
Abstract
Background. End-of-life care for a child is an emotionally charged experience for pediatric trainees. Objectives. Describe the progression of medical trainee experiences with end-of-life care and determine personal/professional experiences that facilitated integration of experiences. Methods. Medical students (MS4) and pediatric residents (PL-1-3) completed a 30-question survey about experiences with patient deaths and integration of these experiences. Results. A total of 307 of 404 residents (76%) participated. Mean number of deaths ranged from 3.0 to 6.5 in the prior 12 months, and the most common location was neonatal intensive care unit or pediatric intensive care unit. In total, 18% to 27% experienced a death in their personal life. Between 26% and 41% of the residents made contact with a family after death, and 15% to 35% attended a funeral. Characteristics of good deaths included good communication and discussion of end-of-life issues. Conclusions. Trainees experienced patient deaths along the educational continuum. These findings have implications for the optimal timing and method of end-of-life care education.
Introduction
The death of a child is a distressing and permanent event that marks a premature loss of human potential. Caring for a child at the end of life and witnessing the child’s death can be an emotional experience for both the child’s family and health care workers. 1 In the United States, there are approximately 20 000 pediatric deaths per year ranging from sudden deaths due to unintentional injury, homicide, suicide, and infections to deaths resulting from chronic conditions, including congenital malformations, heart disease, and malignancies. 2 Throughout the end-of-life period, parents seek complete information, access to emotionally invested staff, providers who will remain present, organized coordination of care, and health care providers who nurture and respect the parent-child relationship. Parents also acknowledge the importance of their faith and spiritual beliefs in coping with their grief. 3 Compassionate, honest, transparent, and coordinated end-of-life care conversations with physicians and other health care providers can have a powerful impact on the process of grieving for patients’ families and loved ones. If information is delivered well, physicians can act as a source of comfort and compassion. However, if information is delivered poorly, physicians can potentially elicit further distress and pain. 4 In addition, after the death of a child, parents often desire a meeting with their child’s physician to discuss the chronology of end-of-life events, receive emotional support, discuss their feelings and review autopsy results if performed. 5
Unfortunately, physicians in general and pediatric residents in particular often feel that they are not adequately trained to maneuver through these emotionally challenging responsibilities.6,7 Pediatric attending physicians who considered themselves knowledgeable about ethical issues expressed substantial variability in their views on end-of-life care, which often do not coincide with published recommendations. 8 According to a study of pediatricians from the New York Hospital, only 8% of residents and 28% of fellows reported receiving end-of-life care training while in residency. 9 In a telephone survey of faculty, residents, and medical students at multiple US academic centers, 31% of residents and 39% of students felt poorly prepared to talk to patients regarding fears about dying, while more than 50% of residents felt poorly prepared to manage spirituality or discuss pertinent cultural issues. 10 However, in many instances pediatric residents are expected to manage end-of-life care decisions without adequate training.1,6,11,12
The Institute of Medicine recommends that medical, nursing, and other health professionals that work with children should have adequate training and competence in palliative, end-of-life, and bereavement care. The Academic Pediatrics Association published educational guidelines and included a statement on Palliative Care for Children that stressed the need to identify and address barriers and facilitators for health care professionals in providing effective palliative care. Among the recommendations in this document are to encourage incorporation of “palliative medicine, communication skills, and addressing grief and loss” within residency training. Figure 1 presents a conceptual model that outlines the numerous facilitators and barriers that can play a role in the pediatrician’s ability to ultimately integrate the end-of-life experience. 13 Developed by Serwint et al through a review of the literature, the model emphasizes that past experiences and specific case factors influence the impact of the pediatric death on the resident, while guilt and coping mechanisms can influence the grief process. 13 While developed for pediatric residents, this framework has relevance to pediatric health care professionals at all stages of their career.
