
Abstract

Case Report
A 15-year-old boy presented to the emergency department at a referring facility with right lower extremity weakness and numbness. He reported being bitten in the right inguinal region by a spider similar in appearance to a brown recluse several hours prior to symptom onset. He first developed redness and pain at the site of the bite followed by stiffening, numbness, tingling, and weakness of the entire right lower extremity, intermittent right digital paresthesias, diffuse myalgias, headache, and abdominal pain. His initial examination was significant for an area of ecchymosis and erythema on his anterior right hip consistent with the location of the reported bite, inability to move his right lower extremity, slightly decreased right hand strength, decreased sensation to light touch over entire right lower extremity, and right patellar areflexia. The patient reported difficulty urinating, and a postvoid bladder ultrasound revealed a residual of approximately 1 L of urine. Initial evaluation, including a complete blood count with differential, basic metabolic panel, urinalysis, and magnetic resonance imaging (MRI) of the lumbar spine was normal.
The patient was started on intravenous steroids for empiric treatment of transverse myelitis. However, over the course of the next 24 hours, the weakness spread to the contralateral lower extremity with ascending numbness to the umbilicus. Negative inspiratory forces decreased from −30 to −10 cm H2O with associated dyspnea and increased work of breathing. He was subsequently sedated, intubated, and transferred to the pediatric intensive care unit at a tertiary care children’s hospital.
Following transfer, it was noted that his initiated breaths on the ventilator were in excess of 500 mL with minimal support. Based on this finding, sedation was held and he successfully passed an extubation readiness assessment of tidal volumes on CPAP/PS (continuous positive airway pressure with additional pressure support). He was then extubated to room air without complication. His neurologic examination after extubation was significant for 0/5 strength in bilateral lower extremities, 4/5 bilateral intrinsic hand muscle strength, bilateral patellar areflexia, bilateral flaccid Babinski, and loss of sensation to pinprick below T5-T6 but marked pain with rectal tone assessment. No other motor or sensory disturbances were noted.
Despite the apparent rapid recovery of respiratory muscle strength and pain with rectal tone assessment being inconsistent with other reported sensory deficits, the presence of areflexia and the progression of neurologic dysfunction leading to intubation was concerning. Therefore, extensive serum laboratory testing was undertaken, including repeat complete blood count with differential and chemistry panel, erythrocyte sedimentation rate, C-reactive protein, fourth-generation HIV antigen/antibody test, rapid plasma reagin (RPR), and enterovirus polymerase chain reaction (PCR) on nasopharyngeal swab, all of which was unremarkable. Lumbar puncture was performed, and cerebral spinal fluid (CSF) studies, including oligoclonal bands and CSF:serum albumin ratio, were normal (Table 1). The local poison control center was contacted, and they confirmed that no spider endemic to the area produces a toxin known to cause ascending paralysis.
The Results of the Diagnostic Evaluation.
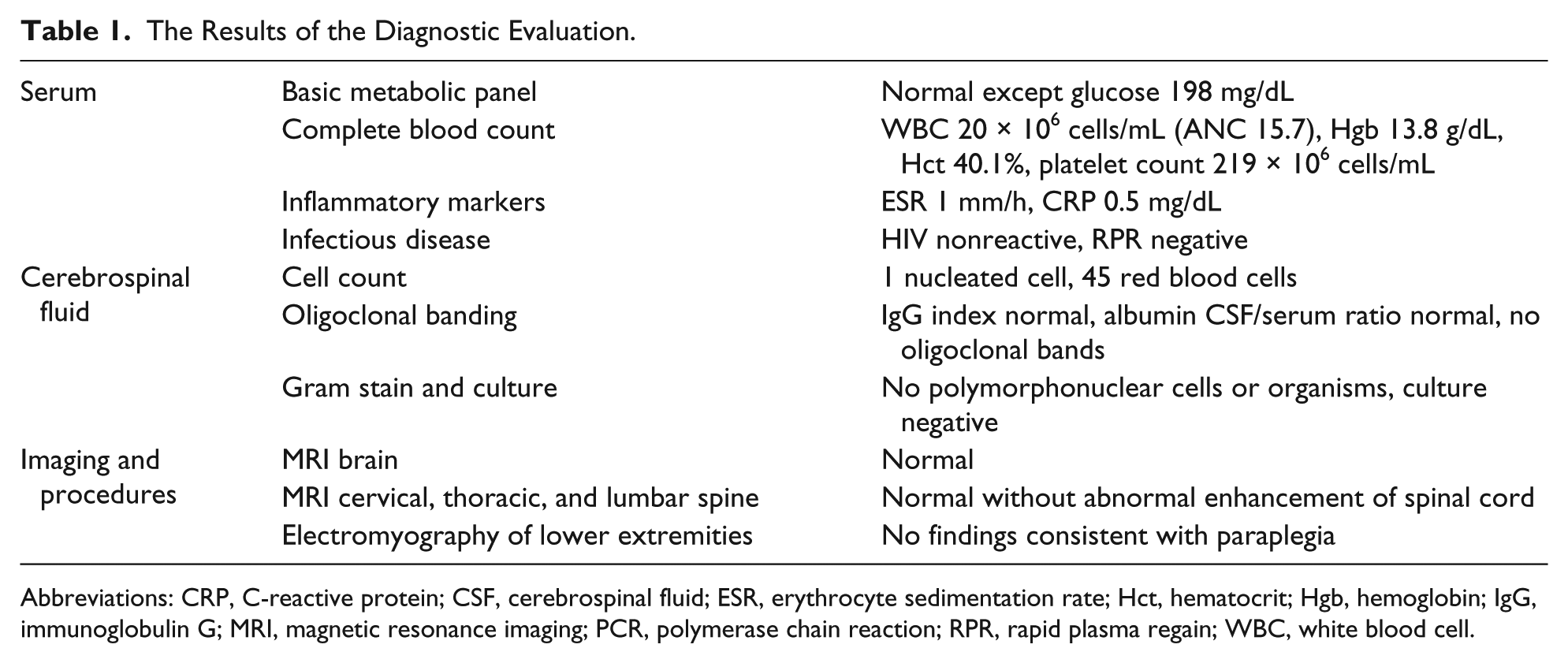
Abbreviations: CRP, C-reactive protein; CSF, cerebrospinal fluid; ESR, erythrocyte sedimentation rate; Hct, hematocrit; Hgb, hemoglobin; IgG, immunoglobulin G; MRI, magnetic resonance imaging; PCR, polymerase chain reaction; RPR, rapid plasma regain; WBC, white blood cell.
