
Abstract
Objective. To identify general awareness of booster seats as well as reasons for use and nonuse in an urban pediatric emergency room. Methods. A total of 100 questionnaires were completed consisting of 24 questions each. Questions included knowledge of booster seat guidelines, source of knowledge, awareness of risks, and confidence in booster seats. Afterward, participants were provided an educational handout. Results. Majority of parents reported currently using or having used a booster seat. The most popular reason was to protect from injury (78%), and reason for nonuse was size (44%). Majority of parents agreed that motor vehicle crashes were the leading cause of death in children. However, 56% of parents prematurely transitioned child out of a booster seat. Only 20% reported learning about booster seats from their pediatrician. Conclusion. Parents continue to transition their children prematurely from booster seats. Current state laws need revision as well as further education using simplified illustrated guidelines.
Introduction
According to the National Highway Traffic Safety Administration and the United States Centers for Disease Control and Prevention, car accidents are the leading cause of unintentional death in children 4 to 9 years old. 1 Booster seats have been shown to effectively reduce the risk of morbidity by 45% for children in this age group. 2 However, statistics tell us that once a child graduates from a forward facing car seat, booster seat use drops exponentially in the range of 10% to 45% use nationwide.3,4 In 2000, a study found that booster seat use peaked at age 3 years (29%) and declined drastically with each succeeding year to 1% after age 5 years. 5 According to the National Highway Traffic Safety Administration, booster seat use among 4- to 7-year-olds since 2006-2013 has only increased from 41% to 46%, whereas booster seat use in 2013 among children 8 to 12 years old was only 10%. 3
Children who are prematurely placed in a vehicle’s shoulder-lap belt system are at an increased risk for head injury, spinal cord injury, and intra-abdominal trauma.5-8 Seat belts in vehicles are designed to properly accommodate an average adult with the lap portion of the belt riding low over the hips and held in place by a mature anterior superior iliac spine. The shoulder portion should cross the sternum and shoulder. 2 According to the American Academy of Pediatrics (AAP), the best practice is to have children remain in a booster seat until the lap and shoulder belt appropriately fit, which typically occurs when a child has reached a height of 4 ft 9 in and between the ages of 8 and 12 years. 9 Still, the Louisiana child passenger law only mandates that a child younger than 6 years and weighing 60 lbs or less should be restrained in a child restraint system,10,11 therefore, giving parents a false sense of security regarding the safety of a vehicle’s seat belt system. The wide range of variability in children’s weight and height at any given age can also cause parental confusion. Therefore, using guidelines that emphasize a child’s proper positioning of a vehicle seat belt system may be easier to understand and promote.
So far there have been many strategies to promote, educate, and upgrade the child passenger laws. Although it has improved overall parental awareness in the past 10 years, it has not improved use and adherence to best practice guidelines recommended by the AAP.
In our study, we sought to determine the general use of booster seats in children aged between 4 and less than 10 years and to identify the reasons for continued use and nonuse of booster seats as it relates to general knowledge of car seat guidelines, perceived risk of motor vehicle crashes, environmental factors, and parenting style.
Methods
This study took place in the Pediatric Emergency Department at Children’s Hospital of New Orleans. This was a convenient sample of patients at our teaching hospital. The emergency room treats approximately 55 000 patients each year and admits approximately 7400 patients annually to their inpatient service. The emergency room covers a diverse socioeconomic background in the greater New Orleans area including the entire state of Louisiana. It is a major referral center and the only freestanding children’s hospital in the state of Louisiana.