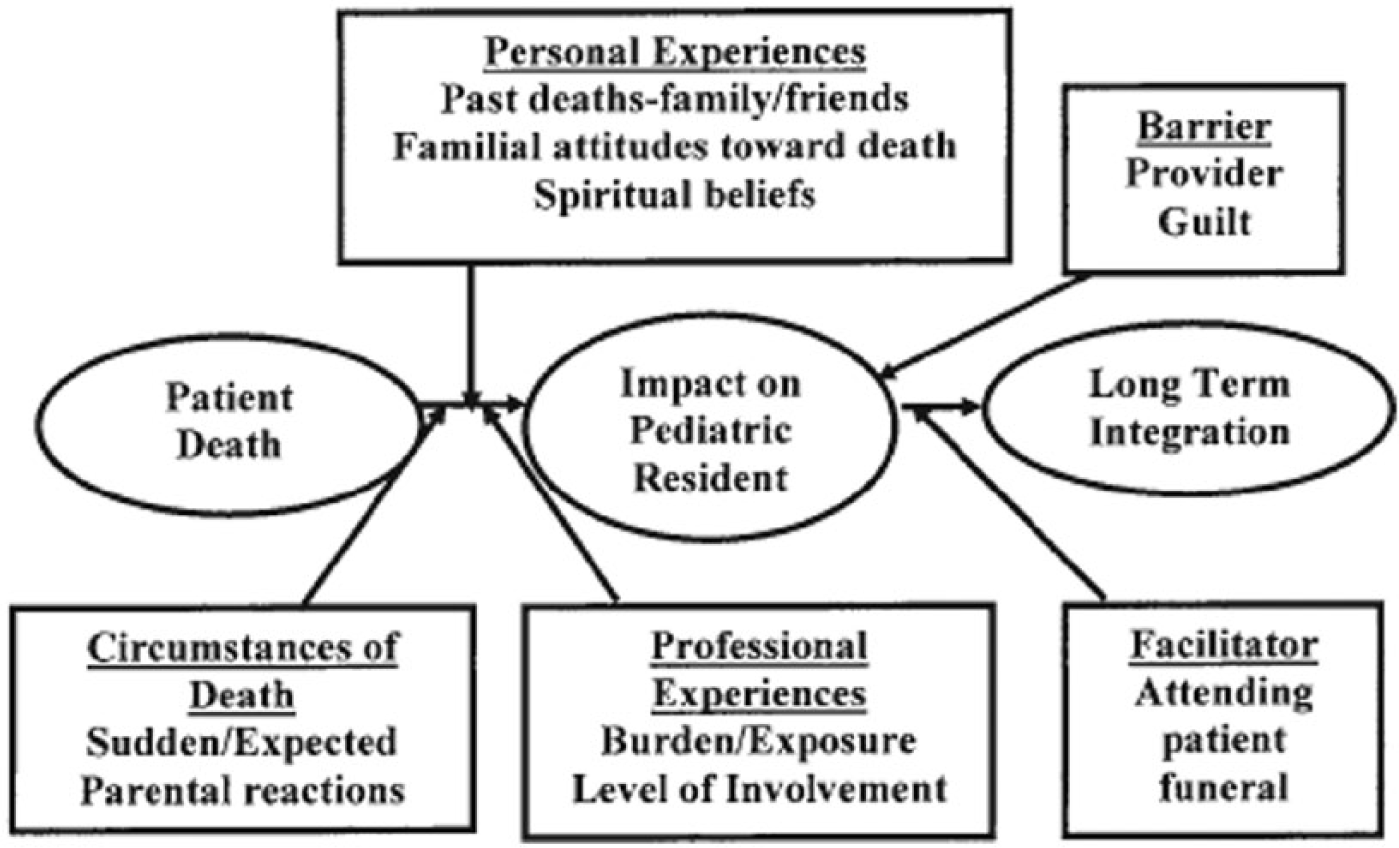
Conceptual framework of factors involved in pediatric resident’s integration of patient’s death.
Past studies of residents’ end-of-life experiences have been cross-sectional and have not examined residents’ perspectives of what constitutes a “good death” or the professional and personal experiences that helped them cope with patient deaths. A clear understanding of these experiences and perspectives would assist educators develop interventions to train pediatric residents to more effectively manage end-of-life discussions and subsequently improve end-of-life care for patients. The objectives of this study are to (1) describe the progression of medical trainee experiences with end-of-life care from medical school through the end of pediatric residency training and (2) document personal and professional experiences that facilitated coping with and integrating end-of-life care experiences.
Methods
Setting and Study Participants
This study was conducted in a pediatric residency training program at an academic medical center in Baltimore, Maryland, during 2001 to 2004. The participants included graduated 4-year medical students entering the pediatric program and pediatric residents. The survey was distributed annually in June of the academic years spanning from 2001 to 2004.
PL-1 residents completed rotations in the pediatric emergency department, general inpatient wards, subspecialty inpatient ward and clinics, outpatient acute clinic, and neonatal intensive care unit (NICU). PL-2 residents completed rotations in the pediatric emergency department, the pediatric intensive care unit (PICU), pediatric oncology/hematology units, developmental pediatrics wards and clinics, and adolescent medicine clinics. PL-3 residents provide supervision in the same areas covered by PL-1 residents and train on the general surgery service. Residents at all levels of training also participate in a weekly continuity experience. An annual death and bereavement seminar is held for PL-2 residents to review end-of-life issues and pratice sharing bad news with standardized patients.
