
Abstract

Rapid weight gain during the first year of life is associated with childhood obesity, adult obesity, and all its concomitant morbidities.1,2 Over the past 30 years, obesity among children 2 to 5 years old doubled. 3 As pediatric health care providers interact with young families routinely throughout the first few years of life, they may be in an ideal position to influence the rate of weight gain.
Innovations in care are needed: although past interventions have demonstrated that intensive anticipatory guidance leads to improved diet and eating habits, 4 within the current system of 12- to 18-minute well-child visits, it is unlikely that pediatric providers can provide this additional support. 5 Group well-child care, one such innovation, the provision of well-child care to 4 to 8 infant/parent dyads, allows providers greater interaction with patients.6,7 Prior analyses of group well-child care have found that group visits allow increased time for education, modeling behaviors, and parent-to-parent support.8-11 In group well-child care, there is an emphasis on maternal/infant relationships and parental self-efficacy, both of which have been associated with less obesity among preschool children, school-age children, and adolescents.12,13 We, thus, designed a follow-up study of participants in a group well-child randomized controlled trial (RCT) at Yale New Haven Hospital (YNHH) to determine the impact of group well-child care on childhood obesity.
This study is a follow-up of our initial RCT, conducted in 2008-2009. For the initial study, inclusion criteria were a mother/infant dyad with the infant in the mother’s care, gestation ≥37 weeks and born at YNHH, planning to use the YNHH primary care center (PCC), and with English as the primary language. On consenting to participate in the study, the mother/infant dyad was randomized to receive either group or individual care. In both arms, mother/infant dyads received the initial pediatric assessment at 2 to 4 days of life in a traditional model by a pediatric resident or a nurse practitioner (NP). In the control arm, for the first year of life, dyads received standard individual care provided by pediatric residents or NPs in the YNHH PCC. In the experimental arm, for the first year of life, dyads received all pediatric primary care in the group setting, led by NPs. The group well-child care intervention consisted of eight 90-minute sessions through the first year of life when the children were 2 weeks, 1 month, 2 months, 3 months, 4 months, 6 months, 9 months, and 12 months old. 14 After 1 year, all dyads received pediatric primary care in the traditional model.
Initially, 97 dyads were enrolled; 55 were allocated to treatment and 42 to control. Mothers in both arms completed questionnaires within the first month of the infant’s life and after their children were 12 months old. The data from the children of the 63 mothers who completed the survey at both baseline and 12 months—40 of whom were assigned to group and 23 to individual well-child care—are included in this analysis.
We collected data through retrospective chart review of electronic medical records from the pediatric primary care outpatient records and participants of the original RCT using the infant’s name and date of birth. We abstracted data on health behavior variables, height, weight, and body mass index (BMI) from records at 24 months, 30 months, and 36 months. We defined loss to follow-up as attrition from the sample by the 24-, 30-, or 36-month visit. The Yale Medicine Human Investigation Committee approved this study protocol.
To assess nutritional behaviors, we selected variables reflective of the priorities of the 5-2-1-0 Let’s Go initiative by the American Academy of Pediatrics, including the consumption of 5 or more servings of fruits or vegetables in 1 day, 2 hours or fewer of screen time, participation in a minimum of 1 hour of physical activity, and consumption of zero sugar-sweetened beverages. 15 In the YNHH PCC electronic medical record, the health care provider is prompted to assess these behaviors at 24, 30, and 36 months; however, given the variability with respect to documentation and missed visits, for each outcome, we collapsed the 3 separate visits into 1 variable to indicate whether the child had ever, over the course of the visits, demonstrated the behavior.
Second, we assessed height, weight, BMI, and BMI percentile for age and gender at 24, 30, and 36 months. To ensure consistency across the sample, we calculated BMI and BMI percentiles, using a calculator provided by the Centers for Disease Control and Prevention.16,17 We converted BMI percentiles into z-scores. We classified individuals as overweight or obese corresponding to a BMI percentile greater than 85% and 95%, respectively. We created 2 variables to capture overweight status and obesity at any of the 3 visits: ever overweight and ever obese.
We first assessed differences in outcome means across treatment and control groups using t tests and χ2 tests. Second, we used regression analysis to assess differences controlling for race, gender, birth year and birth month of the child, age of the mother, and mother’s total number of living children at the time of the patient’s birth. We created indicator variables for female gender, race, and ethnicity categories, which we used as controls. We used STATA 12 SE (College Station, TX) statistical software for all analysis.