This cross-sectional study was performed between November 2013 and April 2014. The study design and consent forms were approved by the institutional review boards of both the Louisiana State University Health Sciences Center (LSUHSC) and Children’s Hospital of New Orleans systems. The surveys were pretested in the Children’s Hospital Emergency Department and then edited to the final format. A waiver of documentation of written consent was granted through the institutional review board process. Once in the examining room, we as primary investigators (emergency room attending and pediatric resident) explained that we were conducting an anonymous survey without identifiable markers regarding child safety with the intent to improve education. The survey consisted of 24 questions that were completed by the caregiver/parent in a private examining room on their own. The survey included questions about demographics, use of booster seats, perceived benefit of use, reasons for use, knowledge of car accident risks, and a parenting style assessment. The participants were approached for participation in the study if they were caregivers with children aged between 4 years and less than 10 years. They were excluded from participation if triaged with an emergent (conditions with imminent risk to life or limb) complaint. After completion of the survey, all participants were provided a handout from Boosters Are for Big Kids! an illustrated 5-step test for accurate transition from a booster seat and answers to the general knowledge questions on the survey. Surveys were conducted on various days of the week and at different times throughout the day, including nights and weekends to try and ensure a diverse sampling of the patient population. To not compromise or delay medical care, the survey was given to the caregivers in a private room after their initial assessment and treatment plan was established. All caregivers approached agreed to participating in the survey. Data entry and analysis were completed using Epi Info 7, May 2014.
Results
During the 5-month study period, a total of 100 eligible surveys were completed in the Children’s Hospital emergency department. The participant’s children were between 4 and less than 10 years of age. The caregiver’s ages ranged from 18 to 23 years (8%), 24 to 29 years (31%), 30 to 35 years (36%), 36 to 40 years (14%), and more than 40 years (10%). Of the participants, 45% had some level of college education, 36% had only a high school education, and 15% postgraduate education. The children of those surveyed were 67% African American, 24% Caucasian, 7% Hispanic, and 1% Asian/other. The participants had a household income range of $10 000 to $30 000 (40%), $40 000 to $100 000 (23%), and less than $10 000 (22%). Ninety-six percent (n = 96) of the participants reported that their children see a pediatrician regularly for sick and/or well visits other than seeking care in the emergency room.
Booster seats were reported to have been owned and/or used by 70% of the participant’s children, and 76% of the caregivers were aware that Louisiana had a child passenger safety law. But when asked what age they thought one should keep a child in a booster seat, 56% answered less than 6 years (Figure 1), which is actually consistent with the current Louisiana child passenger law, but not considered best practice according to the AAP. 9 The most common reason given for using a booster seat was to protect child from injury (72%), and the most common reason given for nonuse was that the child was perceived to be “too big” (44%). Only 20% of caregivers learned about booster seats from their pediatrician even though 96% reported having a pediatrician (Figure 2).