Survey Development
A 30-question survey was developed to address aspects of the conceptual framework of death integration presented earlier. Since no validated tool had been previously developed, the authors designed the survey using outcomes developed from past publications.1,4,9,10,12-15 A paper copy of the survey was distributed in June each year to MS-4 students and PL-1, PL-2, and PL-3 pediatric residents at a training program at an academic medical center in Baltimore, Maryland. The survey asked about experiences over the prior 12 months of training and took 20 to 30 minutes to complete. Institutional review board approval was obtained.
Survey Outcomes
Participants were asked about the number of deaths they had experienced in their personal and professional lives over the preceding 12 months. To capture deaths that occurred while the trainee was actively caring for the patient as well as deaths that occurred in patients for whom the trainee may have provided prior care and developed a relationship, the survey asked, “How many of the patients for whom you have provided care have died in the past year?” The survey also asked about the location, circumstances and type of death, and whether the resident had served as the primary informant to the family. Type of deaths were divided into 5 categories: (1) sudden deaths in previously healthy patients, (2) anticipated deaths, (3) unexpected deaths with chronic conditions but low likelihood of death, (4) unexpected death with high-risk condition, and (5) deaths not otherwise categorized. Categorizing death was intended to better understand educational interventions, as sudden and unexpected deaths have been found to cause more anguish and difficulty with integration in health care professionals. Respondents were additionally asked about feelings of guilt, participation in post-death debriefings, attendance at funerals, and initiation of contact with patients’ families after the death. Post-death debriefings were not formally defined in the survey, but reference to them within the training program included a discussion about the circumstances of a death with either an individual or team, possibly also including medical management, emotional components, and impact on the care team. Residents were also asked to reflect on whether they thought each death was handled well or poorly, reasons for this belief, and personal and professional experiences that helped them with the integration of patient deaths. The medical students (MS-4) completed the same survey as the pediatric residents in training except they were not asked to categorize the type of deaths.
Statistical Analysis
The Statistical Program for Social Sciences SPSS (version 10.0) was used to perform analysis of frequencies and mean scores for each group categorized by level of training. Responses to open-ended questions were clustered into themes and reported.
Results
During academic years 2001 to 2004, 404 trainees were invited to complete the survey and 307 (76%) completed the survey. These trainees included 97 MS-4, 68 PL-1, 65 PL-2, and 77 PL-3 residents.
End-of-Life Care and Death Experiences
The majority of trainees experienced at least one patient death during the preceding 12 months (Table 1). PL-2 residents reported experiencing the highest mean number of patient deaths (mean 6.5, range 1-20). Three percent to 7% of trainees reported experiencing the death of a continuity patient, while 18% to 21% experienced a death within their personal life during the previous 12-month time period.
Number and Characteristics of Deaths During the Prior 12 Months.
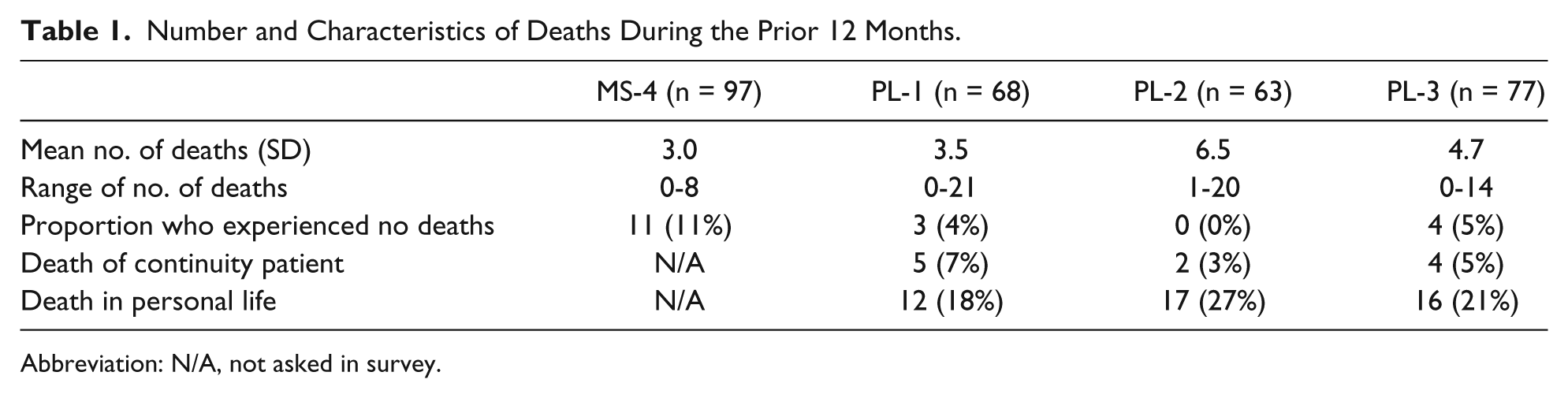
Abbreviation: N/A, not asked in survey.