The sample consisted of 63 dyads, 40 of whom were randomized to group care and 23 to individual care (Table 1). The 2 groups were not significantly different with respect to child’s race, child’s gender, mother’s age, mother’s number of living children, or loss to follow-up. Of the total sample, 27.0% were lost to follow-up by the 24-month visit, 30.2% by the 30-month visit, and 39.7% by the 36-month visit. Broken down by treatment status, 26.1% of control-group children (6 individuals) and 27.5% of treatment-group children (11 individuals) were lost to follow-up by 24 months (Table 1).
Comparison of Characteristics of Group and Individual Well-Child Care (n = 63).
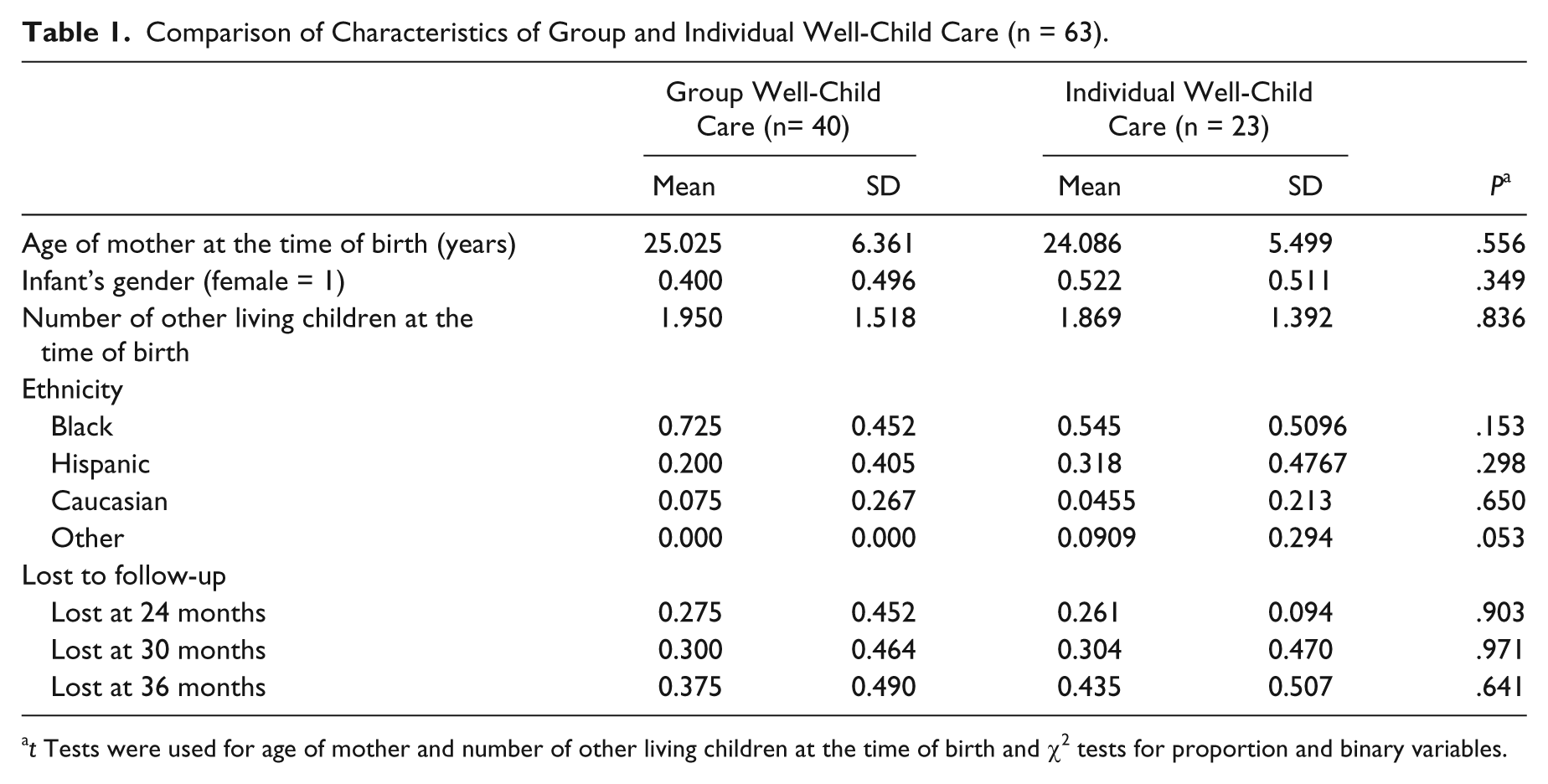
t Tests were used for age of mother and number of other living children at the time of birth and χ2 tests for proportion and binary variables.