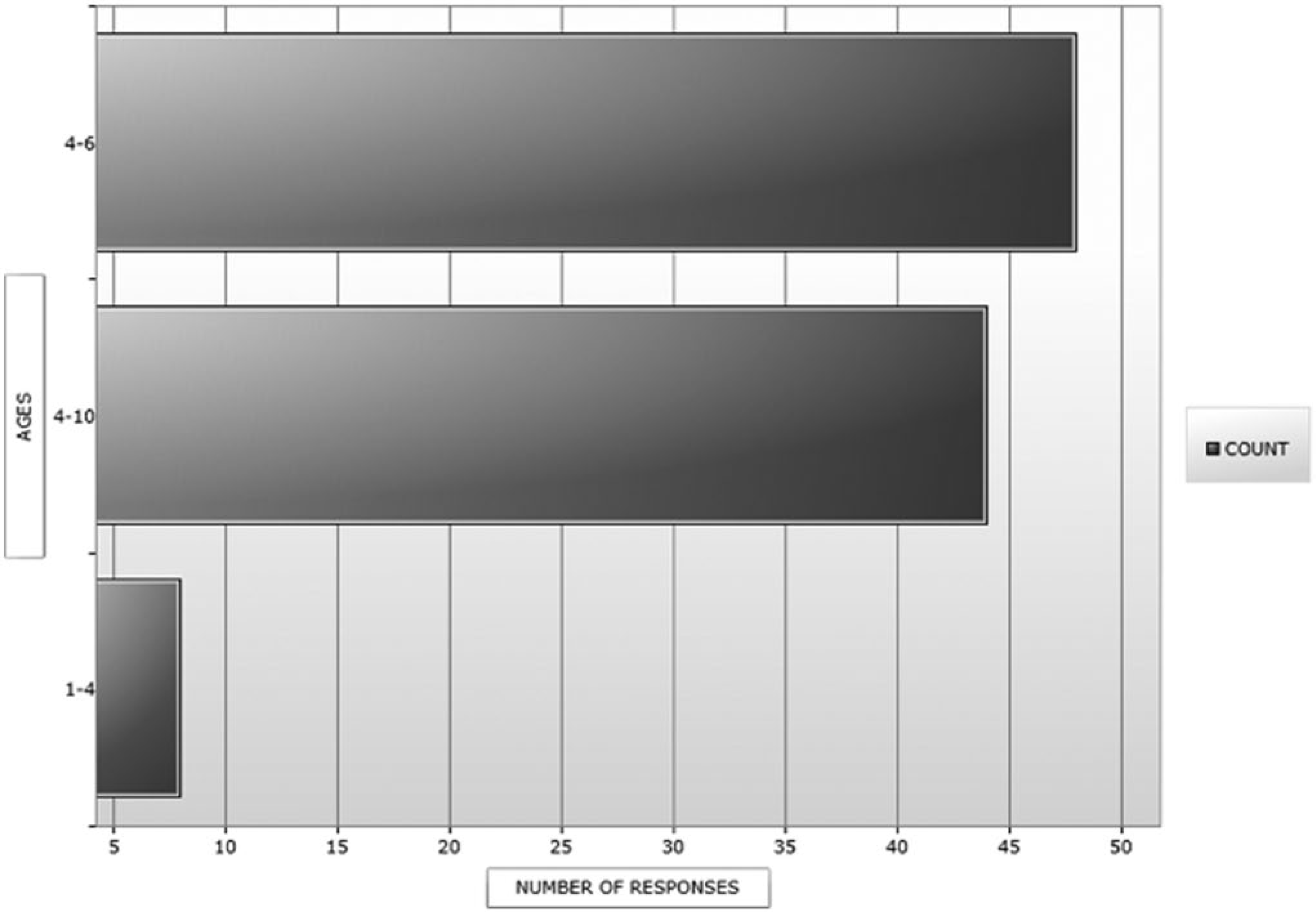
What age do you keep a child in a booster seat?
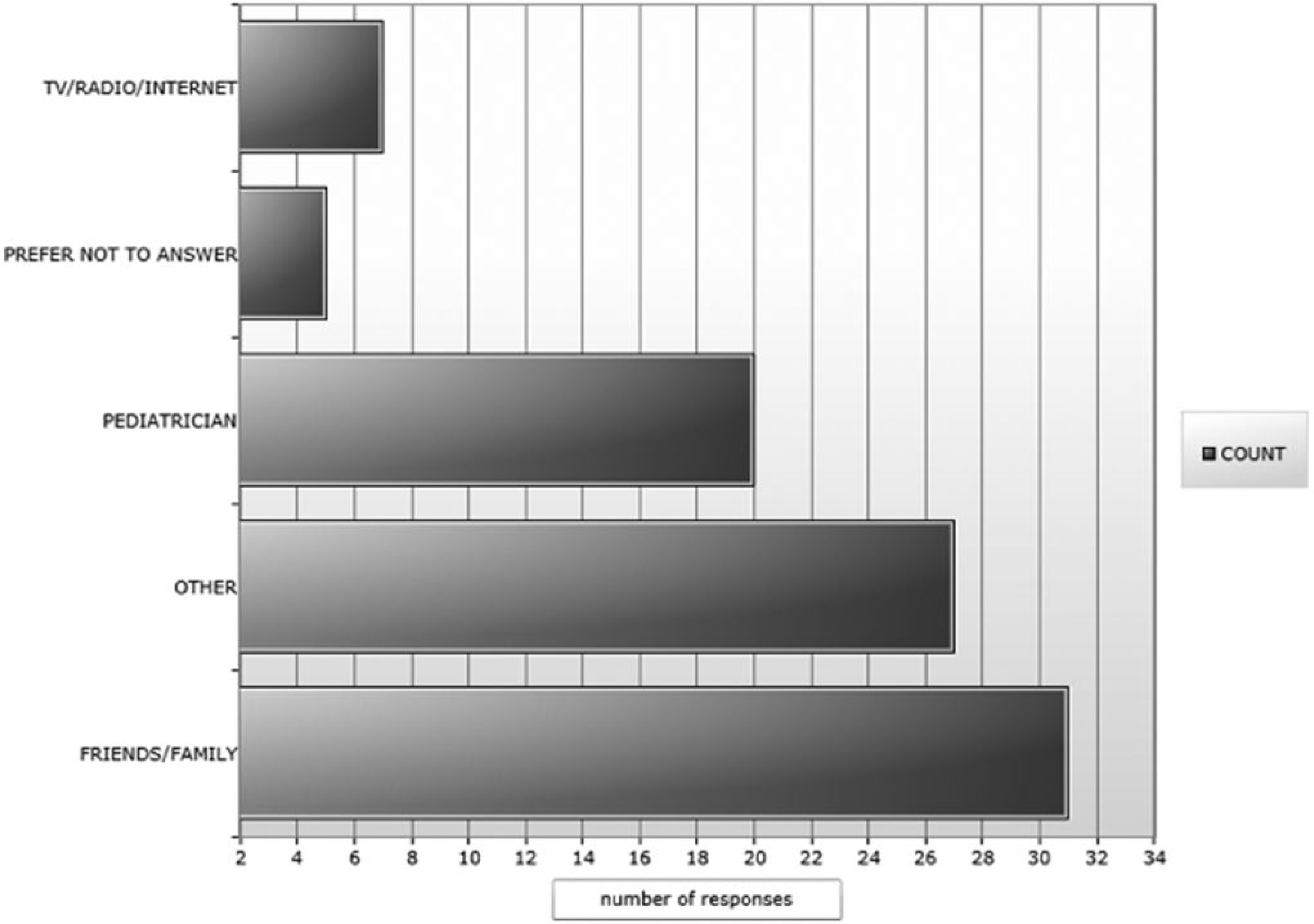
How did you learn about booster seats?
We used a Likert-type scale to ask our participants general knowledge and opinion questions pertaining to car safety and booster seats. They were asked if they strongly agree, agree, neither, disagree, or strongly disagree to the following questions. When asked if they believed accidents were a leading cause of death in children aged 4 to 10 years, 67% said they agree/strongly agreed. When asked if they believed that car crashes were common, 90% agreed or strongly agreed. Furthermore, when asked if they believed a booster seat could save their child’s life in the event of a car crash, 93% answered agree or strongly agree. Finally, regarding parenting style, parents/caregivers were asked to answer “always,” “sometimes,” or “never” to each scenario. The scenarios included children having temper tantrums and refusing to use a booster seat, a carpool situation, and the availability of booster seats. The majority of parents shared the “nonnegotiating” parenting style regardless of household income, level of education, caregiver’s age, and ethnicity. Of 100 participants, 88% answered never to giving into temper tantrums, and 63% stated that they always make sure others have a booster while driving their child. And the majority (93%) of the parents/caregivers were aware of car crash risks and were confident that using booster seats could save their child’s life (Figure 3).