The location of patient deaths varied by year of training (Table 2). The largest proportion of patient death experiences for MS-4 trainees occurred on the adult inpatient units (51%). For PL-1 residents, 69% of deaths occurred in the NICU and PICU, 67% for PL-2, and 62% for PL-3 residents. Among PL-1-3 residents, experiences with unexpected, high-risk patient deaths were most common and accounted for 40% to 62% of all patient death experiences (Table 3).
Locations and Types of Deaths During the Prior 12 Months by Level of Training.
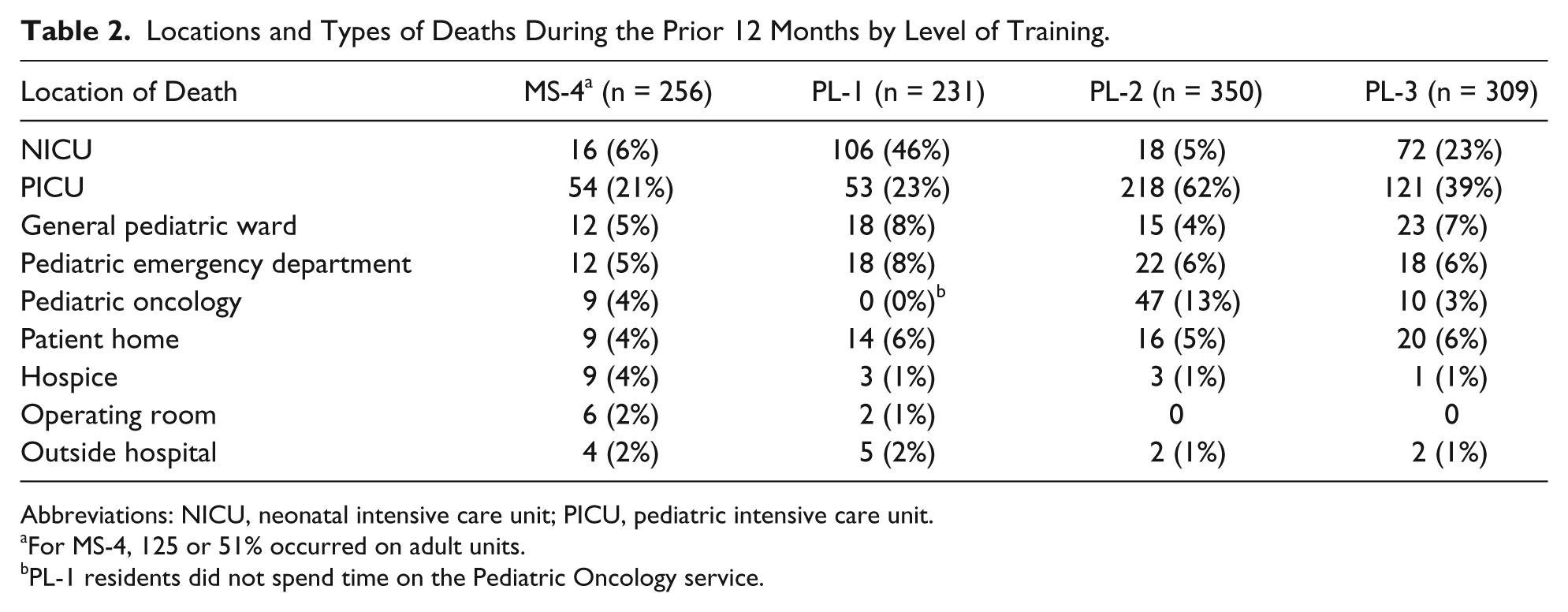
Abbreviations: NICU, neonatal intensive care unit; PICU, pediatric intensive care unit.
For MS-4, 125 or 51% occurred on adult units.
PL-1 residents did not spend time on the Pediatric Oncology service.
Types of Deaths During the Prior 12 Months.