Hospital Course
The patient did not have progression of his sensory deficits or recurrence of respiratory distress. He was transferred out of the intensive care unit to the pediatric inpatient floor service. Brain and total spine MRI and lower extremity electromyography (EMG) did not reveal an etiology for his symptoms (Table 1). After this extensive negative evaluation, the possibility of a somatoform disorder was raised, and a pediatric psychologist was consulted. Prior to her assessment, the primary medical team recommended the patient be transferred to an inpatient rehabilitation facility. Less than one hour after the patient and his family were informed of this recommendation, the patient began to move his lower extremities and void spontaneously. During the subsequent psychology consultation, the patient revealed an extreme dislike and fear of spiders. He further identified frustration with the idea of being away from his girlfriend for several weeks to undergo rehabilitation as his motivation to move again. Based on this information, the inconsistencies in his physical examination, his rapid recovery of function, and the unrevealing workup, a diagnosis of conversion disorder was made.
Prior to discharge, the patient was evaluated by physical therapy and demonstrated normal gait and function for age. Repeat neurological examination showed 5/5 strength in all lower extremity muscle groups bilaterally with recovery of patellar and Achilles reflexes; this was an abrupt improvement from just a few hours prior. The patient was able to ambulate without assistance and reported no sensory abnormalities. He was encouraged to establish care with an outpatient mental health provider following discharge.
Final Diagnosis
Conversion disorder (functional neurologic symptom disorder)
Discussion
Neurologic concerns are common in the pediatric population and often present diagnostic conundrums. 1 Given the potential consequences of a delayed diagnosis, these patients frequently undergo an expensive, and at times invasive, inpatient evaluation. This patient’s case illustrates the challenge of differentiating an organic cause of neurological impairment from a somatoform disorder. In addition, it underscores the importance of a thorough social and psychiatric history and a detailed neurologic examination to ensure appropriate diagnostic evaluation, treatment, and follow-up.
Among children and adolescents, conversion disorder occurs most frequently in the peripubertal years. In a recent retrospective chart review of pediatric patients evaluated in the inpatient setting and diagnosed with a somatoform disorder, the majority were white, adolescent females. 2 Often they reported a current or past nonsomatoform psychiatric disorder and/or family history of mental illness. Traditionally, conversion disorder has been associated with a history of trauma, particularly sexual abuse, and low socioeconomic status,3,4 but more recent literature has suggested that this correlation may not be as strong as previously alleged. In fact, pediatric somatoform disorders may be more common in middle- and high socioeconomic classes, and trauma may play a role in only a minority of cases. 2 However, patients with conversion disorder do often report a history of physical or emotional stress, for example, parental separation, death of a relative or friend, peer relationship issues, or school stress.2,5-7 Although conversion reactions following a phobia-related event, as in the case of this patient, have not been described in the literature to our knowledge, simple and social phobias were documented as comorbid psychiatric illnesses in patients with conversion disorder described by Sar et al. 8