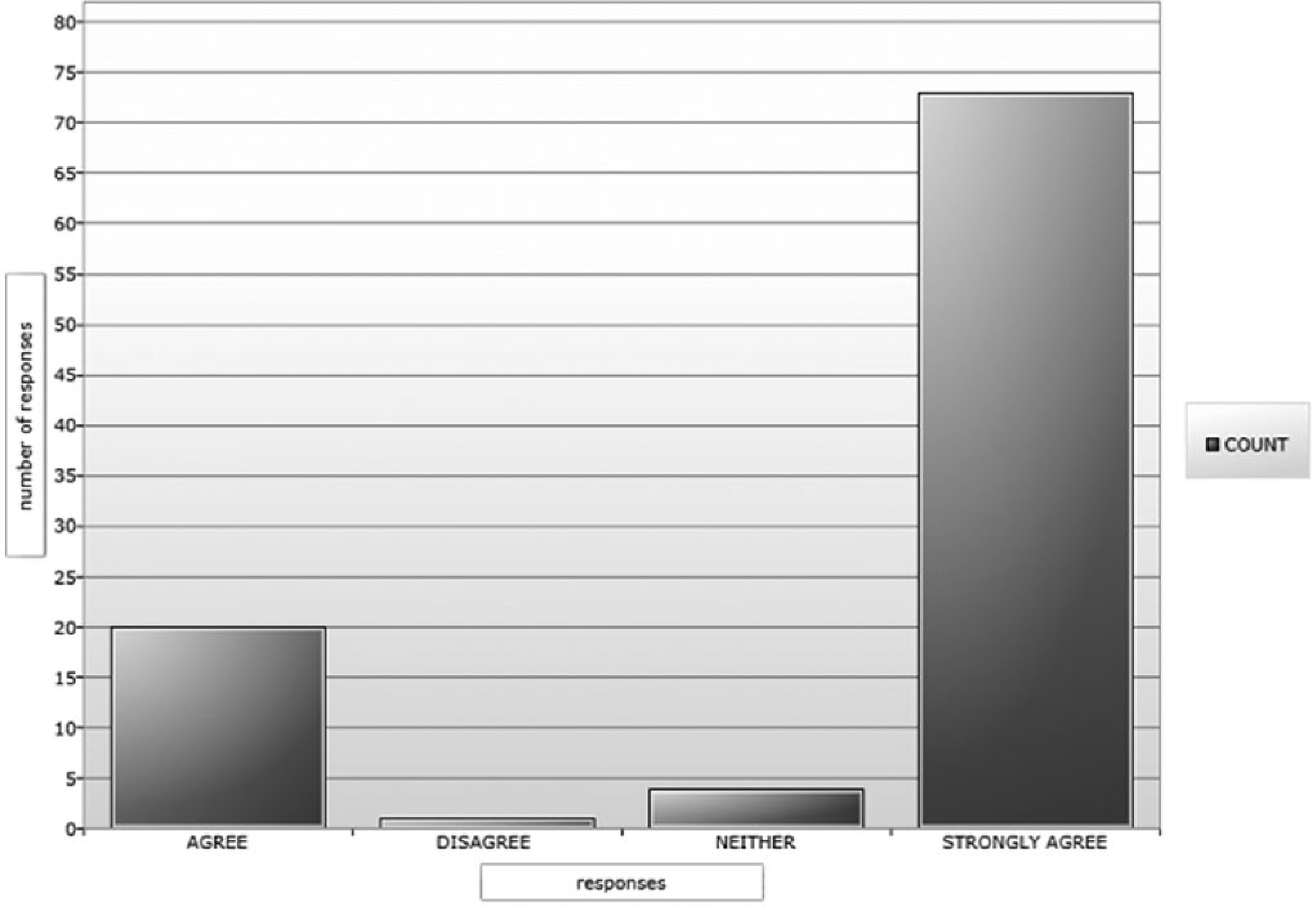
Do you believe booster seats can save your child’s life?
Discussion
Our study objective was 2-fold. First, determine the general use (past and /or present) of booster seats in a segment of emergency department patients in our community. Second, identify a caregiver’s knowledge of booster seat guidelines, awareness of the overall risk of car crashes, and parenting style that may pose as a potential barrier to appropriate use as well as continued use of booster seats. In our study, we found that the confidence in booster seats was evident, the concern for car crashes was apparent, but the gap in knowledge of when children can safely be transitioned to a vehicle seat belt system was lacking. Therefore, health care providers and public health officials should make a concerted effort to focus their attention on the continued use of booster seats beyond the 6 years of age to reduce the risk of preventable injuries and deaths from automobile crashes.
An interesting finding was that almost all the participants identified a pediatrician as their primary care provider, but only 20% reported being counseled on the proper use of booster seats. Additionally, we found that having a medical home did not ensure or guarantee the proper use of booster seats. Most of our participants identified family/friends or other (58%) as their source of knowledge regarding booster seats. Annual well visits are an excellent opportunity to cover a range of preventive care issues, such as child safety. According to our study results, reemphasizing the continued use of booster seats at annual well-visits beyond 6 years of age could prevent early transition due to lack of knowledge.