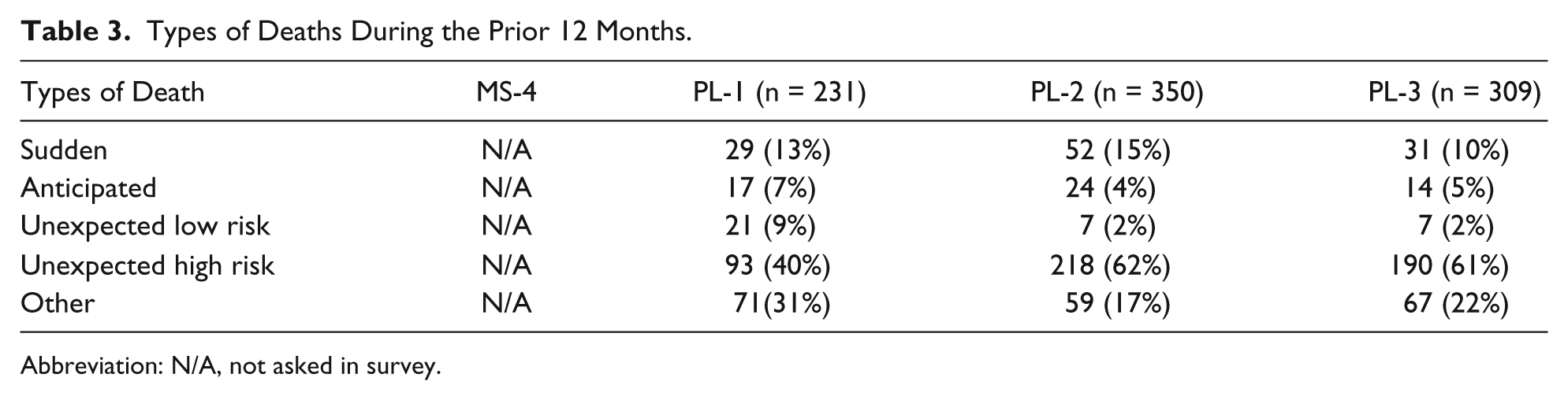
Abbreviation: N/A, not asked in survey.
Qualitative Perceptions of Death
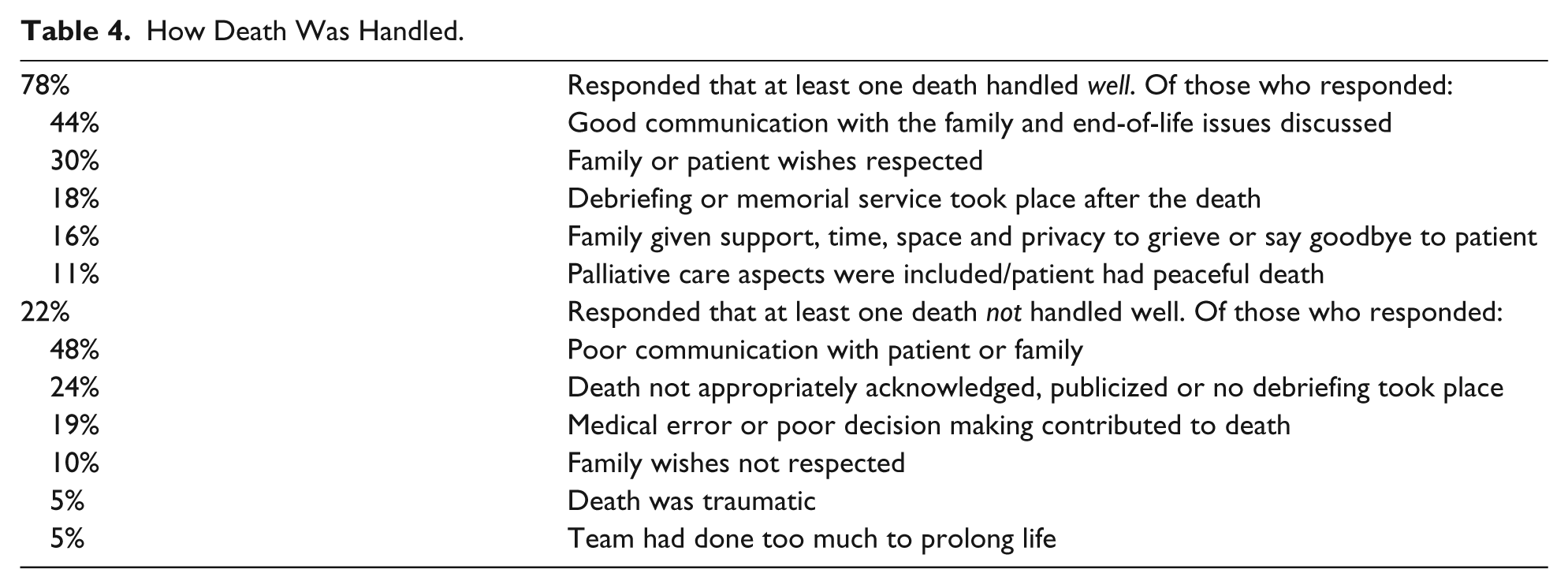
Of all trainees, 78% experienced at least one patient death they felt was well-handled. Good communication with the family and patient was the most commonly cited reason for this perception (Table 4). Lack of communication was the most commonly cited reason for believing that a death was not handled well.