For the whole sample, the average BMI z-scores were −0.0439, 0.182, and 0.0268 at 24, 30, and 36 months, respectively, and 21.1% were ever overweight. At 24, 30, and 36 months, the average BMI z-scores for participants in group care compared with individual care were, respectively, 0.0567 and −0.0262 (P = .921), 0.133 and 0.276 (P = .720), and −0.0355 and 0.156 (P = .599) (Table 2). In the first 3 years of life, 16.0% of group participants and 30.7% of individual care participants were ever overweight (P = .289) (Table 2). Only 5.3% of children in the sample were obese; thus, obesity is not used as an outcome for further analysis in this study.
Comparison of Outcomes of Group and Individual Well-Child Care.
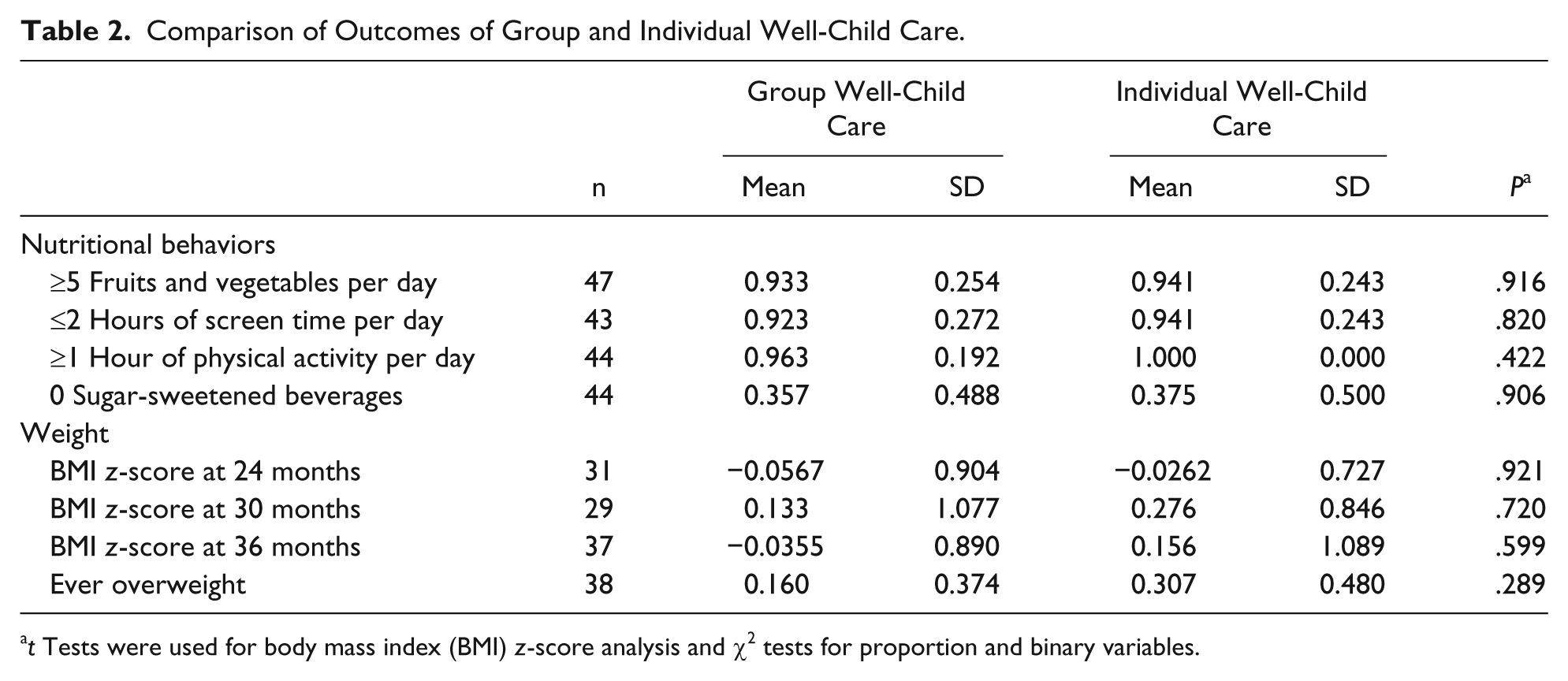
t Tests were used for body mass index (BMI) z-score analysis and χ2 tests for proportion and binary variables.
Multivariate regression analysis did not reveal significant differences between group and individual well-child care for any outcome, although there was a trend toward group participants being less ever overweight compared with individual care participants. Mean rate of ever overweight was 16% and 30.7% for group and individual care, respectively, and this difference grew from 14.7 to 34.9 percentage points (P = .098, Table 3) after adjusting for race, gender, birth year and birth month of the child, age of the mother, and mother’s total number of living children at the time of the patient’s birth.