Although most were aware that Louisiana had a child passenger safety law, only 11% listed the law as the motivating factor for using a booster seat. The number one motivating factor was protection from injury. Parents/caregivers may be more receptive to pediatricians further educating them on the importance of keeping their child in a booster seat to prevent injury. However, if parents were primarily motivated by the law, their child will unfortunately continue to be susceptible to potential serious injury or mortality.6,12
The Louisiana child passenger law currently only requires children younger than 6 years and 60 lbs to use a restraint. The state lags behind best practice according to the AAP, which states that children should remain in a booster until they reach a height of 4 ft 9 in regardless of weight (on average, this is reached between the ages of 9 and 11 years). 13 This recommendation is based on the fact that standard automobile seat belt systems are designed for average adults, not children, and assumes adults wear the seat belt correctly with the seat belt crossing the shoulder without riding up the neck and crossing the upper thighs and not the waist. Proper use of a seat belt prevents life-threatening spinal cord injuries and intra-abdominal injuries.5-8 Clearly, having knowledge of the law is important but when it is not sufficient to protect from serious injury, it can give parents a false sense of security. In the case of our study, well-meaning caregivers/parents reported being primarily motivated by their child’s safety than law enforcement.
An important finding in the area of attitudes and opinions was that more than 90% of parents/caregivers were concerned about car crashes and their overall risk. They also reported a high level of confidence in the use of booster seats. Participants were receptive when learning booster seats protect their child from serious injury and could potentially save their child’s life. Therefore, this area is one that caregivers may not need convincing, instead child safety advocates as well as pediatricians can focus on educating parents on extending their use of booster seats and the potential dangers of premature graduation from booster seats.
Our study has several limitations. First, the majority of participants answered the scenarios given as “nonnegotiating” caregivers/parents instead of “negotiating” ones. Nonnegotiating by definition is a parent who sets rules and follows through regardless of a child’s behavior, peer pressure, and inconvenience. Whereas a negotiating parent may have less rules and allows a child’s behavior or demands to dictate choices. These results may have been biased by a parent’s need or want to be perceived as a “strict” parent, especially since we (their treating physician) were conducting the survey. If nonmedical personnel or a nontreating doctor gave the survey, a caregiver may be more comfortable providing a more honest or unbiased answer. Second, our survey population is relatively small, and although we attempted to obtain a diverse sampling pool of participants, no strict randomization method was used. Last, the emergency department population presenting with nonurgent/urgent complaints in this setting may be different from a population seen in a clinic setting. Although almost all participants reported having a pediatrician, there was no objective way to confirm this, thus leading to possible social desirability bias in this case.
Conclusion
Ultimately, child advocates, including pediatricians, must collaborate to emphasize and remind parents on best practice for booster seat transition according to the AAP. 10 The Louisiana Child Passenger Safety Law is limited, and guidelines that include specific heights, weights, and ages are difficult to remember. After providing all of our participants with the Boosters Are for Big Kids! 5-step illustrated handout on how to determine if their child can be transitioned from a booster seat, 100% of them rated it as more helpful than remembering specific parameters. 14 Variability in a vehicle’s backseat dimensions and various body proportions including childhood obesity all play a role in how a vehicle’s seat belt fits on a given child. This further supports an easy 5-step test that can be individualized for each child past the age of 8 years when safe transition to a vehicle’s seat belt system is more appropriate.
Author Contributions
JA-L conceptualized and designed the study, collected the data in the Emergency Department, analyzed the data, drafted the manuscript, and approved the final manuscript. LH reviewed and edited the data collection instruments, collected data in the Emergency Department, analyzed the initial data, reviewed and approved the final manuscript.
Footnotes
Acknowledgements
The authors thank Dr Evrim Oral, PhD, a biostatistician at LSUHSC School of Public Health for her initial review and revision of our data collection instruments, Carol A. Worsham at the CDC for her patience and guidance while teaching us how to use Epi info 7 statistical tools, and Kelly Allerton at the LSU Department of Pediatrics for reviewing and formatting our final manuscript for submission.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.