: V. J. Evans and T. N. K. Raju, Eunice Kennedy Shriver National Institute of Child Health and Human Development; L. Weglicki, National Institute of Nursing Research; Program Officers; M. Spittel* and M. Willinger, NICHD; Y. Bryan,* NINR. Steering Committee Chairs. M. Phillippe, University of Vermont; E. Fuentes-Afflick,* University of California–San Francisco School of Medicine.
The authors also thank ZRT Laboratory: D. Zava.
*
Indicates those who participated in only the planning phase of the CCHN.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The CCHN is supported through cooperative agreements with the Eunice Kennedy Shriver National Institute of Child Health and Human Development (U HD44207, U HD44219, U HD44226, U HD44245, U HD44253, U HD54791, U HD54019, U HD44226-05S1, U HD44245-06S1, R03 HD59584) and the National Institute for Nursing Research (U NR008929).