Impact of Group Well-Child Care on Ever Overweight: Multivariate Regression. a
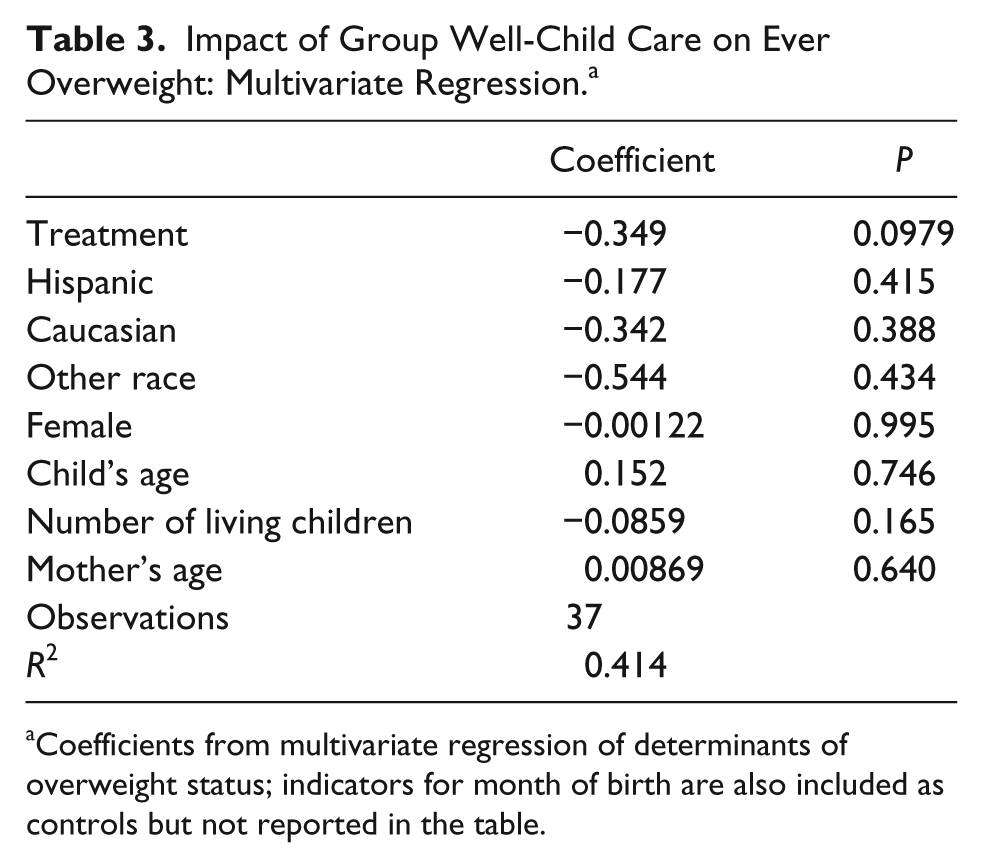
Coefficients from multivariate regression of determinants of overweight status; indicators for month of birth are also included as controls but not reported in the table.
In a 2-year follow-up of a RCT of group versus individual well-child care, we found no statistically significant differences in nutrition-related behaviors, BMI percentile, or proportion of overweight or obesity. We did, however, find a trend of less ever-overweight children randomized to group compared with individual care (16% vs 30.7%).
Given our small sample size, we hypothesize that this finding may become statistically significant with data from a larger study. Because there was no specific emphasis on healthy eating and physical activity in the group compared with individual well-child care but there was an emphasis on maternal/infant secure attachment and parental self-efficacy in group care, we hypothesize that group care may lead to healthier weights, and it may be mediated through maternal/infant secure attachment and parental self-efficacy. Anderson et al 12 posit a pathway from parent-child attachment to unhealthy physiological and behavioral responses to stress, to sleep disturbance and hormonal lability, to obesity. 13 In a study comparing obesity prevention guidance focused on changing maternal eating behaviors and guidance focused on changing child eating behaviors, French et al 18 found better feeding behavior outcomes in children among the mother-focused group. Together, these studies present a compelling case for our hypotheses—empowering mothers, through interventions such as group well-child care, may be key to obesity prevention.
In conclusion, although we did not find statistically significant support for the hypothesis that group well-child care in the first year of life altered weight-related health outcomes during early childhood, we found potentially promising trends. Group well-child care may be a viable option for well-child care because the visit structure can be cost-saving or cost neutral and is an example of efficient distribution of health care resources. 19 Moreover, increased time with patients and the opportunity for more in-depth discussion and counseling may increase provider and patient satisfaction, 14 both of which may lead to better health outcomes.
Author Contributions
NBS, AMF, and MSR contributed to conception, design, acquisition, analysis, interpretation of data and drafting of the manuscript. Each author participated in critical revisions and final approval.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.