How Death Was Handled.
Barriers and Facilitators of Integrating Patient Deaths
The proportion of residents that experienced guilt increased with level of training (26% of MS-4 trainees vs 69% of PL-3 residents). None of the MS-4 trainees served as a primary informant for a patient death, whereas 20% of PL-1-3 residents served as primary informants. Less than half of trainees at any level of training participated in debriefing after experiencing a patient death (Table 5).
Barriers and Facilitators by Resident.
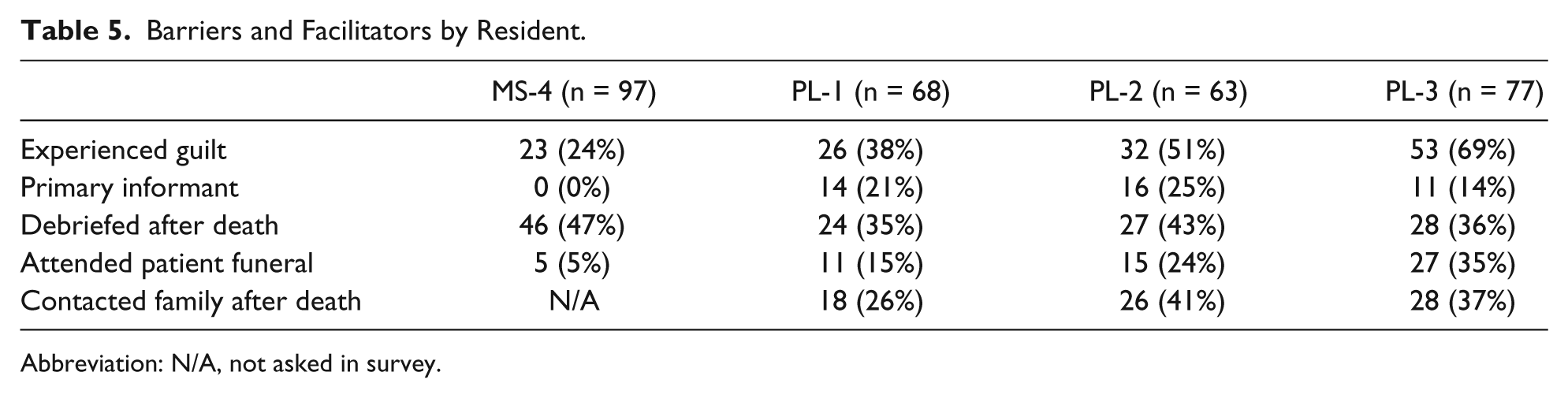
Abbreviation: N/A, not asked in survey.
After experiencing patients’ deaths, 26% of PL-1 residents, 41% of PL-2 residents, and 37% of PL-3 residents contacted the patient’s family. Of all residents that made contact, sending a card was the most common form of contact (78%), followed by phoning the family (30%). Only 14% of residents who contacted a family did so through a follow-up visit in person at the medical center. Overall, of trainees who experienced a patient death, 15% of PL-1, 24% of PL-2, and 35% of PL-3 residents attended a patient’s funeral. Their reasons for funeral attendance included feeling close to the family or patient (56%), to show support for the family (40%), and for personal closure (26%). Of trainees that did not attend a patient funeral, 47% reported not being able to get time off as a reason for not attending.