Many individuals with conversion disorder have multiple or mixed symptoms with pain and motor dysfunction being the most common. 2 In addition, they often have a physical illness and/or comorbid medical condition; thus, the presence of such does not exclude the possibility that somatization may be playing a role in the patient’s presenting symptoms. The physical examination is often key to the diagnosis; findings such as Hoover’s sign (weakness of hip extension when tested in isolation that resolves with testing of contralateral hip flexion), “give-way” weakness, bizarre gaits, normal reflexes, or reciprocal contraction during strength testing suggest a functional process.6,9,10 However, as demonstrated by this patient and a previous report, the absence of reflexes does not exclude the diagnosis of conversion disorder. 11 Management traditionally involves patient education, cognitive behavioral therapy, treatment of comorbid psychiatric illness, and physical therapy and rehabilitation for persistent deficits. Offering a psychological explanation early in the diagnostic evaluation may result in quicker patient and family engagement in such a multidisciplinary approach to treatment. 7
Interestingly, there is increasing evidence for a neuropsychological basis for conversion disorder, which functional MRI technology has helped to further define. As described in the thorough review by Vuilleumier, 12 in patients with conversion symptoms, there appears to be hyperactivity in the ventromedial prefrontal cortex and precuneus, both of which have been implicated in access to internal representations of the self and the integration of memory and sensory information. Increased activity has also been noted in limbic structures, which are known to play a role in emotion regulation and motivated behavior. In contrast, there is decreased recruitment of sensory pathways at the subcortical level. Taken together, these studies suggest that conscious sensorimotor function and self-awareness may be altered in those with conversion disorder, promoting different behavioral responses to emotional states compared with normal controls. 12
Conclusion
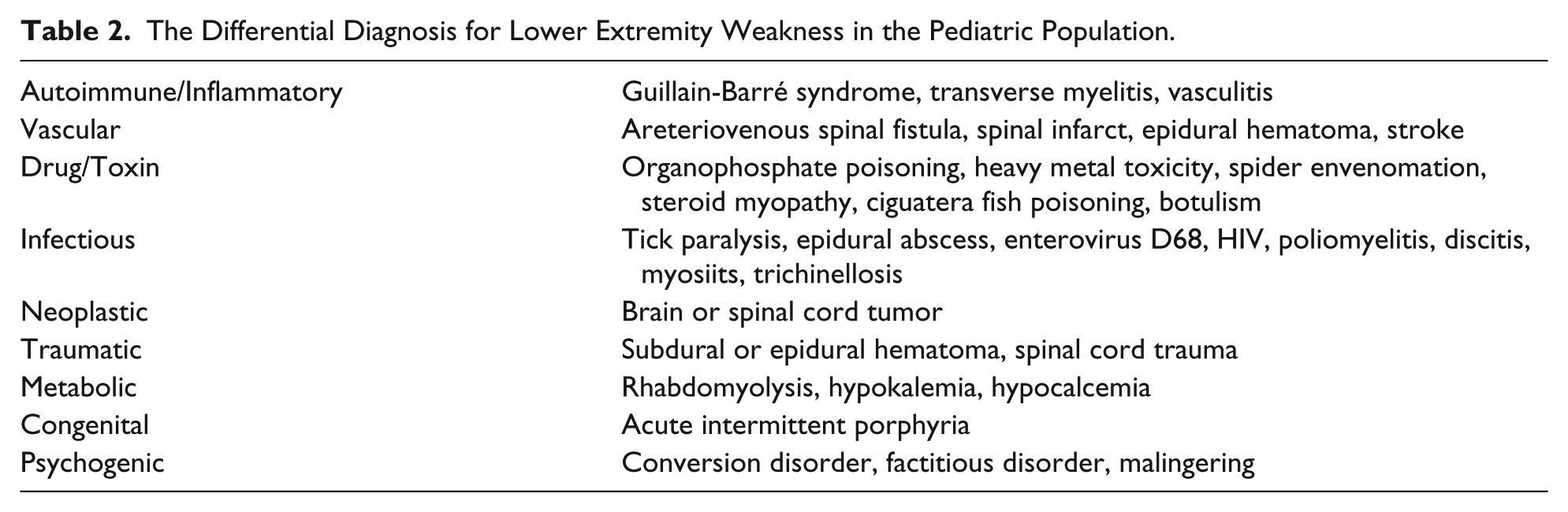
This patient presented with acute motor and sensory system dysfunction suggestive of both myelopathy and radiculopathy. The differential for such symptoms is broad and includes Guillan-Barré syndrome, spinal infarct, transverse myelitis, tick paralysis, organophosphate poisoning, and arteriovenous spinal fistula (Table 2). 13 However, in patients with unexplained neurologic symptoms, conversion disorder should be considered even in the presence of areflexia. Although often thought of as a diagnosis of exclusion, the DSM-5 (Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition) definition of conversion disorder emphasizes that the symptoms of “altered voluntary motor or sensory function” must be inconsistent with a known medical or neurological condition and cause distress or functional impairment. A thorough social and psychiatric history and detailed neurologic examination are integral to making this diagnosis and in some situations, may obviate the need for expensive testing. This patient underwent a thorough, at times invasive, evaluation, in addition to intubation and mechanical ventilation. A more thorough physical examination at initial presentation, including testing for Hoover’s sign, close observation of the patient’s physical abilities when not being formally examined, and assessment for demographic and psychosocial characteristics common in conversion disorder may have allowed this diagnosis to be made earlier. Although recent studies suggest a neurophysiologic basis for conversion symptoms, the condition remains poorly understood and challenging to diagnose and manage.
The Differential Diagnosis for Lower Extremity Weakness in the Pediatric Population.
Author Contributions
EJC and DLM designed, composed, and revised the manuscript. RBC, KMT, and BLJ contributed to interpretation of the case and revised the manuscript.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.