Coping With and Integrating Death Experiences
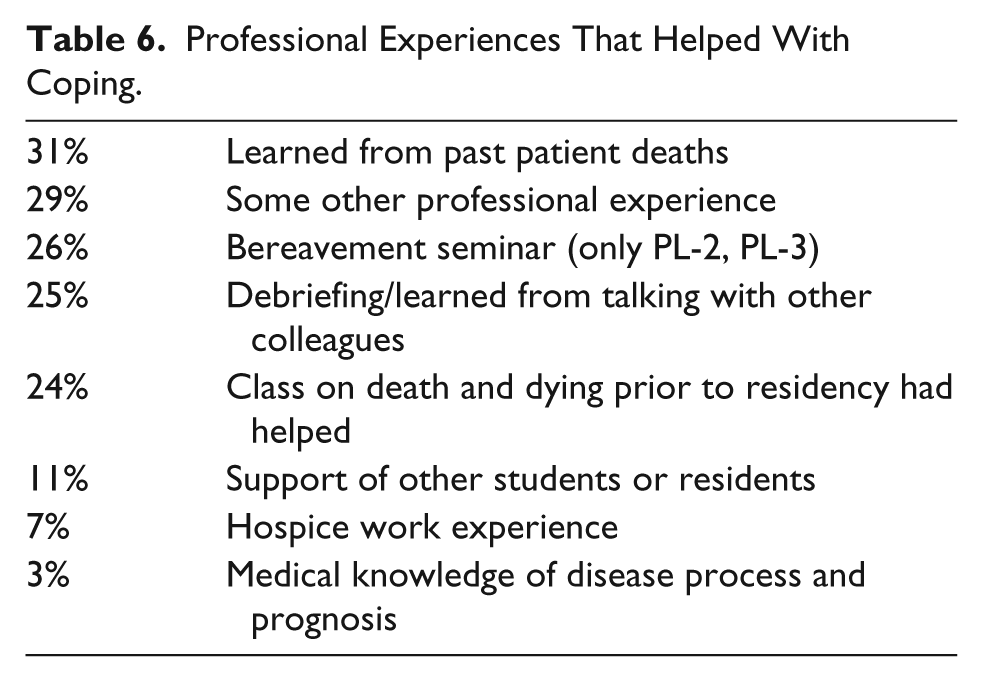
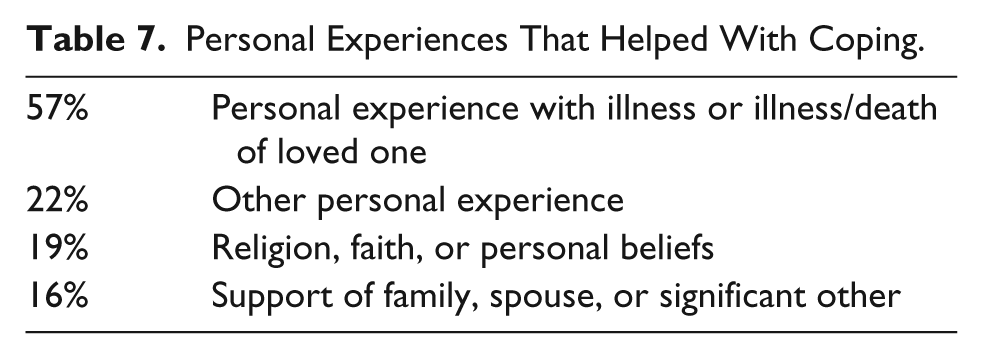
With regard to professional and personal experiences useful for integrating patient death, respondents were asked to generate and remember useful experiences rather than being offered a series of choices. Among MS-4 respondents, 33 (46%) felt that a death and dying course during medical school was useful, while 19 (26%) felt that modeling or talking with an attending or fellow was worthwhile. Thirty-one percent of PL-1-3 residents cited involvement with prior patient deaths as helpful. Among PL-2 and PL-3 residents who had participated in a bereavement seminar given during the second year of residency training, 26% spontaneously mentioned the seminar as useful. Twenty-five percent of residents noted debriefing or talking with their colleagues as beneficial. Fifty-seven percent of trainees reported that their experiences with illness and/or the death of family or friends helped them cope with patient deaths (Tables 6 and 7).
Professional Experiences That Helped With Coping.
Personal Experiences That Helped With Coping.
Discussion
To our knowledge, this is the first study to document medical trainee experiences with pediatric deaths across the continuum from the latter year of medical school through pediatric residency training. These findings have implications for the optimal timing and method of end-of-life care education in the medical school and pediatric residency curricula.
Frequency and Nature of Death Experienced
In this study, pediatric residents experienced the majority of patient deaths in the PICU and the NICU, consistent with previous studies. 14 Of note, the distributed questionnaire was designed to include any patients that the residents cared for, even if the residents themselves were not on the same service during the pediatric death. PL-2 residents experienced the most deaths, which is consistent with the proportional amount of time they spent in the PICU. However, pediatric trainees of all levels did experience pediatric deaths, with medical students experiencing the least, at an average of 3.0 deaths during the prior 12 months.
Reactions to Deaths and Factors Influencing Emotional Distress
The proportion of residents who experienced feelings of guilt after patient deaths increased from 26% among MS-4 trainees to 69% among PL-3 trainees, which may coincide with increasing responsibilities as a health care provider or reflect cumulative experiences with patient deaths. Guilt was experienced by a higher proportion of trainees in this study compared to past studies. 13 In another study at this institution, remorse over the rigor of therapy, resident inexperience, underestimated patient acuity, and a lack of resident compassion were associated with feelings of guilt among residents after patient deaths. 12 Sahler et al have described guilt in the pediatric end-of-life setting as a reaction that can lead to both emotional and physical distancing between the provider and the family, which may contribute to physician dissatisfaction and ultimately to burnout. 15
Professional and Personal Experiences
Of the professional experiences surveyed, residents self-reported benefit most from past experiences with patient deaths and formalized didactics on death and dying. Formal didactic sessions included both coursework prior to residency as well as bereavement seminars offered to residents. 16
Across all levels of training, debriefing occurred in the minority of pediatric deaths, which is consistent with past data. 16 Debriefing or discussion with colleagues was seen as beneficial to 25% of survey respondents. Possible explanations for this could include a low rate of debriefing after patient deaths or inconsistently mediated debriefing. Although many professional societies do endorse debriefing, no empirical evidence has yet proven a benefit for resident mental health.
When analyzing personal experiences that affect the impact of pediatric death on trainees, the majority found their own family illnesses or deaths as being helpful. A study of PL-2 residents at the same institution indicated that only 30% of personal deaths were openly discussed within their family, postulating that these residents may need more explicit training to gain comfort with death and dying. 13
Limitations
This study was conducted at a single institution, and there may be unique institutional cultural issues that affect the responses. Trainees were surveyed annually, which may lead to recall bias as to the precision of whether the death truly happened within the past 12 months. Hence, the number and descriptions of death could be inflated or decreased depending on how the resident completed the survey. Finally, residents may be more likely to recall patients with longer duration of illness or those who experienced sudden or unexpected deaths if these experiences were more memorable.
Recommendations
There have been numerous approaches to effectively educate and acclimate health care workers to meaningful end-of-life care. Some groups believe that the addition of interactive seminar sessions can be highly educational and self-reflective.16,17 Other groups believe that residency programs must change their culture so that palliative care cases are consistently introduced and end-of-life situations are identified as irreplaceable “teachable moments.”15,18 Others recommend both formal curricular change as well as informal cultural change that include developing palliative care leaders, enhancing end-of-life education resources, and faculty development.10,19 Regardless of the method of action, significant strides must be made in the quality and nature of end-of-life care education.
The content of educational interventions should be geared toward not only creating an ideal environment for the patient and family but also to best allow the trainee to appropriately integrate the pediatric death. One way to maximize the utility of this approach is to mirror the conceptual framework of pediatric resident’s integration, which is included earlier in this document.
First and foremost, resident and student end-of-life care education should be incorporated throughout the entire educational curricula. This is especially important if first-year residents are acting as primary informants. Although there are some rotations where pediatric death is more prevalent, the experiences are pervasive throughout all levels of training and rotations. The areas with more frequent pediatric deaths could be arenas for more intensive exposure and education. The majority of deaths were described as unexpected, but in high-risk patients, which may warrant skill building for managing highly urgent end-of-life care discussions or emphasizing the early introduction of end-of-life conversations for all high-risk patients.
Though death and dying courses and bereavement seminars have not been empirically studied, respondents in this study reported benefit. We recommend that educators strongly consider initiating their own versions of formal didactics to discuss, educate, and understand concepts surrounding death and dying. Upper level clinicians should continue to utilize these emotionally charged situations as teachable moments for both residents and medical students.
This study showed that many trainees found personal experiences beneficial to the integration of pediatric death. We propose that residency directors and medical schools should promote a culture of openness of personal experiences, facilitation of existing emotions including guilt, as well as edification and acceptance of spiritual beliefs. Mental health care providers should be readily accessible in order to optimize resident and student emotional health throughout these trying experiences.
We also recommend further study of standardized debriefing for end-of-life care experiences. Though not yet supported in the literature, the experiences may be highly variable depending on the facilitator and environment; a study to assess the efficacy of formal and consistent debriefing after pediatric deaths is warranted.
Finally, funeral attendance should be encouraged by developing a coverage system to allow trainees this opportunity to help facilitate this emotional learning experience.
Author Contributions
KS participated in the data analysis, interpretation of the data, writing the manuscript drafts and final review of the manuscript. JRS developed the original study purpose, developed the survey, paraticipated in the implementation of the study, particpated in the data analysis, interpretation of the data, review of the drafts and the final manuscript. FSD participated in the implementation of the study, cleaned the data, participated in the data analysis and reviews of the drafts resulting in the final manuscript
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.